Treatment of acute coronary syndromes during the COVID‑19 pandemic: a designated COVID‑19 hospital perspective



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Treatment of acute coronary syndromes during the COVID‑19 pandemic: a designated COVID‑19 hospital perspective
Introduction
The COVID‑19 pandemic has become a leading health problem in Poland and worldwide.1 The growing number of patients infected with SARS‑CoV‑2 led to a reorganization of work in health care facilities. The need to provide extra beds for patients with COVID‑19 resulted in the cancellation of scheduled procedures and difficulties in access to medical care. In addition, the patients themselves have been limiting their contacts with health care professionals for fear of infection. In Poland, after the epidemic had been announced at the beginning of March 2020, 16 infectious diseases hospitals designated for the treatment of patients with COVID‑19 were established.2 One of them was the J. Struś Multidisciplinary City Hospital in Poznań with a Cardiology Department. Starting from the beginning of the pandemic, the hospital was put on 24‑hour duty for patients with the diagnosis or suspicion of COVID‑19. In that period, only patients with a confirmed SARS‑CoV‑2 infection and comorbidities, including acute coronary syndrome (ACS), were hospitalized in the Cardiology Department. The pandemic has had a huge impact on the functioning of the Cardiology Department and the Heart and Vascular Laboratory (catheterization laboratory).
The aim of this study was to analyze the procedures performed in patients with ACS in the catheterization laboratory from March 15 to December 5, 2020, that is, during the first and second waves of the pandemic.
Methods
We compared the frequency of diagnosis of different types of myocardial infarction and the number of coronary angiographies and coronary angioplasties performed in the patients diagnosed with ACS between March 15 and December 5, 2020 with data from the same period in 2019. The comparison also included the number of hospitalizations and deaths.
The study was of retrospective design. Information on the procedures performed, diagnoses, comorbidities, and deaths was obtained from an electronic database of the Cardiology Department created based on patients’ medical histories and administered by physicians. The study did not require consent of the Bioethics Committee.
Statistical analysis
The STATISTICA 10 software (Statsoft, Tulsa, Oklahoma, United States) was used for statistical analysis. Continuous variables were presented as means and categorical variables as numbers and percentages. For data with binomial distribution, the binomial proportion test was applied to compare the parameters between the 2 groups. Statistical significance was set at P below 0.05.
Results
In the time interval covering the first and second waves of the pandemic (March 15 to December 5, 2020), a total of 390 patients were hospitalized in the Cardiology Department. During that period, 53 coronary artery angiographies were performed in the catheterization laboratory in the patients diagnosed with ACS (ST‑segment elevation myocardial infarction [STEMI] and non‑STEMI [NSTEMI]). The mean age of the patients was 61 years (range, 36–96). Men constituted 75% (n = 40) of the study population. Of the study participants, 74% (n = 39) had NSTEMI and 26% (n = 14) had STEMI. A total of 30 percutaneous transluminal coronary angioplasties (PTCAs) were performed. Of these, 67% (n = 20) were carried out in patients with NSTEMI, while 33% (n = 10) in individuals with STEMI. In 30% of the patients (n = 16), no significant atherosclerotic lesions were found in the coronary arteries, corresponding to 38% (n = 15) of all NSTEMI cases, and 7% (n = 1) of all STEMI cases. Six percent of the patients (n = 3) were referred for urgent coronary artery bypass grafting. The following cardiovascular risk factors were identified: diabetes in 45% of the patients (n = 24), hypertension in 53% (n = 28), history of coronary artery disease in 36% (n = 19), smoking in 32% (n = 17), and renal insufficiency in 13% (n = 7).
In the same period 1 year before the pandemic year, that is, from March 15 to December 5, 2019, a total of 3559 patients were hospitalized in the Cardiology Department and 414 coronary artery angiographies were performed in the catheterization laboratory in the patients diagnosed with ACS. Among them, 35% (n = 146) had STEMI and 65% (n = 268) had NSTEMI. A total of 388 PTCA procedures were performed: 36% (n = 141) in STEMI and 64% (n = 247) in NSTEMI patients. Coronary arteries without significant atherosclerotic stenosis were found in 3% of the STEMI patients (n = 5) and 8% of the NSTEMI patients (n = 21).
In comparison with the year 2019, during the COVID‑19 pandemic (2020), NSTEMI was more often diagnosed among patients with ACS (74% vs 65%; P = 0.048). The patients with NSTEMI treated in 2020 were also more likely to be diagnosed with no significant coronary artery stenosis than the individuals treated in the previous year (n = 15 [38%] vs n = 21 [8%]; P <0.001). The results are presented in Figure 1.
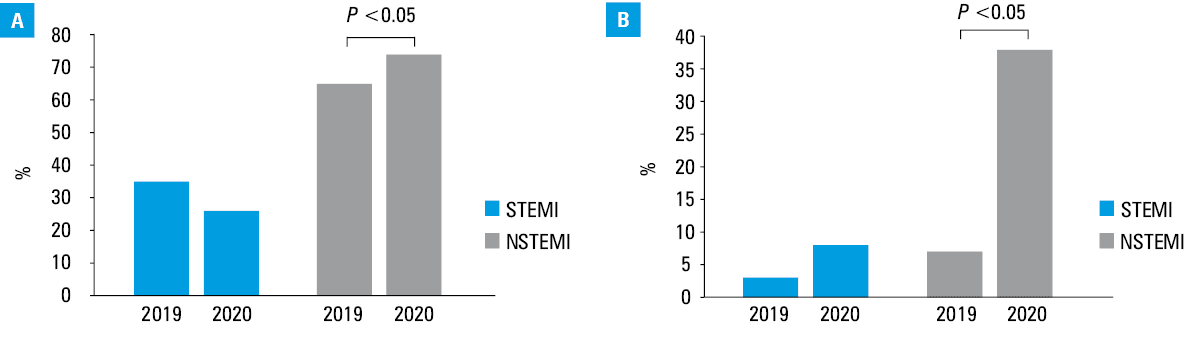
Abbreviations: NSTEMI, non‑ST‑segment elevation myocardial infarction; STEMI, ST‑segment elevation myocardial infarction
During the first 2 waves of the pandemic, from March 15 to December 5, 2020, 19% of the patients (n = 10) hospitalized in the Department of Cardiology for SARS‑CoV‑2 infection with coexisting ACS were in a very severe condition, requiring external ventilation and the presence of an anesthetic team in the catheterization laboratory. Two patients (4%) died during the procedure.
A total of 39 deaths were recorded in the Cardiology Department during the first 2 pandemic waves. During the same period in 2019, a total of 17 deaths were recorded (P <0.001). In 2019, no patient died during coronary angiography in the catheterization laboratory.
Coronary angiography in patients with an active SARS‑CoV‑2 infection was performed in 23 cases (43%) throughout the analyzed period of 2020. By October 31, 2020, the vast majority of the procedures (88%) were carried out in patients negative for COVID‑19. This was due to the fact that in all ACS cases where coronary angiography could be deferred (NSTEMI, GRACE score <140), it was performed after the patient had tested negative for SARS‑CoV‑2. All the patients hospitalized after March 15, 2020 tested positive for COVID‑19. They were also transferred from other centers due to a confirmed SARS‑CoV‑2 infection.
All the procedures followed a strict hygiene regimen and a full range of personal protective equipment was used.
Discussion
Data from various centers in Poland and around the world indicate that the number of patients hospitalized for myocardial infarction (MI) in 2020 was lower by 40% than in 2019.3 The reasons include fewer patients reporting to health care facilities, but also limited access to these facilities during the pandemic.4 It is worth pointing out that a relatively small number of patients infected with SARS‑CoV‑2 require interventional cardiac treatment for ACS. This is especially true for patients diagnosed with NSTEMI, 38% of whom had no significant coronary artery stenosis on coronary angiography in our study. COVID‑19 largely causes a type 2 MI, resulting from the SARS‑CoV‑2 infection itself, and associated with respiratory and hemodynamic abnormalities. Therefore, some patients can be treated conservatively.
The patients included in our study were referred for coronary angiography according to the fourth universal definition of MI.5 A point of concern is that a relatively large proportion of the patients were in a very serious condition and required external ventilation during the procedure. This may be due to the fact that the patients delayed medical consultations for fear of infection or isolation, prolongation of the procedures because of the use of personal protective equipment, but also a delayed diagnosis of ACS because of nonspecific symptoms.
The data presented here show that a relatively small number of patients infected or suspected of being infected with SARS‑CoV‑2 required interventional cardiac treatment for ACS. Therefore, some patients diagnosed with type 2 MI due to COVID‑19 might be treated conservatively. At the same time, it was shown that the prevalence of coronary arteries without significant stenosis was significantly higher among the patients with NSTEMI and COVID‑19 hospitalized in 2020 than those with NSTEMI treated in the corresponding period 1 year before the pandemic (2019).
- Alshaikh MK, Alotair H, Alnajjar F, et al. Cardiovascular risk factors among patients infected with COVID‑19 in Saudi Arabia. Vasc Health Risk Manag. 2021; 17: 161‑168. | Crossref
- Nowak B, Szymański P, Pańkowski I, et al. Clinical characteristics and short‑term outcomes of coronavirus disease 2019: retrospective, single‑center experience of designated hospital in Poland. Pol Arch Intern Med. 2020; 130: 407‑411. | Crossref
- Gąsior M, Gierlotka M, Tycińska A, et al. Effects of the coronavirus disease 2019 pandemic on the number of hospitalizations for myocardial infarction: regional differences. Population analysis of 7 million people. Kardiol Pol. 2020: 78: 1039‑1042. | Crossref
- Cameli M, Pastore MC, Mandoli GE, et al. COVID‑19 and acute coronary syndromes: current data and future implications. Front Cardiovasc Med. 2021; 7: 593496. | Crossref
- Thygesen K, Alpert JS, Jaffeet AS, et al; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019; 40: 237‑269.
ARTICLE INFORMATION