Acute-on-chronic pulmonary embolism-induced right ventricular failure salvaged by combined catheter-directed therapy and levosimendan infusion



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Acute-on-chronic pulmonary embolism-induced right ventricular failure salvaged by combined catheter-directed therapy and levosimendan infusion
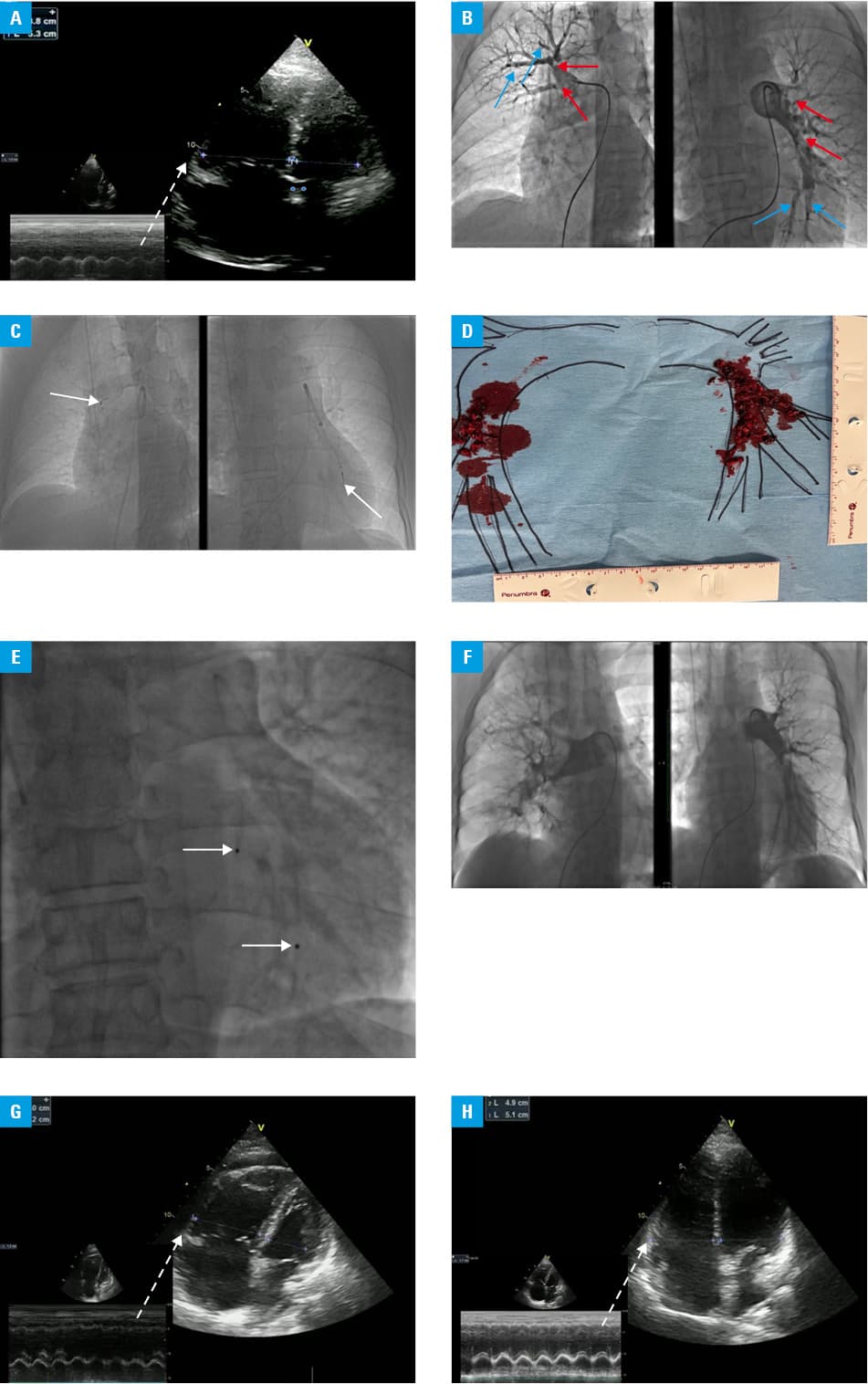
A 52‑year‑old man was admitted to a local hospital due to intermediate‑high risk pulmonary embolism (PE). As 48‑hour intravenous anticoagulation was ineffective, our institutional PE response team (PERT) qualified the patient for catheter‑directed therapy (CDT).1 Initial examination on admission to our department revealed a heart rate (HR) of 120 bpm, respiratory rate (RR) 32/min, saturation (SaO2) 90% despite oxygen supplementation (flow rate [FR] 12 l/min), blood pressure 98/68 mm Hg, elevated troponin (0.5 ng/ml; normal range [NR] <0.01 ng/ml), and N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP; 8548 pg/ml; NR, <125 pg/ml). Echocardiography demonstrated increased right ventricular to left ventricular ratio (RV/LV, 1.4), high‑velocity tricuspid regurgitation (4.5 m/s), and decreased tricuspid annular plane systolic excursion (TAPSE, 10 mm) (Figure 1A). Pulmonary angiography showed dilated pulmonary arteries (PAs) with web- and ring‑like thromboembolic lesions indicating a chronic process overlapping with bilateral fresh emboli (Figure 1B). The mean pulmonary arterial pressure (mPAP) was 55 mm Hg and pulmonary vascular resistance (PVR) was 9 Wood Units (WU). Catheter‑directed mechanical thrombectomy with an 8‑F Indigo CAT8 XTORQ catheter (Penumbra, Alameda, California, United States) was performed in the right and left PA branches. Additionally, low‑dose thrombolysis (12 mg of alteplase/12 hours) was carried out through a 5‑F Fountain catheter (Merit Medical, South Jordan, Utah, United States) placed in the left lateral segmental PA (Figure 1C-1F). The procedure resulted in a significant thrombus burden reduction and hemodynamic improvement (mPAP, 50 mm Hg; HR, 90 bpm; SaO2, 94% [FR, 3 l/min on a nasal cannula]). However, after 2 days the patient’s condition deteriorated, HR increased to 120 bpm with an expansion in systemic congestion (6 l/48 hours with fluid accumulation), elevation of troponin I (0.8 ng/ml) and NT‑proBNP (9530 pg/ml), and enlargement of RV/LV ratio (52 mm/30 mm = 1.7) (Figure 1G), but without an increase in RR (20/min) or oxygen demand (SaO2, 94% [FR 3 l/min on the nasal cannula]). The computed tomography scan did not reveal PE clot burden reload. PERT reconsulted the patient and qualified him for surgical embolectomy with mechanical circulatory support but the patient refused. Intensive vasopressor therapy with noradrenaline (0.3 µg/kg/min) and dobutamine (8 µg/kg/min), with intravenous furosemide (20 mg/h) infusions were started. Despite the therapy, the patient continued to deteriorate and PERT proposed levosimendan as a reasonable therapeutic option. The patient was given detailed information and provided written informed consent. A 24 hour infusion of levosimendan (0.2 µg/kg/min, no initial bolus) was implemented without complications. The patient’s condition began to improve within several hours and he was independent of vasopressors within 36 hours (Figure 1H). He was discharged home 4 days later, on apixaban anticoagulation. Three months later, chronic thromboembolic pulmonary hypertension with mPAP 36 mm Hg and PVR 3.5 WU was confirmed. The patient started a targeted therapy with riociguat and underwent 4 sessions of balloon pulmonary angioplasty (residual mPAP 25 mm Hg, PVR 2.5 WU).
Repeated episodes of PE can persistently increase PAP and depress RV function leading to an overt event with rapid deterioration.2,3 We describe a life‑threatening acute‑on‑chronic PE treated with CDT supported by levosimendan infusion. This report showed that levosimendan may have favorable effects on RV contractility in acute settings.4,5
- Araszkiewicz A, Kurzyna M, Kopeć G, et al. Pulmonary embolism response team: a multidisciplinary approach to pulmonary embolism treatment. Polish PERT Initiative Report. Kardiol Pol. 2021; 79: 1311‑1319. | Crossref
- Araszkiewicz A, Sławek‑Szmyt S, Jankiewicz S, et al. Continuous aspiration thrombectomy in high- and intermediate‑high‑risk pulmonary embolism in real‑world clinical practice. J Interv Cardiol. 2020; 2 020: 4191079. | Crossref
- Pruszczyk P, Skowrońska M, Ciurzyński M, et al. Assessment of pulmonary embolism severity and the risk of early death. Pol Arch Intern Med. 2021; 131: 16134. | Crossref
- Lyhne MD, Dragsbaek SJ, Hansen JV, et al. Levosimendan, milrinone, and dobutamine in experimental acute pulmonary embolism. Pulm Circ. 2021; 11: 20458940211022977. | Crossref
- Tycińska A, Gierlotka M, Bugajski J, et al. Levosimendan in the treatment of patients with acute cardiac conditions: an expert opinion of the Association of Intensive Cardiac Care of the Polish Cardiac Society. Kardiol Pol. 2020; 78: 825‑834. | Crossref
ARTICLE INFORMATION