Adherence to prophylactic treatment in adult patients with severe hemophilia in Poland
Key words: hemophilia, Poland, prophylaxis, treatment adherence, VERITAS-Pro



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Adherence to prophylactic treatment in adult patients with severe hemophilia in Poland
Introduction: Patient adherence to a prophylactic regimen is important for optimal benefit of hemophilia treatment. Despite a growing number of adults with hemophilia in Poland receiving secondary prophylaxis, data on adherence to the regimen are limited.
Objectives: The aim of the study was to assess adherence to secondary prophylaxis in Polish adults with severe hemophilia.
Patients and methods: Patients were recruited in 18 hemophilia treatment centers in Poland. Adherence to prophylaxis was assessed with the Validated Hemophilia Regimen Treatment Adherence Scale Prophylaxis (VERITAS‑Pro) questionnaire.
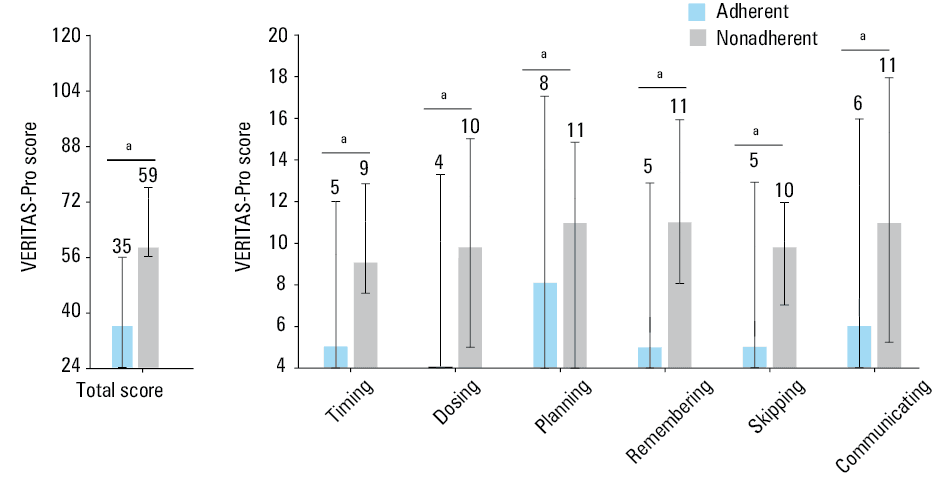
Results: Data on 270 men on the prophylactic regimen (median [interquartile range, IQR] age, 37 [18–75] years; mean [SD], 38.2 [13.3] years) were analyzed. Median (IQR) VERITAS‑Pro score for the study population was 36 (24–76) years; mean (SD), 37.7 (9.9) years, indicating general adherence to the prophylactic regimen. The median subscale scores ranged from 4 for Dosing to 8 for Planning (means, 5.6 and 7.7, respectively). The most pronounced difference in the subscale scores between adherent and nonadherent patients was recorded for Dosing (median, 4 vs 10; mean, 5.3 vs 9.3) and Remembering (median, 5 vs 11; mean, 5.7 vs 10.7). The overall adherence rate was 94%.
Conclusions: Our results show a high rate of adherence to hemophilia prophylaxis by Polish adults. Problems with the management of clotting factor stocks and remembering about the injection of the clotting factor were identified as potential barriers to adherence in adults with hemophilia in Poland.
What's new?
Home treatment and prophylaxis are the standard of care in severe hemophilia but data on their outcome in Poland are scarce. In particular, the available data on adherence to the prophylaxis in hemophilia are limited; no research has been conducted in Poland on this topic despite a continually growing access to prophylactic treatment. We present a large national study on this topic and discuss barriers to effective prophylactic regimen, which can improve effectiveness of hemophilia treatment in clinical practice.
Introduction
The standard hemophilia treatment includes prophylaxis with regular, continuous, intravenous injections of clotting factors concentrate.1 Well‑conducted prophylaxis contributes to the achievement of optimal treatment effects in children, adolescents, and adults.2-8
A prerequisite for the effective prophylaxis is largely the patient’s adherence to the prescribed treatment regimen. It was demonstrated that poor adherence had serious adverse effects on the disease outcome.6,8,9 Maintaining high adherence to the prescribed treatment is a challenge for patients with hemophilia due to the their lifestyle habits and perceptions of the disease, the disease severity, treatment, health care system, and socioeconomic factors.10-12 The multitude of elements determining adherence to the therapeutic recommendations may raise concerns about the possibility of meeting them by some patients. This may discourage physicians from prescribing prophylaxis and result in suboptimal treatment.13,14 Therefore, according to the recommendations,1 regular and standardized assessments of individual health status and outcomes are required to identify new or potential problems, so that treatment plans can be optimized. Evaluation of patients’ adherence to the prophylaxis should also be a part of this process.
Validated Hemophilia Regimen Treatment Adherence Scale Prophylaxis (VERITAS‑Pro) is a questionnaire designed to assess adherence to a prophylactic regimen in patients with hemophilia, suitable for use in clinical and research settings.15 The application of the cutoff points allows for the identification of nonadherent patients. Moreover, VERITAS‑Pro provides comprehensive insight into the nature of nonadherence by analyzing responsible factors. This measure has shown good reliability and validity in several populations of pediatric and adult hemophilia patients, for example, from the United States,15 Canada,16 Brazil,17 the Netherlands,18 and Spain.19
Hemophilia affects 1 in 12 300 Polish inhabitants.20 In 2008, the first therapeutic program in Poland for the prophylaxis of bleeding in children with hemophilia A and B was implemented. Under the current national health program, prophylactic treatment is available to children (since 2008) and adults (since 2012) with hemophilia. However, despite the growing number of Polish patients with hemophilia who receive prophylactic treatment, the available data on their adherence to the prophylaxis are limited.20
Hemophilia care in Poland is coordinated by Hemophilia Treatment Centers (HTCs), which are part of the regional hematology departments or clinics. Clotting factor concentrates are stored and distributed for home treatment and hospital use by the regional blood banks.
The aim of the study was to assess the adherence to the prophylactic regimen by Polish adult patients with severe hemophilia using the VERITAS‑Pro.
Patients and methods
Participants
A total of 34 hematologists were asked to invite approximately 15 consecutive adult patients with hemophilia A or B (with or without an inhibitor), who attended their routine visit at a hematologic outpatient clinic. Seven physicians resigned and 27 completed the project, each recruiting 2 to 43 patients (depending on the site capacity). All patients were asked to complete a survey that included clinical data (disease type, inhibitor presence, information about drug administration) and socio‑demographic characteristics (age, body mass, employment status), and also to complete the VERITAS‑Pro questionnaire. All clinical data were verified by a physician. According to Polish regulations, such surveys are neither clinical studies nor medical experiments, and the approval of the Ethics Committee is not required. Written informed consent was obtained from all patients.
Measure
The VERITAS‑Pro scale was used to quantify the adherence to prophylactic treatment regimen (with permission from the Indiana Hemophilia and Thrombosis Center, Indianapolis, Indiana, United States).21 The Veritas‑Pro scale is a 24‑item questionnaire divided into 6 subscales. The Timing subscale provides information on taking the clotting factor as scheduled, Dosing refers to the administration of the prescribed dose, Planning assesses the organization of clotting factor supplies, Remembering informs about missed infusions, Skipping refers to doses intentionally not taken, and Communicating evaluates communication with the treatment center at appropriate times. Each subscale contains 4 items. Response options are presented as a 5‑point Likert scale ranging from “always” to “never”. The direction of responses is different in different items, that is, “always” may reflect the best or the worst possible adherence, depending on the item. The response indicating the best adherence (either “always” or “never”) is coded as 1 and the response indicating the worst adherence (also “always” or “never”) is coded as 5, and therefore a higher number denotes worse adherence. The total score ranges from 24 to 120, and the subscale scores range from 4 to 20. A total score equal to or above 57 points indicates overall nonadherence and a subscale score equal to or above 11, 7, 9, 11, 11, and 10 indicates nonadherence for Timing, Dosing, Planning, Remembering, Skipping, and Communicating, respectively.15
The VERITAS‑Pro scale was translated into Polish by an experienced translator under the supervision of a group of experts selected from HTCs in Poland and in close cooperation with the developer of the scale, that is, the Indiana Hemophilia and Thrombosis Center.
Statistical analysis
Descriptive statistics were computed for analyzed parameters as appropriate (mean with SD for parameters with normal distribution or median and interquartile range [IQR] for parameters with non normal distribution). The analysis of the VERITAS‑Pro scale was performed for the entire survey (total score) and for each subscale (subscale scores). As the distribution of variables from the VERITAS‑Pro scale was not normal (the Shapiro–Wilk test), nonparametric tests were used in further analyses. Comparisons between groups were done using the Mann–Whitney test, the Kruskal–Wallis test, and the χ2 test. Statistical significance was set to P below 0.05. Statistical analyses were carried out using the IBM SPSS Statistic version 24 (IBM, Armonk, New York, United States). Additionally, the means have been included to facilitate the comparison of our results with those from other studies.
Results
Survey administration
The survey was conducted between July and October 2018. Finally, 27 hematologists from 18 HTCs in Poland participated in the study. They recruited a total of 400 patients and the number of patients enrolled by a single specialist ranged from 2 to 43, depending on the recruitment possibilities of the medical facility.
Patient characteristics
From a total number of 400 patients who participated in the survey, 1 was excluded due to poor quality of the data, hence the questionnaires of 399 patients were suitable for analysis. Since not all patients provided all the required data, the number of patients included in each analysis was given.
The study group consisted of 270 men with severe hemophilia receiving prophylactic treatment at the study entry, and 129 patients treated on demand. Most patients on prophylaxis had hemophilia A without an inhibitor, followed by those with hemophilia B without an inhibitor, hemophilia A with an inhibitor, and hemophilia A with inhibitor status unknown. Regarding treatment administration, the vast majority of patients self‑administered the drug and most of them noted each dose in their diary. Most patients with hemophilia A, both with and without an inhibitor, administered prophylactic treatment (either factor VIII concentrate or activated prothrombin complex concentrate) 3 times a week, whereas the majority of patients with hemophilia B infused factor IX concentrate twice a week. Professional activity was reported mainly as employed, student, or learner. Detailed characteristics of the study population are presented in Table 1.
Parameter | Value | ||||
Whole population (n = 270)a,b | |||||
Data are presented as number (percentage of patients) unless indicated otherwise.
a Descriptive parameters for self‑administration of the drug were calculated for n = 270.
b n = 266 for age, body mass, and BMI due to missing data
c Due to the small size of the group (n = 5), the patients with hemophilia A with unknown inhibitor status were excluded from this analysis.
Abbreviations: BMI, body mass index | |||||
Age, y | Median (range) | 37 (18–75) | |||
Mean (SD) | 38.2 (13.3) | ||||
Body mass, kg | Median (range) | 80 (50–126) | |||
Mean (SD) | 81.8 (13.8) | ||||
BMI, kg/m² | Mean (SD) | 25.80 (4.02) | |||
Self‑administration of the drug | Yes | 243 (90) | |||
No | 24 (9) | ||||
No data | 3 (1) | ||||
Category | Whole population (n = 270)c | Hemophilia A without an inhibitor (n = 202) | Hemophilia B without an inhibitor (n = 34) | Hemophilia A with an inhibitor (n = 29) | |
Drug application diary | Yes, I make a note of every dose | 195 (72) | 150 (74) | 23 (68) | 18 (62) |
I note some of the doses | 37 (14) | 28 (14) | 5 (15) | 4 (14) | |
I don’t keep a diary | 36 (13) | 24 (12) | 4 (12) | 7 (24) | |
No data | 2 (1) | 0 | 2 (6) | 0 | |
Frequency of the agent administration | 3 times a week | 132 (49) | 108 (53) | 4 (12) | 17 (58) |
2 times a week | 81 (30) | 51 (25) | 23 (68) | 5 (17) | |
Every other day | 23 (9) | 22 (11) | 1 (3) | 0 | |
Every third day | 10 (4) | 8 (4) | 1 (3) | 1 (3) | |
Once a week | 15 (6) | 7 (3) | 5 (15) | 3 (10) | |
2–3 times a week | 2 (1) | 2 (1) | 0 | 0 | |
Every 3–4 days | 1 (0.37) | 1 (0.49) | 0 | 0 | |
Other | 5 (2) | 3 (1) | 0 | 2 (7) | |
No data | 1 (0.37) | 0 | 0 | 1 (4) | |
The assessment of adherence to prophylaxis was carried out in a sample of 262 patients with hemophilia, after excluding the individuals who did not provide data regarding all VERITAS‑Pro subscales.
VERITAS‑Pro scores in the whole study population
The total VERITAS‑Pro score and the subscale scores for the entire study population are presented in Table 2. The median score for the study population was 36 (IQR, 24–76; mean, SD 37.7 [9.9]). This result indicates good adherence to the prophylactic regimen in general. The median subscale scores ranged from 4 for Dosing to 8 for Planning (means, 5.6 and 7.7, respectively), indicating that the patients reported the highest adherence to the recommendations for administering the correct clotting factor dose and injecting as scheduled, and the lowest for the organization of drug stocks.
Score | Whole population (n = 262)a | Hemophilia A without an inhibitor (n = 199) | Hemophilia B without an inhibitor (n = 33) | Hemophilia A with an inhibitor (n = 26) | |
a Due to the small size of the group (n = 5), the patients with hemophilia A with unknown inhibitor status were excluded from this analysis. | |||||
Total score | Median (range) | 36 (24–76) | 36 (24–65) | 35 (24–59) | 34 (24–76) |
Mean (SD) | 37.7 (9.9) | 37.5 (9.3) | 39.0 (11.0) | 38.6 (13.1) | |
P value | – | 0.92 | |||
Timing | Median (range) | 5 (4–13) | 5 (4–12) | 6 (4–12) | 5.5 (4–13) |
Mean (SD) | 6.0 (2.3) | 5.9 (2.2) | 6.4 (2.3) | 6.5 (2.8) | |
P value | – | 0.40 | |||
Dosing | Median (range) | 4 (4–15) | 4 (4–15) | 5 (4–11) | 4 (4–10) |
Mean (SD) | 5.6 (2.1) | 5.6 (2.2) | 5.9 (2.1) | 5.2 (2.0) | |
P value | – | 0.32 | |||
Planning | Median (range) | 8 (4–17) | 8 (4–17) | 8 (4–15) | 8 (4–15) |
Mean (SD) | 7.7 (2.9) | 7.6 (2.8) | 8.1 (2.9) | 8.0 (3.2) | |
P value | – | 0.81 | |||
Remembering | Median (range) | 5 (4–16) | 5 (4–16) | 4 (4–13) | 5 (4–12) |
Mean (SD) | 6.0 (2.4) | 5.9 (2.3) | 6.4 (2.9) | 6.3 (2.7) | |
P value | – | 0.76 | |||
Skipping | Median (range) | 5 (4–13) | 5 (4–12) | 5 (4–13) | 4 (4–12) |
Mean (SD) | 5.7 (2.1) | 5.7 (2.0) | 6.2 (2.6) | 5.5 (2.4) | |
P value | – | 0.25 | |||
Communicating | Median (range) | 6 (4–18) | 6 (4–16) | 5 (4–15) | 6 (4–18) |
Mean (SD) | 6.8 (3.0) | 6.9 (3.0) | 6.1 (3.0) | 7.1 (3.4) | |
P value | – | 0.25 | |||
Adherence rate, % | 94 | 95 | 94 | 88 | |
P value | – | 0.41 | |||
VERITAS‑Pro scores in patients with different adherence status
Patients identified as adherent (ie, those who achieved a total VERITAS‑Pro score <57) were significantly different from those identified as nonadherent with respect to total and all subscale scores, (P <0.001) (Figure 1). The adherent patients had a median score of 35 (IQR, 24–56; mean, 36.3; n = 247), and the nonadherent patients reached the median score of 59 (IQR, 57–76; mean, 61.4; n = 15). The nonadherent group exceeded the cutoff for Dosing, Planning and Communicating. However, in both patient groups (adherent and nonadherent) there were individuals who exceeded the cutoff for either subscale, indicating nonadherence. The most pronounced difference in the subscale scores between the adherent and nonadherent patients was recorded for Dosing (median, 4 vs 10; mean, 5.3 vs 9.3) and Remembering (median, 5 vs 11; mean, 5.7 vs 10.7), and the smallest difference was noted for Planning (median, 8 vs 11; mean, 7.5 vs 11.0). These results suggest that remembering the injection of the clotting factor is difficult, especially for the nonadherent group, but that the organization of the clotting factor stocks poses a problem for both the adherent and nonadherent groups.
VERITAS‑Pro scores in patients with various types of hemophilia
The medians of total score did not differ significantly between the patients with different types of hemophilia (Table 2). The patients with hemophilia A without an inhibitor had a median score of 36, the patients with hemophilia A with an inhibitor 33.5, and the patients with hemophilia B without an inhibitor 35 points. The narrowest range of total score was reported in the patients with hemophilia B without an inhibitor (24–59), followed by the patients with hemophilia A without an inhibitor (24–65). The widest range was seen in the patients with hemophilia A with an inhibitor (24–76). The scores for the subscales also did not differ significantly between the patient groups and did not exceed cutoffs for nonadherence. Among the subscales, the highest median score was obtained for Planning (8) in all 3 groups of patients. Due to the small size of the group, the patients with hemophilia A with unknown inhibitor status were excluded from this analysis. Table 2 contains means of the above analyzed variables.
VERITAS‑Pro scores in patients of different age categories
The total VERITAS‑Pro score did not differ significantly between patients assigned to different age categories (Table 3). The median score ranged from 33 (IQR, 24–65) for the patients aged 50–59 years to 37 (IQR, 24–63) for patients aged 30–39 years, indicating good overall adherence. All patients aged 60 and older adhered to the prophylactic regimen but some patients assigned to other age categories exceeded the cutoff representing nonadherence. Table 3 contains means of the above analyzed variables.
Age category, y | n (%) | Median (range) | Mean (SD) | P value |
18–29 | 76 (29) | 36 (24–76) | 38.1 (9.8) | 0.86 |
30–39 | 69 (27) | 37 (24–63) | 38.0 (10.8) | |
40–49 | 61 (24) | 36 (24–65) | 37.7 (9.5) | |
50–59 | 33 (13) | 33 (24–65) | 35.9 (9.1) | |
≥60 | 19 (7) | 36 (25–53) | 37.0 (8.8) |
VERITAS‑Pro scores in patients of different occupational status
We did not find significant differences in the total VERITAS‑Pro score between the patients of different occupational status (Table 4). The median score calculated for the employed / students / learners was 36.0 (IQR, 24–76; mean, [SD] 38.1 [10.3]; n = 174), and for the unemployed it was 34 (IQR, 24–59; mean, [SD] 36.7 [9.0]; n = 74). The total score ranged from 24.0 (in both groups) to 76.0 (for the employed / students / learners), and 59.0 (for the unemployed), indicating that there were nonadherent patients in both analyzed groups. However, when analyzing the subscales, the unemployed group scored significantly lower on the Remembering scale (median, 4.0) than the employed / student / learner group (median, 5.0), which reflects less difficulty with remembering about the injection in this subpopulation (P = 0.021). Mean scores on Remembering were 5.4 and 6.2, respectively (Table 4).
Score | Employed / student / learner (n = 174) | Unemployed (n = 74) | P value | ||
Median (range) | Mean (SD) | Median (range) | Mean (SD) | ||
Total score | 36.0 (24–76) | 38.2 (10.2) | 34.0 (24–59) | 36.7 (9.0) | 0.37 |
Timing | 5.0 (4–13) | 6.1 (2.3) | 5.0 (4–12) | 5.9 (2.1) | 0.68 |
Dosing | 5.0 (4–15) | 5.7 (2.3) | 4.0 (4–11) | 5.3 (1.9) | 0.21 |
Planning | 8.0 (4–17) | 7.6 (2.9) | 8.0 (4–15) | 8.0 (2.7) | 0.25 |
Remembering | 5.0 (4–16) | 6.2 (2.5) | 4.0 (4–13) | 5.4 (2.1) | 0.02 |
Skipping | 5.0 (4–12) | 5.8 (2.2) | 4.0 (4–13) | 5.4 (2.1) | 0.09 |
Communicating | 6.0 (4–18) | 6.8 (3.0) | 6.0 (4–15) | 6.7 (3.1) | 0.55 |
Adherence rate, % | 93 | 97 | – | ||
Additionally, the evaluation of VERITAS‑Pro scores was performed in the subgroups of patients derived by combining such variables as age and occupational status (Table 5). The highest outcomes were obtained by patients above 60 years who were employed / students / learners (median, 41.0 [IQR, 33–42]; mean, [SD] 39.3 [4.3]) and the lowest result was noted for the unemployed young patients (median, 31.0 [IQR 24–76]; mean, [SD], 34.4 [7.6]). No significant difference was found in total VERITAS‑Pro scores between the subgroups of employed / students / learners (P = 0.80) and unemployed (P = 0.93) patients grouped by age.
Age category, y | Occupational status | Patients, n | Median (range) | Mean (SD) | P value |
18–29 | Employed / student / learner | 63 | 37 (29–50) | 38.6 (10.1) | 0.30 |
Unemployed | 7 | 31 (24–76) | 34.4 (7.6) | ||
30–39 | Employed / student / learner | 52 | 37,5 (24–58) | 37.4 (10.6) | 0.71 |
Unemployed | 14 | 35 (24–56) | 38.4 (10.7) | ||
40–49 | Employed / student / learner | 39 | 36 (24–65) | 38.0 (9.6) | 0.67 |
Unemployed | 20 | 36 (24–59) | 37.6 (9.7) | ||
50–59 | Employed / student / learner | 14 | 32.5 (34–65) | 36.6 (11.5) | 0.92 |
Unemployed | 17 | 33 (25–47) | 35.1 (7.3) | ||
≥60 | Employed / student / learner | 4 | 41 (33–42) | 39.3 (4.3) | 0.87 |
Unemployed | 13 | 36 (25–53) | 37.1 (10.1) |
Discussion
The assessment and monitoring of adherence to therapeutic recommendations allow for optimization of prophylaxis and increasing therapeutic benefits for the patients.6,8,22
However, there are still limited data on adherence to secondary prophylaxis in adults with hemophilia. This assessment is mainly based on the analysis of data from visual analogue scales or questionnaires completed by patients, interviews with patients conducted by doctors / nurses, injection logs, pharmacy logs, and medical records. With such a wide variety of data sources, the estimated level of adherence to hemophilia prophylaxis varies significantly depending on the tool used. Hence, the adherence rate in adult hemophilia patients can range from 39% to 82%.23-26
In this study, we used a validated measure, the VERITAS‑Pro questionnaire, to provide data on adherence to prophylaxis in Polish adults with hemophilia. As the distribution of VERITAS‑Pro results in our population was not normal, we presented results as medians and IQRs. To enable data comparison with other publications, we also reported means and SD.
We noted a median score of 36 points with the cutoff value of 57. A mean score of 37.7 points in our study reflected higher adherence than that obtained by Duncan et al27 for adults in the United States (total score 45.8).27 However, the study by Duncan et al27 included only 23 adults, who were also ethnically heterogeneous. The higher total VERITAS‑Pro score (50.8), which reflected lower adherence, was also reported by Krishnan et al,8 who studied 55 adult patients on continuous prophylaxis from the United States, Canada, and Australia. However, the limitation of both abovementioned studies was the lack of stratification of the adult patients by age. In general, better adherence is noted in younger patients with prescribed prophylaxis, in whom the treatment is administered by their parents. After childhood, the adherence declines with age.27,28 However, a recent study showed an increase in adherence in elderly patients (≥60 years) as compared with those aged 20–59 years.29 We found no significant differences in the total score between the age groups, although the patients aged 50–59 scored slightly lower than all the other age groups. The total score for patients aged 18–29 was comparable to the results calculated by Miesbach et al.30 Regarding the subscales, the entire study population obtained the lowest results in the Dosing and Skipping, and the highest in the Planning subscale. These findings suggested that the patients generally administered the scheduled dose but had problems with organization of their clotting factor stocks. As home deliveries were not available in Poland at the time of the study, the need for personal collection and transportation of the factor concentrate from a blood bank might have posed a barrier, especially for elderly or immobilized patients.
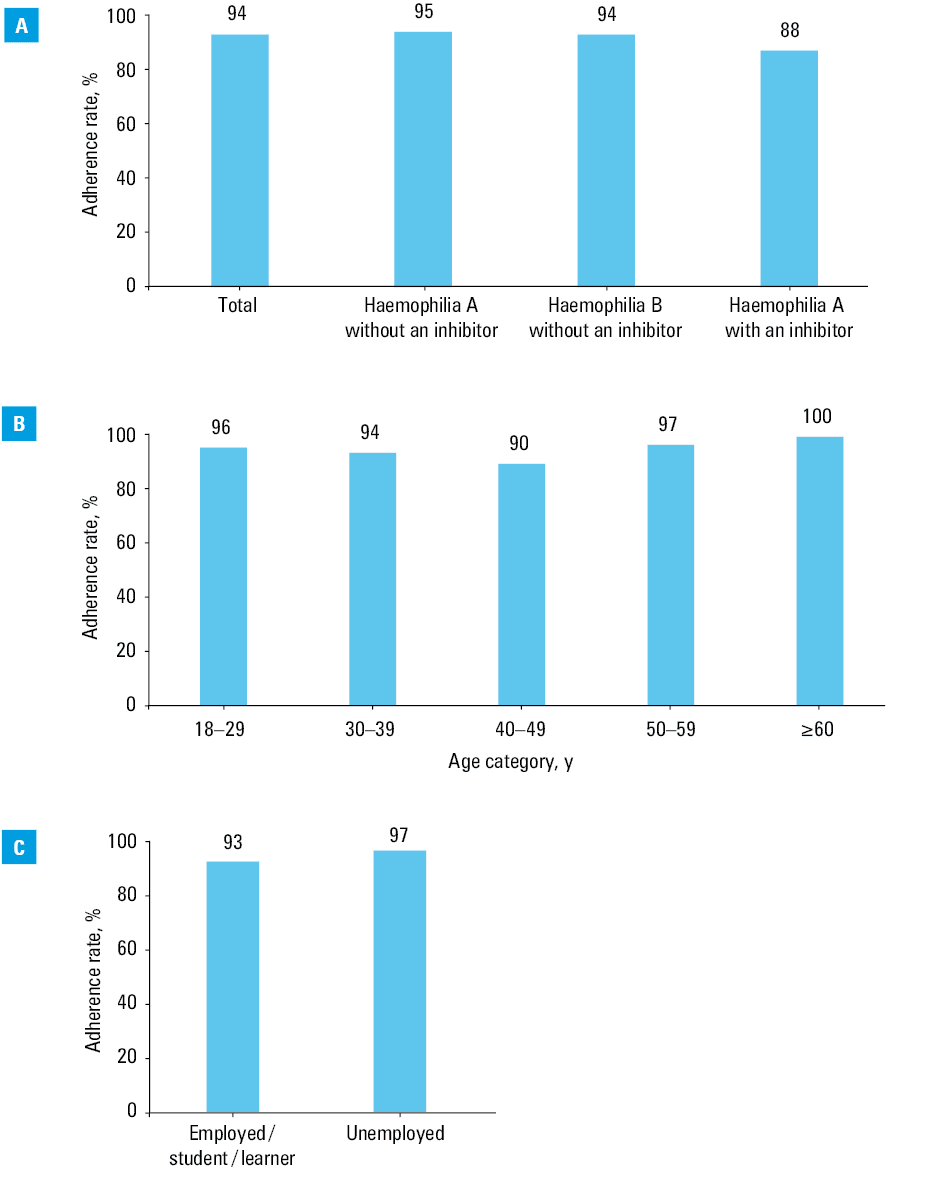
In our study population, 94% of patients adhered to the prophylactic regimen. The lowest adherence rate was observed in the patients with hemophilia A with an inhibitor (88%), as compared with those with hemophilia A (95%) or B without an inhibitor (94%) (Figure 2A). When analyzed by age, the lowest adherence rate was found in the patients aged 40–49 (90%), and the highest in those aged 60 years or over (100%) (Figure 2B, Table 5). However, these differences did not reach statistical significance. Comparable values of the adherence rate were found in the patients of different occupational status: 93% in the employed / student / learner group, and 97% in the unemployed group (Figure 2C). The study did not reveal differences in adherence rate between the patients who self‑administered the drug (94%) and those who needed assistance (96%).
Mean scores of VERITAS‑Pro in all cited studies were below the cutoff value and the lowest (42.0) was observed in the Croatian / Slovenian population29, followed by Spanish (42.6)28 and United States (45.8)27 groups, with the highest for Australian / Canadian / United States (50.8) population.8 Only 1 available study presented VERITAS‑Pro scores as medians—it concerned a relatively large German population, and the median score was 38 for the patients aged 20–59, and 32 for the patients above 60 years old.30 We did not observe such a big difference between median scores in the patients stratified by age, but we noted the highest adherence rate in patients above 60 years as well.
In addition to having difficulty managing the clotting factor stocks, the nonadherent patients also scored above the Dose and Communication cutoffs, indicating problems with administering the prescribed dose and communicating with a HTC. The most noticeable difference in subscale scores between the adherent and nonadherent patients was recorded for Remembering, indicating that unintentional omission of an injection can also be an important determinant of adherence. The adherence rate in our patients was higher than that calculated with VERITAS‑Pro for a Spanish population (71%).19 However, the Spanish sample also included adolescents. Another Spanish population study conducted only in adult patients showed a higher adherence rate of 82.5%.28 The adherence rate in our study was also higher than that obtained for the Croatian / Slovenian population (83%),29 but comparable to that for the German patients with hemophilia (93.1%).30
Interestingly, all patients aged 60 and over adhered to the prophylactic regimen. A similar phenomenon was observed in the German population.30 The results of studies conducted by Miesbach et al30 indicate that among patients older than 20, the adherence rate was the lowest in those aged 40–59 years, while the elderly perticipants (ie, ≥60 years) were characterized by a high adherence rate (93.9%). It has been suggested that high adherence to the prophylaxis in the elderly patients can be associated with an increased percentage of people experiencing pain in this age group.29
High adherence to the prophylaxis found in this study should be discussed considering patient characteristics and the hemophilia treatment policy in Poland. Our patients had advanced arthropathy and have only been able to benefit from a widely available secondary prophylaxis for 6 years now. It can therefore be assumed that our patients had high expectations regarding prophylaxis, guided by the awareness of the risk of deteriorating health. This is in line with research showing that experiencing symptoms and having a strong belief in the need for treatment are the motivators for adherence to treatment.10,31,32 Consequently, we studied a selected, highly cooperative population of adults.
In our study, the adherence rate did not differ significantly between patients with different types of hemophilia (A, B, or A with an inhibitor), which is consistent with the results obtained by others.19 Again, the Planning subscale scored higher in all 3 patient groups than the other subscales, indicating that drug stock management can be a barrier to adherence, regardless of the type of hemophilia. There are data indicating that some components of the adherence may be influenced by the nature of the patient activity, including occupational status.19 In our study, being employed or being a student / learner was associated with more frequent unintentional omission of a clotting factor injection.
Our study had several limitations that should be acknowledged. Although the VERITAS‑Pro scale was translated into Polish by a panel of experts, its assessment by the respondents was not carried out. A second limitation may be a skewed distribution of the VERITAS‑Pro scores, as most patients reported very good adherence, but our results for total score and subscale scores for the whole study population were comparable with those obtained by Miesbach et al.30 Another limitation was the fact that the patients self‑reported the data. The data were collected once and provided by the patient only, which may potentially result in a recall bias. Another limitation to mention was the lack of objective control measure that could be performed by extracting data from patient administration logs or the General Adherence Rating (GAR) scale.15 However, both instruments, that is, the GAR and patient administration logs also provide self‑rated data on the patient adherence. In addition, such analyses had been performed previously and revealed moderate‑to‑strong correlation of the VERITAS‑Pro total score with GAR results obtained from primary infusers and from medical staff, as well as with percentage of recommended infusions administered.15
Conclusions
In summary, our study provided the first data on adherence to hemophilia secondary prophylaxis in a Polish national sample using VERITAS‑Pro. The results of this study encourage further research on adherence to prophylaxis in adults and children with hemophilia in Poland using this validated tool as a measure. An important issue to be investigated is the assessment of the relationship between the adherence and the disease outcomes in Polish patients with hemophilia.
The results of this study showed a high rate of adherence to the prophylactic regimen by Polish adults with hemophilia, which may be a consequence of enabling universal access to prophylaxis and building the HTC network. Our results also indicate problems with the management of clotting factor stocks and remembering about the injection of the clotting factor as potential barriers to adherence to prophylaxis in Poland.
- Srivastava A, Brewer AK, Mauser‑Bunschoten EP, et al. Treatment Guidelines Working Group on Behalf of The World Federation of Hemophilia. Guidelines for the management of hemophilia. Haemophilia. 2013; 19: e1‑e47. | Crossref
- Manco‑Johnson MJ, Abshire TC, Shapiro AD, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007; 357: 535‑544. | Crossref
- Collins P, Faradji A, Morfini M, et al. Efficacy and safety of secondary prophylactic vs. on‑demand sucrose‑formulated recombinant factor VIII treatment in adults with severe hemophilia A: results from a 13‑month crossover study. J Thromb Haemost. 2010; 8: 83‑89. | Crossref
- Hay CR. Prophylaxis in adults with haemophilia. Haemophilia. 2007; 3 (Suppl 2): 10‑15. | Crossref
- Tagliaferri A, Franchini M, Coppola A, et al. Effects of secondary prophylaxis started in adolescent and adult haemophiliacs. Haemophilia. 2008; 14: 945‑951. | Crossref
ARTICLE INFORMATION