Oligosymptomatic microscopic colitis with eosinophilia in a patient returned from Rwanda



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Oligosymptomatic microscopic colitis with eosinophilia in a patient returned from Rwanda
Swimming in lakes located in intertropical regions is a risk factor for infection with blood flukes from the Schistosoma genus. Two types of clinical course for this trematode infection can be manifested: gastrointestinal and urinary, caused mainly by S. mansoni and S. haematobium, respectively. Classical diagnostics of schistosomiasis is based on a microscopic analysis of stool sample or urine sediment. A late diagnosis usually leads to irreversible complications, such as liver cirrhosis (S. mansoni) or prediction of bladder cancer (S. haematobium).1,2
A 54‑year‑old man presenting with mild, nonspecific, periodic abdominal discomfort was admitted to the Department of Tropical Diseases after returning from a 5‑year stay in Rwanda. The patient reported swimming in the Kivu Lake, where free‑living forms of Schistosoma sp. cercariae have been detected.3 They can actively invade human skin and cause infection.1
On admission, the physical examination did not reveal any abnormalities. In the basic laboratory analysis, only mild eosinophilia (white blood count [WBC], 8.9 × 103/μl, reference range, 3.9–11.0 × 103/μl, eosinophil count [EOS], 1.7 × 103/μl, reference range, 0.02–0.5 × 103/μl) was found in the blood count. There was no evidence of hypergammaglobulinemia.
Enzyme‑linked immunosorbent assays (ELISA) for the presence of antibodies against other parasitic tropical infections were negative for leishmaniasis and amebiasis, and highly positive for schistosomiasis (ie, 62 NTU [reference range, >11 NTU = positive result]). Subsequent immunoblotting confirmed the ELISA positive results by identifying immunoglobulin G antibodies against Schistosoma sp. antigens.4
Numerous stool samples were microscopically analyzed using the Kato–Katz test, and no Schistosoma sp. eggs were found. We also performed numerous microscopic analyses of urine sediment, and no S. haematobium eggs were found.4 Simultaneously, the fecal occult blood test was negative, and the level of calprotectin in the patient’s stool was normal.
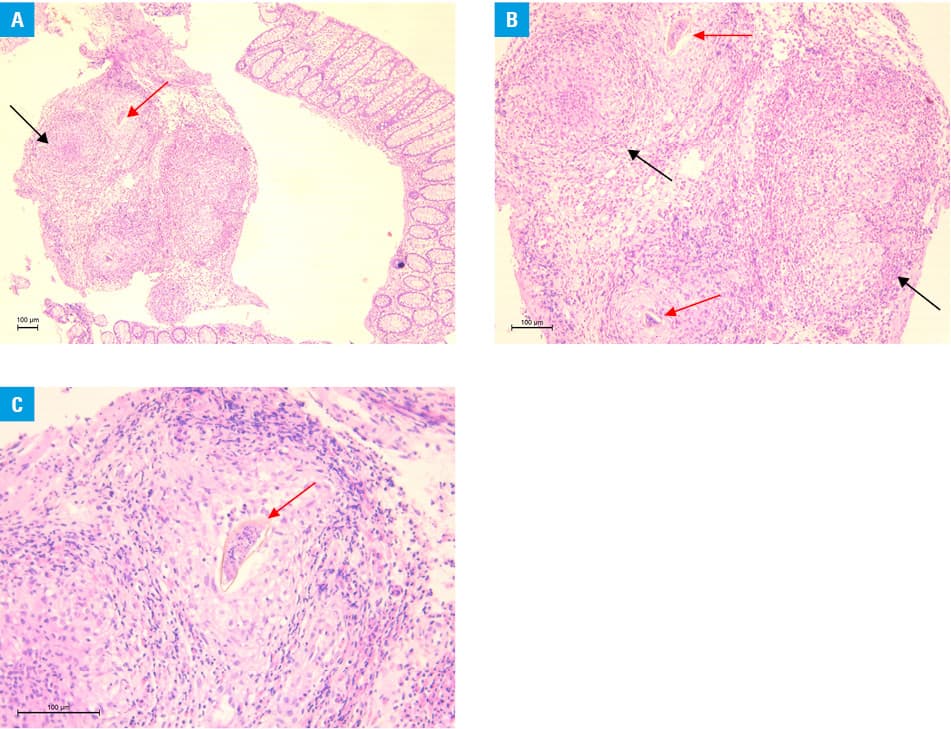
Because of the abdominal disturbances, the patient underwent a colonoscopy, which revealed numerous small, white, submucosal papules located in the cecum and ascending colon, and specimens were collected for histopathological analysis. Staining with hematoxylin and eosin confirmed the ova of Schistosoma sp. in the loose submucosa of the large intestine, accompanied by granuloma formulation with infiltration by many eosinophils (Figure 1). Additionally, an involvement of muscularis mucosa was observed, but the overlying mucosa showed no ulceration.
Since the abdominal ultrasound was clear, there was no suspicion of any complications. Treatment with praziquantel was implemented with an indirect diagnosis of parasitic infection. Histopathology results confirmed schistosomiasis 2 weeks later. The patient was followed to monitor changes in the eosinophilia. After the first 3 weeks, the EOS increased significantly (WBC, 10.6 × 103/μl, EOS, 4.2 × 103/μl), and then the decrease was observed (WBC, 9.9 × 103/μl, EOS, 3.5 × 103/μl).
“Schistosomiasis without eggs” refers to cases in which no ova are found on microscopic observations, but there is a high clinical suspicion of infection due to the patient’s long stay in an endemic area.5 It should be highlighted that direct detection of ova under a microscope or in urine sediment or stool sample brings about negative results until the flukes reach sexual maturity and start to produce eggs. Also, a small number of released eggs translates into negative results on microscopy.1 Thus, it is very important to analyze the presence of anti-Schistosoma antibodies by immunoassays, such as ELISA and Western blot that have high sensitivity and specificity.4 The potential for serious complications of untreated Schistosoma sp. infection justifies praziquantel treatment in patients with only indirect evidence of infection.
- Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. 2014; 383: 2253‑2264. | Crossref
- Ross AG, Olds GR, Cripps AW, et al. Enteropathogens and chronic illness in returning travelers. N Engl J Med. 2013; 368: 1817‑1825. | Crossref
- Madinga, J, Linsuke, S, Mpabanzi L, et al. Schistosomiasis in the Democratic Republic of Congo: a literature review. Parasites Vectors. 2015; 8: 601. | Crossref
- Weerakoon KG, Gobert GN, Cai P, McManus DP. Advances in the diagnosis of human schistosomiasis. Clin Microbiol Rev. 2015; 4: 939‑967. | Crossref
- Bustinduy AL, King CH. Schistosomiasis. In: Farrar J, Hotez PJ, Junghanss T, et al, eds. Manson’s Tropical Diseases, 23rd ed. Elsevier Health Sciences. 2014; 698‑725. | Crossref
ARTICLE INFORMATION