How to optimize the prevention of post‑thrombotic syndrome: recent advances
Key words: deep vein thrombosis, post-thrombotic syndrome, prevention, residual venous obstruction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
How to optimize the prevention of post‑thrombotic syndrome: recent advances
Post‑thrombotic syndrome (PTS) is the most frequent complication of deep vein thrombosis, and it can be detrimental to the quality of life of the affected patients. Once affected by this chronic condition, the patient’s treatment options are very limited, so preventive therapies are crucial. Currently, the prevention of PTS is hampered by the lack of unequivocally effective therapies. However, improved insight into pathogenesis of this condition acquired in recent years, including the central role of residual venous obstruction, could lead to a better application of the existing therapies and identification of novel therapeutic targets. Plausible therapeutic agents include flavonoids and statins, while promising future agents include those that target leukocyte‑endothelial interaction. Moreover, differences in PTS risk were found to be partly explained by a tendency of patients to form clots that are less susceptible to lysis. Finally, identifying patients that are expected to benefit most from certain therapies is equally valuable for the success of future preventive strategies. This requires exploration of better risk stratification through machine learning techniques.
Introduction
Post‑thrombotic syndrome (PTS) is the manifestation of chronic venous disease (CVD) following an episode of deep vein thrombosis (DVT).1 PTS develops in about 1 in 3 patients, making it the most frequent complication of DVT.1 It adversely affects the quality of life, productivity, and health care costs.2-4 Thus, PTS is an important health issue, the prevalence of which is only expected to increase due to ageing of the population, rising life expectancy, and improved DVT survival. Since PTS is considered an irreversible condition and treatment options are limited, the cornerstone of its management lies in prevention.1 However, currently there is a lack of unequivocally effective preventive therapies, which leaves clinicians empty‑handed in the care for their patients. Luckily, the last decade has seen many advances in our understanding of the pathogenesis of PTS, mainly based on experiments in mouse models of DVT.5 These insights are gradually leading to translational studies and clinical trials. In this review, we provide an overview of these advances and their translation into clinical practice. We discuss several promising therapeutic agents, and how these might interact with pathogenic processes. Finally, we stress the increasing importance of risk stratification for PTS by classic or machine learning methods to identify the best candidates for specific preventive therapies in the future.
Diagnosis
PTS is a constellation of signs and symptoms in the affected extremity following DVT, which can vary from patient to patient.1 There is no gold standard for diagnosis, and research has long been hampered by the use of different diagnostic scores. To improve comparability between studies, in 2009 the International Society of Thrombosis and Haemostasis (ISTH) reached a consensus on adopting the Villalta score as the preferred diagnostic tool (Table 1).6 This score combines 5 symptoms (ie, pain, cramps, heaviness, paresthesia, pruritus) and 6 signs (ie, edema, skin induration, hyperpigmentation, redness, venous ectasia, painful calf compression). Each item receives a score varying from 0 (absent) to 3 (severe), and PTS is diagnosed if the combined score is equal to or above 5 or venous ulceration is present at least 6 months after the acute DVT. Venous claudication, a tense painful feeling that occurs during walking and persists upon rest, is not included in this score. An important limitation of the ISTH consensus definition is that this chronic condition can be diagnosed based on a single observation, although symptoms can be nonspecific and vary over time. This could result in an overestimation of the number of patients with PTS, particularly its mild cases (Villalta score <10) without objective signs.7 Thus, if feasible, it is preferable to confirm the diagnosis on 2 consecutive assessments, in agreement with the original scoring method by Prandoni.8This requires regular visits during at least 1 year following DVT.
Criteriaa | None | Mild | Moderate | Severe |
a Each item receives a score from 0 to 3 based on severity. Post‑thrombotic syndrome is diagnosed if the total score is at least 5. It can be categorized as mild (score 5–9), moderate (score 10–14) or severe (score ≥15). If venous ulcer is present and the total score is below15, then a total score of 15 is assigned, which puts it in the severe category. | ||||
Subjective criteria: symptoms | ||||
Pain | 0 | 1 | 2 | 3 |
Cramps | 0 | 1 | 2 | 3 |
Heaviness | 0 | 1 | 2 | 3 |
Paresthesia | 0 | 1 | 2 | 3 |
Pruritis | 0 | 1 | 2 | 3 |
Objective criteria: clinical signs | ||||
Pretibial edema | 0 | 1 | 2 | 3 |
Skin induration | 0 | 1 | 2 | 3 |
Hyperpigmentation | 0 | 1 | 2 | 3 |
Redness | 0 | 1 | 2 | 3 |
Venous ectasia | 0 | 1 | 2 | 3 |
Pain on calf compression | 0 | 1 | 2 | 3 |
Venous ulcer | Absent | Present | ||
Clinical manifestation
The clinical manifestation of PTS shows a substantial overlap with that of primary CVD. Therefore, similarities in their pathophysiology are presumed, with a central role for venous hypertension. Hypertension from the deep veins is transferred to the capillary system, which increases the capillary leakage of plasma, red blood cells, and leukocytes into the interstitial space.9 Increased interstitial volume presents as edema, and elevated intracompartmental and subcutaneous pressure can be experienced as heaviness.10 Proinflammatory cytokines released by leukocytes and other local cells activate nociceptors, which results in chronic pain and painful calf compression.11 Inflammation also leads to vasodilation that can be observed as skin redness.10 Venous hypertension causes fibrin and collagen deposition around dermal capillaries, which impairs oxygenation and nutrient perfusion. Subsequent loss of epidermal integrity can result in skin induration and, in extreme cases, lipodermatosclerosis with ulceration due to impaired wound healing.9 Dilated veins due to hypertension can be observed as venous ectasia, and deposition of hemosiderin can lead to hyperpigmentation.9 Causes of cramps, paresthesia, and pruritus are less clear. Finally, venous claudication is more characteristic of PTS, and can be explained by ambulatory hypertension upon increased blood flow with proximal obstruction during walking.10
Current prevention
Anticoagulant therapy
Following DVT, patients routinely receive anticoagulant therapy for at least 3 months to prevent short‑term complications and recurrent venous thromboembolism (VTE). Moreover, observational studies in patients receiving vitamin K antagonists (VKAs) have shown subtherapeutic anticoagulation within the first 3 months to be associated with 2‑fold increased odds of developing PTS.13,14 Extension of anticoagulant therapy beyond this time does not seem to have any preventive effect, as demonstrated by 2 randomized controlled trials (RCTs).15,16 Studies suggest a reduction of PTS risk in patients treated either with low‑molecular weight heparin (LMWH)17 or direct oral anticoagulants (DOACs),18 as compared with VKAs. For DOACs, these data are based almost exclusively on factor Xa inhibitor rivaroxaban; a recent trial found no effect for a direct thrombin inhibitor dabigatran.19 Awaiting more convincing evidence, current guidelines do not recommend a specific type of anticoagulant to prevent PTS.20
Elastic compressive therapy
Elastic compressive therapy (ECT) for 2 years after DVT was introduced as an integral element of PTS prevention 20 years ago, based on 2 RCTs that demonstrated a 50% risk reduction.21,22 Later, its effectiveness was questioned when a placebo‑controlled larger SOX (Compression Stockings to Prevent the Post‑Thrombotic Syndrome) trial failed to show any beneficial effects,23 and as a result ECT was no longer recommended by most guidelines.24This negative RCT, however, has since been criticized due to reported low therapy adherence, which most likely influenced its results. A meta‑analysis including subsequent trials indicated a trend favoring the use of ECT.25 Therapy adherence is critical for ECT to be effective. It might be improved by using more tolerable below‑knee stockings, which were found to be as effective as thigh‑length stockings.26 It might also be improved by individualized shortening of therapy duration up to a minimum of only 6 months based on the Villalta score, which was shown to have high adherence and to be noninferior to a regular 2‑year duration in the IDEAL trial (Individualised Versus Standard Duration Of Elastic Compression Therapy For Prevention Of Post‑Thrombotic Syndrome).27 A recently completed RCT, the CELEST trial (Compression Stockings To Prevent Postthrombotic Syndrome),28 investigated whether lower‑strength stockings (25 mm Hg) are as effective as currently used stockings (35 mm Hg). The tested hypothesis was that lower‑strength stockings might improve adherence, and findings of this trial are expected to be published soon.28
Therapeutic thrombolysis
Thrombus removal has long been advocated to have the potential to lower the risk of developing PTS but trials using therapeutic thrombolysis have yielded mixed results.29 So far, 3 RCTs using catheter‑directed thrombolysis (CDT) in addition to a regular therapy have been published. The CaVenT trial (Post‑Thrombotic Syndrome After Catheter‑Directed Thrombolysis for Deep Vein Thrombosis) in patients with femoral or iliofemoral DVT observed an absolute PTS risk reduction of 14% after 2 years, and of 28% after 5 years.30,31 The CAVA32trial (Ultrasound‑Accelerated Catheter‑Directed Thrombolysis Versus Anticoagulation For The Prevention of Post‑Thrombotic Syndrome) in patients with iliofemoral DVT did not find significantly less frequent PTS after 1 year, although using the ISTH consensus definition a significant 22% absolute reduction in PTS was observed after a median follow‑up of 39 months.33 Finally, the ATTRACT trial (Acute Venous Thrombosis: Thrombus Removal With Adjunctive Catheter‑Directed Thrombolysis) in patients with proximal DVT did not find any difference in PTS after 2 years,34 although CDT did lower PTS severity in patients with iliofemoral DVT.35 This uncertain efficacy is offset by significantly higher major bleeding risk in patients allocated to CDT, which is the reason why the current guidelines do not recommend routine CDT in proximal DVT.24 On a case‑by‑case basis, patients with extensive thrombosis, limb‑threatening clinical presentation, and low bleeding risk might be selected for CDT in experienced centers.24
Pathogenic processes and therapeutic targets
To find ways to move forward in the prevention of PTS, it is worthwhile taking a closer look at its pathogenesis. Despite similarities in clinical manifestations, PTS has a very different etiology to that of primary CVD, involving distinct pathogenic processes. While primary CVD is characterized by a gradual buildup of venous hypertension and skin changes with aging primarily due to valvular reflux, PTS has a relatively rapid onset.1 Following DVT, there is an acute onset of venous hypertension due to venous obstruction. This DVT is then gradually resolved over the duration of several weeks to months through an immune‑mediated process similar to wound healing, including an acute, subacute, and chronic phase.1 In some patients, however, restoration of the vein patency is incomplete due to an interplay of pathogenic processes leading to residual venous obstruction (RVO) as visualized in Figure 1. This interplay can be summarized as a vicious circle, which is shown in Figure 2. In brief, venous obstruction causes hypertension, leading to endothelial dysfunction with increased leukocyte extravasation and activation. This promotes persistent inflammation, which delays thrombus resolution. Meanwhile, vein wall fibrosis continues, and the thrombus is gradually incorporated into the vein wall, resulting in RVO. Below we discuss the latest insights into each of these processes, based mainly on mouse models of DVT.36 We look for correlations between them and clinical observations and highlight several potential therapeutic targets.
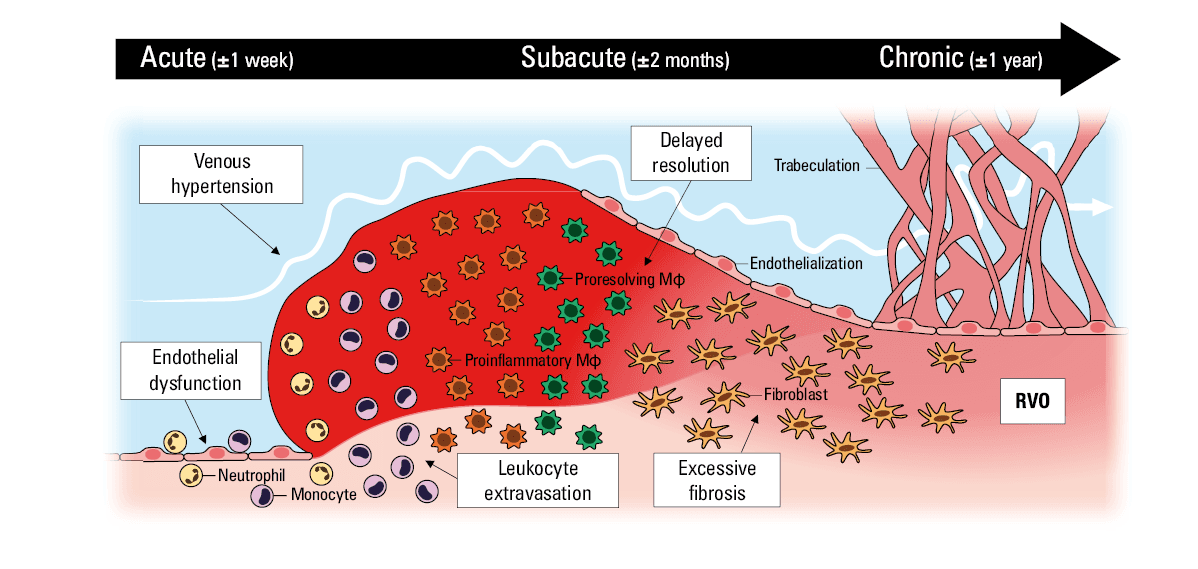
Abbreviations: Mφ, macrophage; RVO, residual venous obstruction
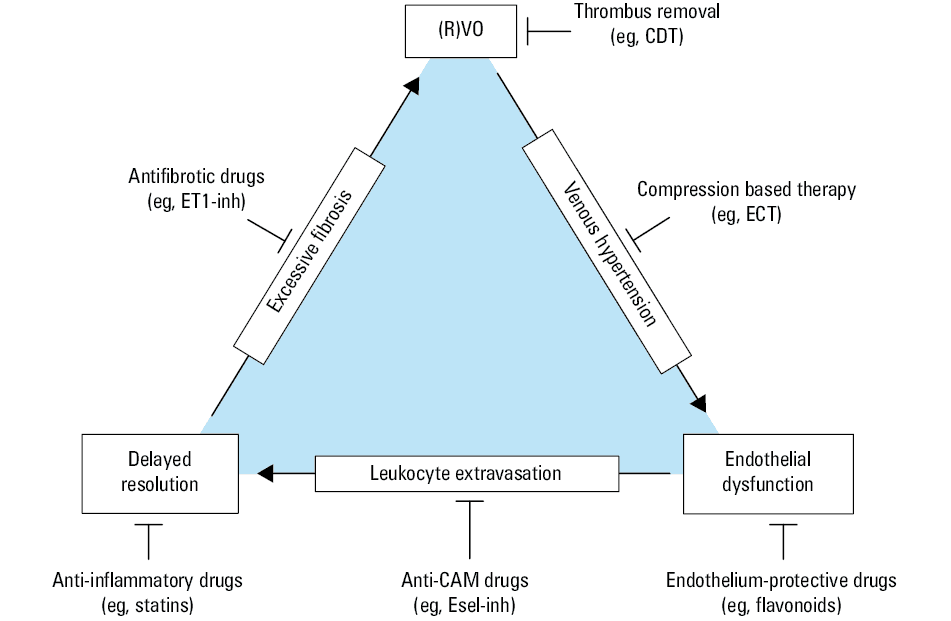
Abbreviations: CAM, cell adhesion molecule; CDT, catheter‑directed thrombolysis; ECT, elastic compressive therapy; Esel‑inh, E‑selectin inhibitor; ET1‑inh, endothelin‑1 inhibitor; others, see Figure 1
(Residual) venous obstruction
Venous obstruction by DVT, and later RVO, is considered the major driver in the pathogenesis of PTS. Indeed, clinical ultrasound assessment shows RVO as strongly associated with the risk of PTS.37 Thus, it has been hypothesized that early restoration of patency—before fibrosis has occurred—can lower the risk of PTS, which is referred to as the open vein hypothesis.38 This has been supported by findings in mouse models, where smaller vein wall damage is observed if the thrombus is adjacent to the vein wall for a shorter time.39However, more recently this hypothesis has lost its credibility due to the lack of effectiveness in clinical trials with CDT.38 Interestingly, subanalyses of these trials showed that complete patency was often not achieved and postprocedural RVO was associated with PTS.40-42 Experiments have since revealed that the efficacy of therapeutic thrombolysis is highly dependent on the thrombus age: no effect on thrombus resolution or vein wall fibrosis was observed when thrombolytics were administered more than 4 days after DVT in mice, which correlates with about a week in humans.5,35 Accordingly, a post‑hoc analysis of the ATTRACT trial found that only patients included 8 days or less after the symptom onset benefited from reduced PTS symptoms by CDT. Surprisingly, those included earlier than 4 days after the symptom onset did not benefit from CDT, perhaps because anticoagulation alone was sufficient in these fresh thrombi.38,43 These findings highlight that the therapeutic window for CDT is much narrower than the 3 weeks assumed in other trials.30,35 This could be explained by thrombus endothelialization, which occurs in the subacute phase, starting after about 1 week, and makes the thrombus inaccessible to administered thrombolytics.44 Thus, CDT might expand its therapeutic window by innovations that allow for penetration of this endothelial layer. Moreover, it is important to be aware that the patient‑reported symptom onset is not a robust indicator of the thrombus age.45 In a post‑hoc analysis of the CAVA trial, the patients reporting symptoms since 1–2 weeks or 2–3 weeks already had chronic thrombi in 16% and 41%, respectively, based on magnetic resonance venography (MRV).46 These patients are beyond the reversible period and should not be exposed to unnecessary bleeding risk induced by CDT. Also, there was a considerable overlap between acute and subacute thrombi; adding novel MRV labels of fibrin accessibility might provide further differentiation in these specific cases.44 Conclusively, therapeutic innovations and improved pre‑selection are needed to increase the efficacy of CDT. Most patients, however, are expected to remain ineligible and require other preventive strategies.
Venous hypertension
Obstruction by DVT leads to hypertension in the affected veins, which is perpetuated in the presence of RVO. Valvular reflux due to local valve damage caused by DVT also contributes to hypertension, although its contribution to the risk of PTS seems limited based on ultrasound assessment of popliteal reflux.37 Apart from local valves, also distal valves can become insufficient due to vein dilation and remodeling in response to increased wall tension induced by hypertension.9 A consequence of venous hypertension is endothelial dysfunction, which is promoted through shear stress and glycocalyx injury, but also through hypoxia due to stasis.47As further discussed below, this has a detrimental effect on the thrombus resolution and vein wall fibrosis. Venous hypertension can be counteracted with ECT, which uses graded compression to lower the venous pressure by improving the venous ejection fraction.48 In a mouse model, normalized blood flow significantly improved thrombus resolution and reduced vein wall fibrosis.49 Trials found that immediate ECT in DVT patients significantly reduces the incidence of RVO as compared with ECT delayed by several weeks, when acute edema has resorbed.50,51 Correspondingly, the patients with immediate ECT had lower incidence of PTS.50 This observation supports the hypothesis that the therapeutic target of ECT should be the acute and subacute resolution phase. It is unsure what ECT can contribute after this period, and optimal therapy duration remains uncertain. Interestingly, a recent observational study suggested that prolonging ECT is only worthwhile in patients with RVO, measured 3 months after DVT; again, the presence of popliteal reflux was irrelevant.52 Thus, ECT might still be beneficial in the chronic phase for those with delayed resolution. Taken together, in contrast with current guideline recommendations, recent evidence supports ECT as an essential part of PTS prevention, on the condition of its immediate application and adherence.
Endothelial dysfunction
Endothelial cells are essential regulators of thrombus resolution.53 They regulate extravasation and activation of leukocytes, regulate fibrinolysis, endothelialize the damaged vein and thrombus, form neovascular channels, and modulate fibrosis.5 While these cells accelerate thrombus resolution, their dysfunction and reduced survival can have detrimental effects on the thrombus resolution and vein wall fibrosis.53,54 Thus, endothelium‑protective therapy in patients with DVT might be beneficial. A drug group already on the market that fits this description are flavonoids. These antioxidants protect endothelial cells from hypoxia and inflammation, have affinity for venous endothelium, and were found in clinical studies to reduce markers of endothelial damage and dysfunction.55-58 Flavonoids, in particular modified variants of rutoside and micronized purified flavonoid fraction (MPFF), were found to reduce the symptoms in both primary CVD and PTS.59,60 Guidelines recommend these flavonoids in the treatment of primary CVD, and a large trial is ongoing to confirm the effectiveness of MPFF in reducing the symptoms of PTS (NCT03833024). Based on these observations, it is plausible that early flavonoid treatment might prevent the onset of PTS. This was recently assessed in a pilot trial of 90 patients treated with MPFF, which found accelerated vein recanalization and reduced incidence of PTS after 1 year, with 8.9% PTS in the participants treated with MPFF and 48.9% PTS in those not receiving MPFF.61 This striking finding will have to be confirmed in future trials. Moreover, the trial did not clarify if its effect on PTS symptoms persisted after stopping MPFF. Another pilot trial assessing the effect of rutoside treatment on the presence of RVO is ongoing (NCT04670432). One more endothelium‑protective drug is sulodexide, a glycosaminoglycan that protects endothelial cells mainly by supporting their glycocalyx, similarly to heparin or LMWH but without the anticoagulant effect.63 It has been found to increase healing of venous ulcers, although this is based on low‑quality evidence.64 In an observational study, sulodexide treatment after DVT was associated with significantly lower incidence of PTS after 1 and 5 years.65 However, this study used a modified definition of PTS, hampering comparability with other studies. Thus, a clinical trial using the ISTH consensus definition is warranted to confirm its findings.
Leukocyte extravasation
When endothelium becomes dysfunctional, there is an increased expression of cell adhesion molecules (CAMs) on its surface. These CAMs increase activation and extravasation of circulating leukocytes into the thrombus and vein wall.5 Inhibitors of CAMs, such as P‑selectin, E‑selectin, intercellular adhesion molecule 1 (ICAM‑1), or vascular cell adhesion molecule 1 (VCAM‑1) were found to accelerate resolution and reduce vein wall fibrosis in animal models of DVT.66,67 Their clinical relevance is supported by circulating marker studies in DVT patients. High levels of soluble ICAM‑1 after DVT were consistently over time associated with PTS risk.68,69 Also, patients with PTS tend to have higher levels of soluble VCAM‑1,70 and those with severe PTS (Villalta score ≥15) have higher levels of soluble E‑selectin. Finally, high levels of soluble P‑selectin were found to predict DVT recanalization.71 Consequently, inhibition of CAMs has been considered a therapeutic target, particularly for selectins. Exogenous inhibition of P‑selectin or E‑selectin has shown great promise by reducing leukocyte extravasation, accelerating thrombus resolution, and reducing vein wall fibrosis and thickness in a baboon model, which is considered comparable to human DVT.66 Several P‑selectin antagonists have been developed, and registered antibodies inclacumab and crizanlizumab are currently studied in trials for various diseases, although not in VTE.66 It must be noted that P‑selectin is also present on platelets, making E‑selectin a more specific target to inhibit leukocyte extravasation. Uproleselan, an E‑selectin antagonist, had an acceptable safety profile in healthy individuals, but a trial in patients with DVT unfortunately experienced difficulties in patient accrual, possibly because its administration was intravenous.72 Despite promising preliminary outcomes, there are currently no ongoing trials with these drugs in the context of PTS prevention. For now, we have to wait on their effects and off‑target effects in trials with other diseases, an overview of which was recently published by Purdy et al.66
Delayed resolution
DVT elicits an immune response with leukocytes infiltrating the thrombus. In the acute phase neutrophils are the predominant subset, but in the subacute phase this role is shifted to monocytes, which then differentiate into macrophages.5 Lymphocytes, mainly effector‑memory T cells, have also been observed to infiltrate the thrombus.5 This immune response is initially of an inflammatory type, which aims to stabilize the thrombus and guarantee sterility.5 Next, a resolving response is initiated by macrophages that shift into a proresolving phenotype to orchestrate the thrombus resolution.5 Proresolving macrophages do this by clearing cellular and matrix debris, promoting fibrinolysis, influencing tissue remodeling, and facilitating neovascularization.5 However, if an inflammatory response persists instead, thrombus resolution is delayed and fibrosis continues, leading to RVO.5 Indeed, increased proinflammatory markers, such as interleukin 6 (IL‑6) in patients after DVT are associated with both the presence of RVO71,73 and onset of PTS.69,74Also, an increased level of proresolving marker IL‑10 at 6 months after DVT, but not at earlier timepoints, is associated with PTS, supporting the negative role of delayed resolution in patients.69 After the onset of PTS, patients still have increased inflammatory markers and their leukocytes express more proinflammatory factors than leukocytes in unaffected patients.75-77 Reasons why some patients present with persistent inflammation and delayed resolution are unclear. Inhibition of inflammation has been proposed as a therapeutic target to accelerate thrombus resolution and prevent PTS, for example using a registered IL‑6 inhibitor tocilizumab. However, inhibition of IL‑6 has yielded conflicting results in different mouse models, even finding delayed resolution in 1 study, which showed an initial inflammatory response is essential for thrombus resolution.5,78 Also, IL‑6 inhibition is known to have off‑target effects on immunity. A more promising drug class with anti‑inflammatory properties are statins. Rosuvastatin and atorvastatin accelerated thrombus resolution and reduced vein wall fibrosis in a mouse model.79 An observational study identified statins as protective factors for PTS, and another study found that statin use was associated with improved thrombus resolution on ultrasound 1 month after DVT.80,81 Furthermore, an RCT with 3‑month adjuvant use of rosuvastatin after DVT reported a significantly decreased PTS incidence from 48% to 38%.82 In contrast, a recently published RCT did not find any difference in PTS incidence after 6 months of rosuvastatin therapy.83 A potential explanation for this lack of effect might be that the therapy in this RCT was started within a month after DVT (median, 16 days), which might have been too late to exert a positive effect on the thrombus resolution. Thus, the jury is still out on whether there is any place for statins in the prevention of PTS. Meanwhile, an exciting new advent is the use of specialized proresolving mediators to promote resolution. Research on such mediators is still in its infancy but recently the endogenous lipid resolving D4 was identified as a potent promotor of thrombus resolution.84
Excessive fibrosis
If thrombotic material remains present into the late subacute phase, it is fibrosed and gradually incorporated into the vein wall.1 This occurs through rapid collagen deposition in the residual thrombus and adjacent vein wall combined with remodeling by matrix metalloproteinases.5 Once fibrin is replaced, a slower maturation process similar to wound healing follows in the chronic phase, including further remodeling and replacement of collagen type 3 by type 1.5 While vein wall fibrosis is dependent on the presence of adjacent residual thrombus, it is also determined by local signaling factors.39 A major driver of fibrosis by fibroblasts is transforming growth factor β. Its release from endothelial cells is stimulated by endothelin‑1 (ET‑1). Exogenous inhibition of ET‑1 was found to accelerate thrombus resolution and reduce vein wall fibrosis in a mouse model.85 Thus, this has been considered as a therapeutic target and its effect was reproduced with ET‑1 inhibitor bosentan.85 Unfortunately, this drug has several off‑target effects including an antidiuretic effect leading to peripheral edema.86 Therefore, its use in clinical practice would benefit from targeted drug delivery systems (eg, nanobody‑based) currently under development.
Influence of clot properties
Aside from the above‑described response to DVT, the thrombus itself also plays a role in the pathogenesis of PTS. This includes the extent and proximity of DVT with, for example, a 2‑fold increased risk of PTS in patients with iliofemoral DVT.1 However, the thrombus composition also has an important role. In mouse models, the mechanism of thrombogenesis (eg, stasis or nonstasis) was found to have more impact on the vein wall response than the thrombus size.39 In clinical care, it has been found that patients with RVO or PTS form denser clots with thinner fibers, which make them less permeable and impair their susceptibility to lysis.87,88 Moreover, these clot properties assessed 3 months after DVT could also predict PTS, its severity and venous ulceration.89,90 These clot properties are known to depend on various patient‑specific factors, which are summarized in Figure 3. An example of such a factor is elevated thrombin generation. Interestingly, elevated circulating prothrombin fragments upon DVT diagnosis, representing thrombin generation, are associated with poor vein recanalization.91 Other factors, such as inflammatory diseases or fibrinogen polymorphisms, have received limited attention in the context of PTS. These clot properties partly explain why some patients develop PTS while other patients readily lyse their DVT. It can be speculated that these properties also play a role in the efficacy of CDT, which is something that warrants further investigation.
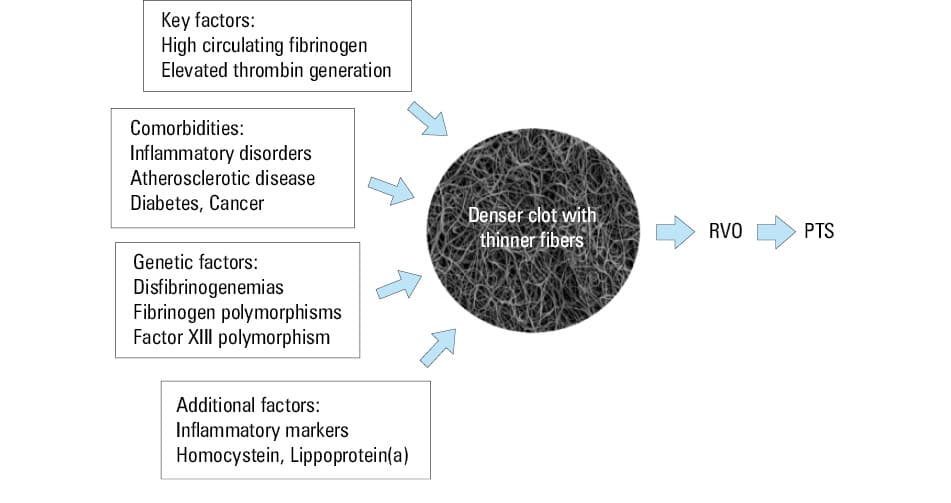
Abbreviations: PTS, post‑thrombotic syndrome; others, see Figure 1
Risk stratification to guide prevention
Stratification of PTS risk in patients following DVT can be expected to gain importance once effective preventive therapies are established by future research. Patients at increased risk should be offered more intensive preventive strategies. Currently, 2 externally validated risk models have been published. The baseline model by Amin et al92 uses risk factors of old age, male sex, obesity, smoking, varicose veins, previous DVT, provoked DVT, and iliofemoral DVT. Additionally, it uses the presence of RVO to stratify the risk even further after 6 months of treatment. The model by Rabinovich et al93 is based on iliofemoral DVT, obesity, and baseline Villalta score. While these classic types of risk models are valuable to assess the risk for individual patients, they miss potential heterogeneity of the patients. To tackle this issue, recent years have seen an increased use of cluster analysis, a machine learning technique that identifies distinct subgroups of patients within populations. These analyses can provide further pathogenic insight, particularly when nonphenotypic data (eg, biomarkers, genetics) are included.94 Therefore, future stratification of subgroups could not only improve risk models but also guide the selection of an adequate preventive therapy. For example, pathogenic mechanisms in patients with pre‑existent CVD might be distinct from those in patients with inflammatory disorders, and therefore they may benefit from different preventive strategies.
Conclusions
PTS is a common chronic complication of DVT that manifests itself similarly to primary CVD and has limited treatment options. Its diagnosis should be made using the Villalta score during regular visits following DVT for at least 1 year. Its prevention encompasses applying immediate ECT and providing adequate anticoagulant therapy during the first 3 months. To improve adherence, we recommend compression using knee‑high stockings for a tailored duration of at least 6 months based on the Villalta score. Of anticoagulant agents, DOACs (particularly factor Xa inhibitors) seem to be more effective than VKAs. Nevertheless, there remains a high‑risk population of DVT patients who require additional preventive therapies that are currently not available. In recent years, however, extensive insight has been gained into the pathogenesis of PTS with identification of several therapeutic targets. Trials using statins or flavonoids have been performed or are underway, but their further translation into clinical practice is dearly needed. Personalized risk stratification to support adequate patient selection will be of paramount importance for the effectiveness of these therapies in the near future.
- ten Cate‑Hoek AJ, Henke PK, Wakefield TW. The post thrombotic syndrome: ignore it and it will come back to bite you. Blood Rev. 2016; 30: 131‑137. | Crossref
- Kahn SR, Hirsch A, Shrier I. Effect of postthrombotic syndrome on health‑related quality of life after deep venous thrombosis. Arch Intern Med. 2002; 162: 1144‑1148. | Crossref
- Roberts LN, Patel RK, Donaldson N, et al. Post‑thrombotic syndrome is an independent determinant of health‑related quality of life following both first proximal and distal deep vein thrombosis. Haematologica. 2014; 99: e41‑e43. | Crossref
- Guanella R, Ducruet T, Johri M, et al. Economic burden and cost determinants of deep vein thrombosis during 2 years following diagnosis: a prospective evaluation. J Thromb Haemost. 2011; 9: 2397‑2405. | Crossref
- Nicklas JM, Gordon AE, Henke PK. Resolution of deep venous thrombosis: proposed immune paradigms. Int J Mol Sci. 2020; 21: 2080. | Crossref
ARTICLE INFORMATION