In search of “red flag” symptoms accompanying spinal pain in diffuse large B‑cell lymphoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
In search of “red flag” symptoms accompanying spinal pain in diffuse large B‑cell lymphoma
A 34‑year‑old man presented to his general practitioner (GP) with lumbosacral back pain. Due to his underlying illnesses (type 2 diabetes and obesity) he was advised to lose weight. Abdominal ultrasound showed no abnormalities.
During the next month, his pain worsened despite losing 3 kg of weight. He also developed paresthesia in digits 2 and 4 of his left hand.
In the presence of these new symptoms, he self‑referred for an orthopedic consultation. X‑ray and magnetic resonance imaging of the cervical spine revealed multilevel lesions suggestive of a hematologic disorder. Two months later, the patient presented to the emergency department with worsening back pain and reported episodes of low‑grade fever (up to 38 °C) and excessive sweating. On physical examination there was no lymphadenopathy or hepatosplenomegaly. No changes were detected in the blood smear. The patient was admitted to the internal medicine department for further diagnostic evaluation.
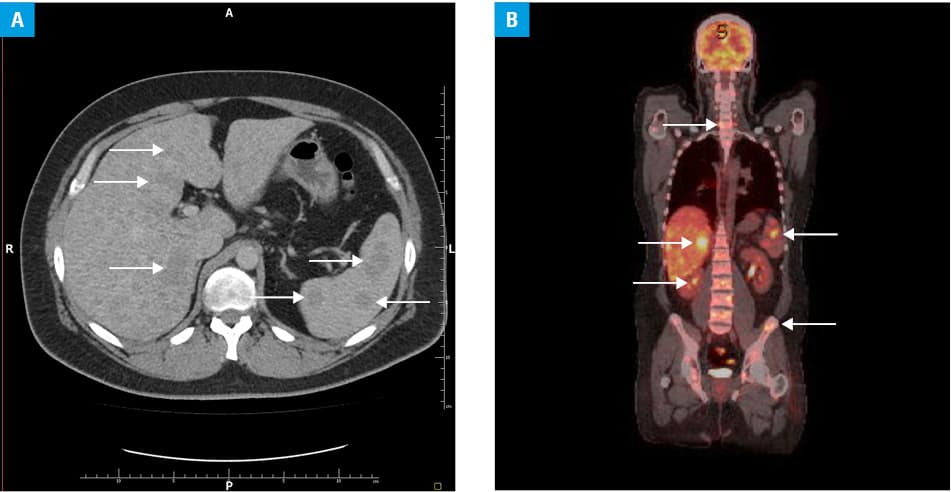
Ultrasound scanning and computed tomography (CT) showed lesions suggestive of metastases in the liver and spleen (Figure 1A) and numerous lung nodules bilaterally with enlarged mediastinal lymph nodes. Positron emission tomography‑CT revealed abnormal metabolic activity in the lungs, liver, skeletal system, and many lymph nodes (Figure 1B). An axillary lymph node biopsy showed a diffuse large B‑cell lymphoma (DLBCL). The patient received aggressive chemotherapy in the hematology department and went into remission.
Chronic back pain is a very common presenting complaint, yet it can represent serious diagnostic uncertainty. Establishing its origin, be it common mechanical pathologies (not requiring diagnostic imaging and managed conservatively), or rare malignant ones (which should lead to more detailed evaluation) is an important clinical skill. Given that obesity is one of the most common reasons for lower back pain1 and that this patient did not present with any “red flag” symptoms during his first visit, he was correctly recommended to lose weight by his GP. However, neurological symptoms (paresthesia) should raise some suspicions,2 and rightly the clinician ordered further imaging. It should be noted that DLBCL can present with neurological symptoms from any region of the spine (in this case the pain originated in the lumbosacral region with neuropathic symptoms in the cervical spine).
Low‑grade fever and sweating are nonspecific symptoms that should be considered in the context of the whole clinical picture. The differential diagnoses should include infectious and inflammatory diseases (eg, connective tissue disorders and inflammatory bowel disease), other chronic illnesses (such as hepatic cirrhosis or hepatitis), and malignant disorders (especially blood and lymphatic system disorders).
DLBCL is usually diagnosed at the advanced stage, when the survival rate is much lower than at earlier stages.3 Therefore, identifying “red flag” symptoms and conducting a follow‑up after the initial consultation is crucial for the early detection of certain hematological disorders and achieving more frequent successful therapeutic outcomes in aggressive lymphomas, such as DLBCL.
- Chou L, Brady SRE, Urquhart DM, et al. The association between obesity and low back pain and disability is affected by mood disorders. Medicine (Baltimore). 2016; 95: e3367. | Crossref
- Henschke N, Maher CG, Refshauge KM, et al. Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain. Arthritis Rheum. 2009; 60: 3072‑3080.7 | Crossref
- Durmaz M, Visser O, Posthuma EFM, et al. Time trends in primary therapy and relative survival of diffuse large B‑cell lymphoma by stage: a nationwide, population‑based study in the Netherlands, 1989‑2018. Blood Cancer J. 2022; 12: 38. | Crossref
ARTICLE INFORMATION