Atypical presentation of gastric adenocarcinoma secondary to Wilms tumor in a 32‑year‑old kidney transplant recipient



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atypical presentation of gastric adenocarcinoma secondary to Wilms tumor in a 32‑year‑old kidney transplant recipient
A 32‑year‑old kidney transplant recipient was admitted to the Department of Nephrology and Transplantation Medicine with acute, severe mid‑epigastric pain and fever of 38 ºC. At the age of 7 years, he had been diagnosed with Wilms tumor of the left kidney and subjected to nephrectomy followed by radiotherapy and chemotherapy (dactinomycin, vincristine, doxorubicin). Thirteen years later, a kidney transplantation had been performed, resulting in primary nonfunction. After 1 year, the patient had undergone a second, successful kidney transplantation.
Upon admission (11 years later), he presented with fever and tenderness in the epigastric region with elevated levels of C‑reactive protein (197 mg/l; reference range, 0–5 mg/l) and white blood cells (15.7 × 103/μl; reference range, 4–10 × 103/μl). Chronic immunosuppressive therapy consisted of tacrolimus (trough level, 6.78 ng/ml; reference range, 5.35–7.15 ng/ml), mycophenolate mofetil (1 g/d), and prednisone (5 mg/d). Initial ultrasonography showed extensive, pathological, multilocular cystic structures in the mid- and left epigastrium, measuring at least 11 × 14 cm. The structures were initially identified as fluid collections resulting from possible pancreatitis; however, laboratory markers of acute pancreatitis were absent (Figure 1A). A computed tomography (CT) scan confirmed the presence of fluid collections of approximately 14 × 9 × 8 cm, with no focal lesions (Figure 1B) and no abnormalities in the pancreas. The collections were most likely located within the peritoneum.
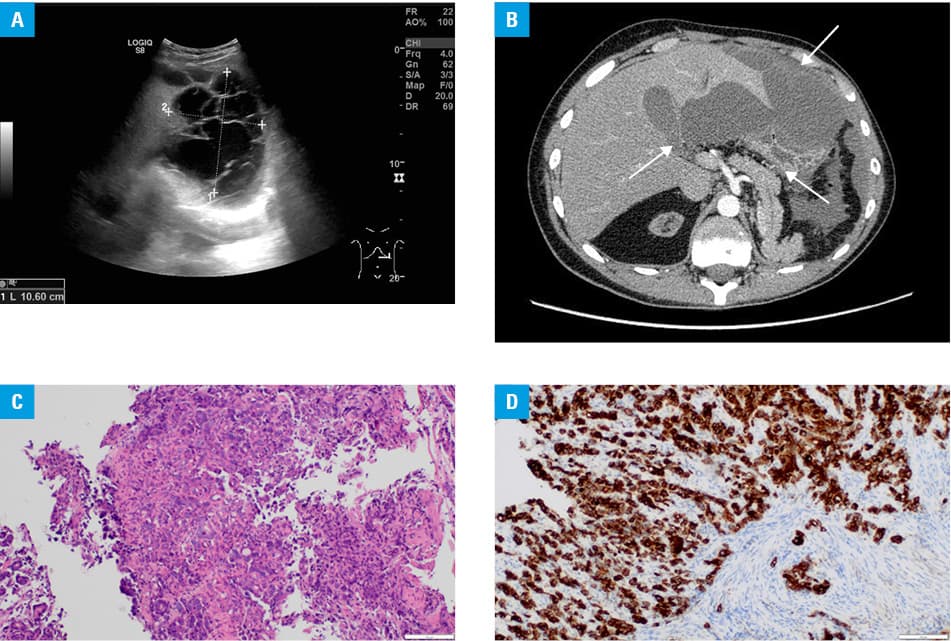
After a 10‑day antibiotic therapy with meropenem, the inflammatory markers returned to normal values and the abdominal fluid collections significantly decreased. Tests for Echinococcus granulosus / multilocularis were negative. Unfortunately, the epigastric pain did not alleviate. It was necessary to perform gastroscopy, which revealed a 7‑mm ulceration in the subcardial region of the stomach. Histopathological examination of the gastric biopsy specimen showed infiltration of poorly differentiated gastric adenocarcinoma (Figure 1C and 1D). The patient was referred for chemotherapy and discharged from the hospital. After 2 days, he was readmitted due to tachycardia and abdominal pain. A CT scan showed suspicious mediastinal lymph nodes measuring 6 mm and an encysted fluid collection of 7 × 8 × 3 cm in the abdominal cavity adjacent to the stomach. Positron emission tomography images confirmed peritoneal and lymph node metastases. Laboratory tests showed elevated levels of cancer antigen 125 and cancer antigen 19–9 but no increase in the carcinoembryonic antigen level. The presence of Epstein‑Barr virus and BK virus was excluded. The patient passed away within 4 months of preparation for chemotherapy.
The present case shows an example of a secondary malignant neoplasm (SMN), which develops within 20 to 30 years after the primary tumor in 5% to 15% of childhood cancer survivors.1 When taking into account only the patients who survived Wilms tumor, the risk of SMN ranges between 1.5% and 3.9%.2 Most frequently, the second neoplasm affects the digestive system, breasts and bones, as well as blood‑forming cells (leukemia).3 Standard treatment for Wilms tumor comprises chemotherapy (vincristine and actinomycin), radiotherapy, and nephrectomy.4 The risk factors for SMN include time since recovery from the tumor, doses of radiotherapy and chemotherapy, as well as the duration of immunosuppression.1 In this case, there were no typical symptoms of gastric cancer, such as weight loss, nausea, vomiting, anemia, hematemesis, or hematochezia.5 The relatively rapid progression of cancer with metastases in a young patient was unusual. This report highlights the need to pay special attention to kidney transplant recipients with nonspecific symptoms and abnormalities on imaging studies.
- Henderson TO, Oeffinger KC, Whitton J, et al. Secondary gastrointestinal cancer in childhood cancer survivors: a cohort study. Ann Intern Med. 2012; 156: 757‑260. | Crossref
- Lee JS, Padilla B, DuBois SG, et al. Second malignant neoplasms among children, adolescents and young adults with Wilms tumor. Pediatr Blood Cancer. 2015; 62: 1259‑1264. | Crossref
- Breslow NE, Lange JM, Friedman DL, et al. Secondary malignant neoplasms after Wilms tumor: an international collaborative study. Int J Cancer. 2010; 127: 657‑666. | Crossref
- Sosnowska‑Sienkiewicz P, Januszkiewicz‑Lewandowska D, Jończyk‑Potoczna K, et al. Therapeutic management in a child with Wilms tumour and radiological features suggesting rupture at the time of diagnosis. Pediatr Pol. 2021; 96: 288‑291. | Crossref
- Park JM, Choi MG, Yang CW, et al. Increased incidence of gastric cancer in renal transplant recipients. J Clin Gastroenterol. 2012; 46: 87‑91. | Crossref
ARTICLE INFORMATION