A 73‑year‑old man with a diagnosis of small lymphocytic lymphoma (2019) and colon cancer of the hepatic flexure (2020) was admitted to our department for the administration of the 12th cycle of adjuvant chemotherapy according to the FOLFOX‑4 regimen. Previously, he received 2 lines of treatment for small lymphocytic lymphoma and underwent adenoidectomy with bilateral tonsillectomy (2019). After right‑sided hemicolectomy with a resection of the terminal ileum and the 6th segment of the liver due to locally advanced G2 colorectal cancer (pT4bN2bM0; KRAS, NRAS, BRAF wild‑type), the adjuvant chemotherapy was initiated (2021).
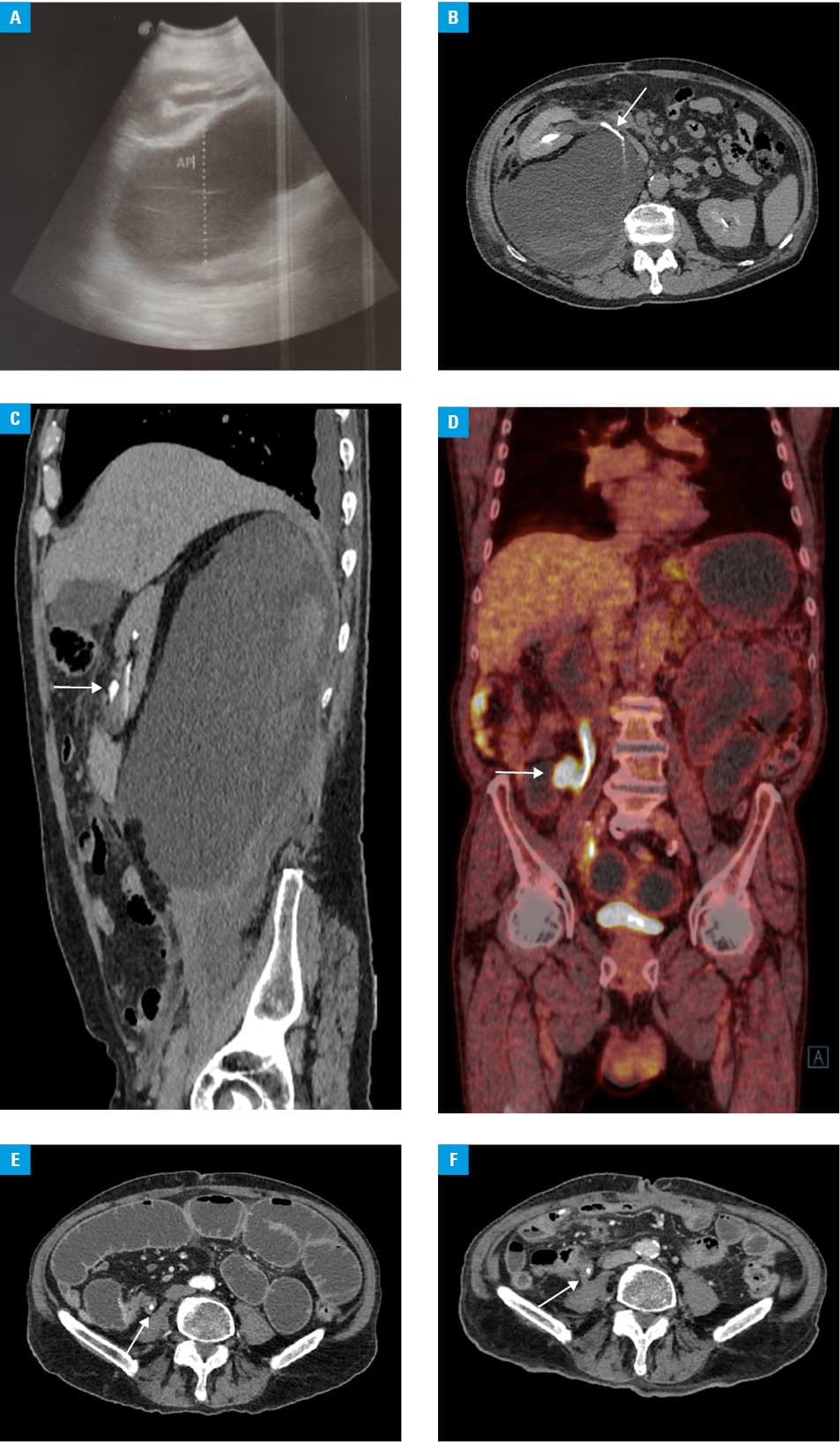
On admission, the patient reported nausea and severe colic pain in the right hypochondrium. Laboratory tests revealed moderately elevated levels of C‑reactive protein (44.0 mg/l; reference range, 0–5 mg/l); creatinine (88.2 µmol/l; reference range, 59–104 µmol/l), carcinoembryonic antigen (1.88 ng/ml; reference range, 0–5 ng/ml), and cancer antigen 19–9 (80.56 U/ml; reference range, 0–37 U/ml). Abdominal ultrasound revealed an undefined hypoechogenic structure in the retroperitoneal space (Figure 1A). Computed tomography (CT) performed on the same day visualized a spontaneous perforation of the right ureter with the formation of urinoma (Figure 1B and 1C). The patient was urgently transferred to the urology department, where the rupture was successfully treated with a D‑J probe (5 Fr) insertion and peritoneal cavity drainage. Positron emission tomography–CT (PET‑CT) was performed; however, the cause of the perforation remained unclear (Figure 1D). Two months later, the patient developed an obstruction of the small intestine requiring surgical intervention (Figure 1E). The surgeon found tumor infiltration in the retroperitoneal space covering the ureter and a part of the small intestine. Due to advanced stage of the disease, surgery was restricted to excision of the fragment of the intestine causing the obstruction, with restoration of the gastrointestinal tract continuity using side‑to‑side anastomosis. A retrospective analysis of CT images showed the presence of discrete changes in the retroperitoneal cavity on the right side, corresponding with tumor recurrence (Figure 1F).
Ureter perforation may cause urine collection in the retroperitoneum (urinoma) and, in the case of its infection, formation of an abscess with the risk of progression to urosepsis and acute renal impairment. In the majority of cases, the perforation is caused by obstructing ureteral stones and strictures of the ureter.1 The most common symptoms include severe, persistent lower abdominal pain with severe peritoneal irritation associated with nausea and vomiting.2
There are few reports of spontaneous ureteral rupture. Out of 119 cases available in the English medical literature, only 11 reported malignancy as the etiology. In contrast to our case, none of them was related to recurrence of another organ tumor.3,4
This unique case describes a spontaneous perforation of the ureter caused by its infiltration with recurrent colorectal cancer, which led to diagnostic difficulties despite the use of all available imaging methods. The presented clinical problem emphasizes the need to exercise criticism during the diagnostic work‑up with respect to the assessment of the results of imaging studies, including PET‑CT. To our best knowledge, the presented case is the first of its kind to be described.
- Choi SK, Lee S, Kim S, et al. A rare case of upper ureter rupture: ureteral perforation caused by urinary retention. Korean J Urol. 2012; 53: 131‑133. | Crossref
- Diamond DA, Marshall FF. The diagnosis and management of spontaneous rupture of the ureter. J Urol. 1982; 128: 808‑810. | Crossref
- Chen GH, Hsiao PJ, Chang YH, et al. Spontaneous ureteral rupture and review of the literature. Am J Emerg Med. 2014; 32: 772‑774. | Crossref
- Akpinar H, Kural AR, Tüfek I, et al. Spontaneous ureteral rupture: is immediate surgical intervention always necessary? Presentation of four cases and review of the literature. J Endourol. 2002; 16: 179‑183. | Crossref
ARTICLE INFORMATION