Aortic valve Libman‑Sacks endocarditis mimicking papillary fibroelastoma: therapeutic possibilities



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Aortic valve Libman‑Sacks endocarditis mimicking papillary fibroelastoma: therapeutic possibilities
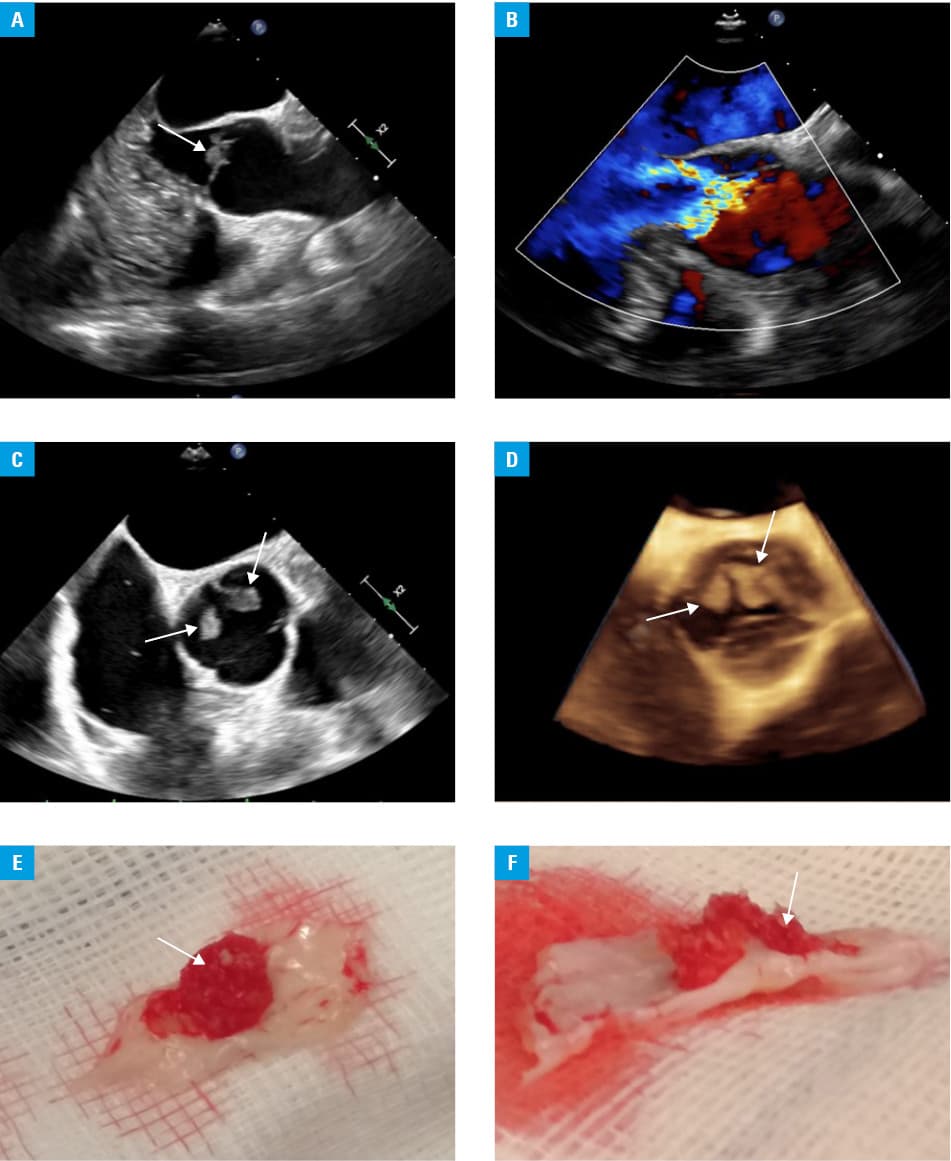
A 28‑year‑old man with antiphospholipid syndrome (APS) was admitted to the cardiac surgery department for a resection of a single tumor with papillary fibroelastoma morphology in the aortic leaflet, causing severe regurgitation. The patient suffered from right‑sided ischemic stroke (with resolving paresis of the left upper limb), thrombosis of the cerebral sinuses and the right internal jugular vein, as well as chronic renal failure, thrombocytopenia, hypertriglyceridemia, hypertension, and chronic hepatitis B. He was treated with dabigatran. Transesophageal echocardiography revealed 2 irregular, free‑floating structures with a length of 7 mm and 4 mm at the edges of the noncoronary and left coronary leaflets, with a moderate 2‑stream regurgitation (Figure 1A–1D). Laboratory results and the patient’s clinical condition did not reveal any signs of a systemic infection apart from a slightly elevated activity of liver enzymes typical of chronic hepatitis B. Due to a high risk of embolism and primary tumor suspicion, the patient was qualified for a cardiac surgery. The native aortic valve with 2 papillary tumors (Figure 1E and 1F) on the leaflets was removed through the upper ministernotomy, and a bioprosthesis (Inspiris Resilia Aortic Valve, Edwards Lifesciences; Irvine, California; United States) was implanted. The choice of the valve for the patient with anticardiolipin antibodies in the serum and a history of serious thromboembolic events was motivated by its lower thrombogenicity as compared with mechanical prostheses and a specific production technology that enables the use of the bioprosthesis in younger patients. Histopathological examination revealed fibrosis of one of the valve leaflets, while nodular lesions were identified as organizing thrombi. The postoperative period was uneventful. On transesophageal echocardiography no paravalvular leakage was observed and proper function of the valve was confirmed. After initiation of vitamin K antagonist, the patient was discharged in a good general condition.
Heart valve diseases associated with APS are found during transthoracic echocardiography in about one‑third of primary APS patients and are the most common cardiac manifestations of this disease.1 The lesions occur mainly on the mitral valve, less often on the aortic valve.1 In the presented case, the differential diagnosis took into account the most common noninfectious lesions in the aortic valve leaflets diagnosed in the general population, which include primary tumors, as well as more typical in APS nonbacterial, organized thrombus in the course of Libman‑Sachs endocarditis, and significantly less frequent thrombus on the aortic valve leaflets without a fibrin component.2,3 The differentiation process in the diagnosis of a hemodynamically stable patient is important due to sensitivity of an unorganized thrombus to the anticoagulant therapy, which enables a successful, conservative treatment, even though it does not exclude the possibility of a thromboembolic event in a markedly extended treatment.2 The effects of anticoagulants and glucocorticosteroids on the vegetations in Libman‑Sacks endocarditis require further research.1 Surgical treatment preferred in the valve dysfunction and high risk of embolism involves aortic valve replacement or, if possible, removal of the lesions and the native valve repair.4 The surgery is associated with an increased risk of bleeding or development of prosthetic valve thrombosis, minimized in some centers by replacing mechanical valves with aortic bioprostheses.1,5 In the context of these reports, the use of persistent biological valves with low thrombogenicity in young patients, even if the anticoagulant therapy is required as a secondary thromboembolism prophylaxis, may contribute to reducing the number of risk factors and obtaining good therapeutic outcomes, as in the described case.
- Kolitz T, Shiber S, Sharabi I, et al. Cardiac manifestations of antiphospholipid syndrome with focus on its primary form. Front Immunol. 2019; 10: 941. | Crossref
- Salzberg SP, Nemirovsky D, Goldman ME, Adams DH. Aortic valve vegetation without endocarditis. Ann Thorac Surg. 2009; 88: 267‑269. | Crossref
- Premyodhin N, Glovaci D, Azam S, et al. Distinguishing aortic valve thrombus from Libman‑Sacks endocarditis in antiphospholipid syndrome: imaging and management. Future Cardiol. 2021; 17: 101‑111. | Crossref
- Keenan JB, Rajab TK, Janardhanan R, et al. Aortic valve replacement for Libman‑Sacks endocarditis. BMJ Case Rep. 2016; 2016: bcr2016215914. Correction in: BMJ Case Rep. 2016; 2016: bcr2016215914corr1. | Crossref
- Colli A, Mestres CA, Espinosa G, et al. Heart valve surgery in patients with the antiphospholipid syndrome: analysis of a series of nine cases. Eur J Cardiothorac Surg. 2010; 37: 154‑158. | Crossref
ARTICLE INFORMATION