A rare case of metastatic pheochromocytoma in the course of neurofibromatosis type 1



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A rare case of metastatic pheochromocytoma in the course of neurofibromatosis type 1
Most pheochromocytomas are sporadic; however, up to 40% of the cases have a genetic background.1 In neurofibromatosis type 1 (NF1) pheochromocytoma is very rarely observed, having a prevalence of 0.1% to 5.7%. Among them, up to 12% might be malignant.2,3
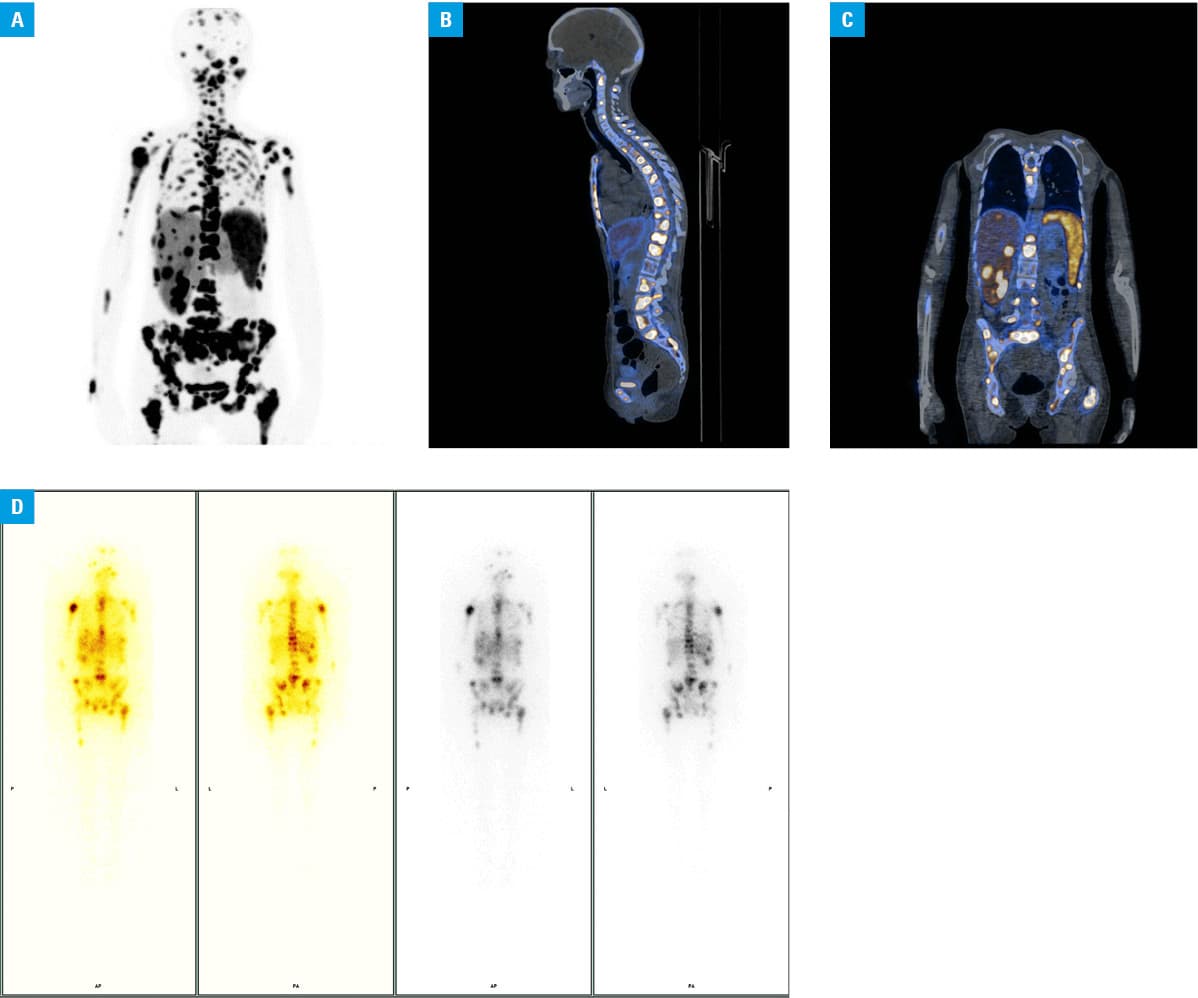
We present a case of a 36‑year‑old woman with a metastatic pheochromocytoma in the course of NF1. The patient had a positive family history (affected mother) and NF1 clinically diagnosed at the age of 3. At the age of 35, routine follow‑up abdominal ultrasonography revealed a heterogeneous litho‑cystic tumor (100 × 70 mm) between the spleen and left kidney. On computed tomography (CT), a hypodense mass (100 × 80 × 100 mm) with necrotic lesions and peripheral hypervascularization, and multiple lesions categorized as neurofibromas were observed. Clinically, only 1 episode of heart palpitations accompanied by nonspecific abdominal pain with normal blood pressure was recorded. Twenty‑four‑hour urinary fractionated metanephrine collection showed significant elevation of normetanephrine, metanephrine, and 3‑metoxytyramine levels: 15 502.9 µg/24 h (upper limit of normal [ULN], 440), 8625.4 µg/24 h (ULN, 220), and 3357.4 µg/24 h (ULN, 341), respectively. Doxazosin up to 6 mg was introduced and an emergency left adrenalectomy with nephrectomy was performed due to local mass invasion and a risk of the tumor rupture. Histopathological assessment confirmed the diagnosis of pheochromocytoma (the Pheochromocytoma of the Adrenal gland Scaled [PASS] score of 10, pT2R0LV1, according to the American Joint Committee on Cancer 2017), features of angioinvasion, necrosis, capsule infiltration, mitosis activity 5/10 high power fields, and single atypical mitosis. The patient reported postoperative persistent pain in the left hip and left lower limb (7/10 using a numerical rating scale)4 despite analgesic therapy with opioids. Magnetic resonance imaging of the lumbosacral region (5 months after the first CT) revealed pathological masses at L5–S1, and remodeling of the Th12/L1/L2 vertebrae with propagation into the epidural space. The lesions were suggestive of neurofibrosarcomas. Numerous circular lesions suspected to be metastases in the liver (not visible on the prior CT) were detected. Because of the persistent elevation of urinary metanephrines, doxazosin therapy was reinitiated. [68Ga]Ga‑DOTA‑TATE positron emission tomography / CT confirmed dissemination to the bones, liver, and lungs (Figure 1A–1C). Based on meta‑iodo‑benzyl‑guanidine (MIBG) scintigraphy (Figure 1D), the patient was qualified for [131I]I‑MIBG therapy in a single dose of 7.4 GBq. The post‑therapeutic imaging confirmed uptake in numerous lesions. The treatment was complicated by neutropenia and thrombocytopenia. Furthermore, persistent macrocytic anemia, thrombocytopenia, and lymphopenia, elevated calcium concentration, and slightly elevated liver enzymes were observed. The next administration of [131I]I‑MIBG was considered; however, subsequent rapid progression of the disease resulted in the patient’s death.
Current recommendations on NF1 do not include systematic biochemical screening for the presence of pheochromocytoma.5 However, based on the observations presented by Zinnamosca et al,3 the actual incidence of pheochromocytoma in NF1 may be underestimated.2,3 Undiagnosed pheochromocytoma in NF1 patients, often qualified for surgical procedures, creates an important health hazard.2 Based on the need for that, and on our case, we support the view of routine hormonal assessment towards pheochromocytoma in patients with NF1. Due to the rarity of the disease, a prospective, multicenter study is needed.
- Sarkadi B, Saskoi E, Butz H, Patocs A. Genetics of pheochromocytomas and paragangliomas determine the therapeutical approach. Int J Mol Sci. 2022; 23: 1450. | Crossref
- Moramarco J, El Ghorayeb N, Dumas N, et al. Pheochromocytomas are diagnosed incidentally and at older age in neurofibromatosis type 1. Clin Endocrinol (Oxf). 2017; 86: 332‑339. | Crossref
- Zinnamosca L, Petramala L, Cotesta D, et al. Neurofibromatosis type 1 (NF1) and pheochromocytoma: prevalence, clinical and cardiovascular aspects. Arch Dermatol Res. 2011; 303: 317‑325. | Crossref
- Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain. 1986; 27: 117‑126. | Crossref
- Legius E, Messiaen L, Wolkenstein P, et al. Revised diagnostic criteria for neurofibromatosis type 1 and Legius syndrome: an international consensus recommendation. Genet Med. 2021; 23: 1506‑1513.
ARTICLE INFORMATION