Combined large-cell neuroendocrine carcinoma and atypical carcinoid of the thymus presenting as ectopic Cushing syndrome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Combined large-cell neuroendocrine carcinoma and atypical carcinoid of the thymus presenting as ectopic Cushing syndrome
Cushing syndrome (CS) is a well‑known clinical presentation of glucocorticoid excess. However, diagnosis and treatment may still be challenging. We present a case of a young man with ectopic CS (ECS) due to combined large‑cell neuroendocrine carcinoma (LCNEC) and atypical carcinoid (AC) of the thymus.
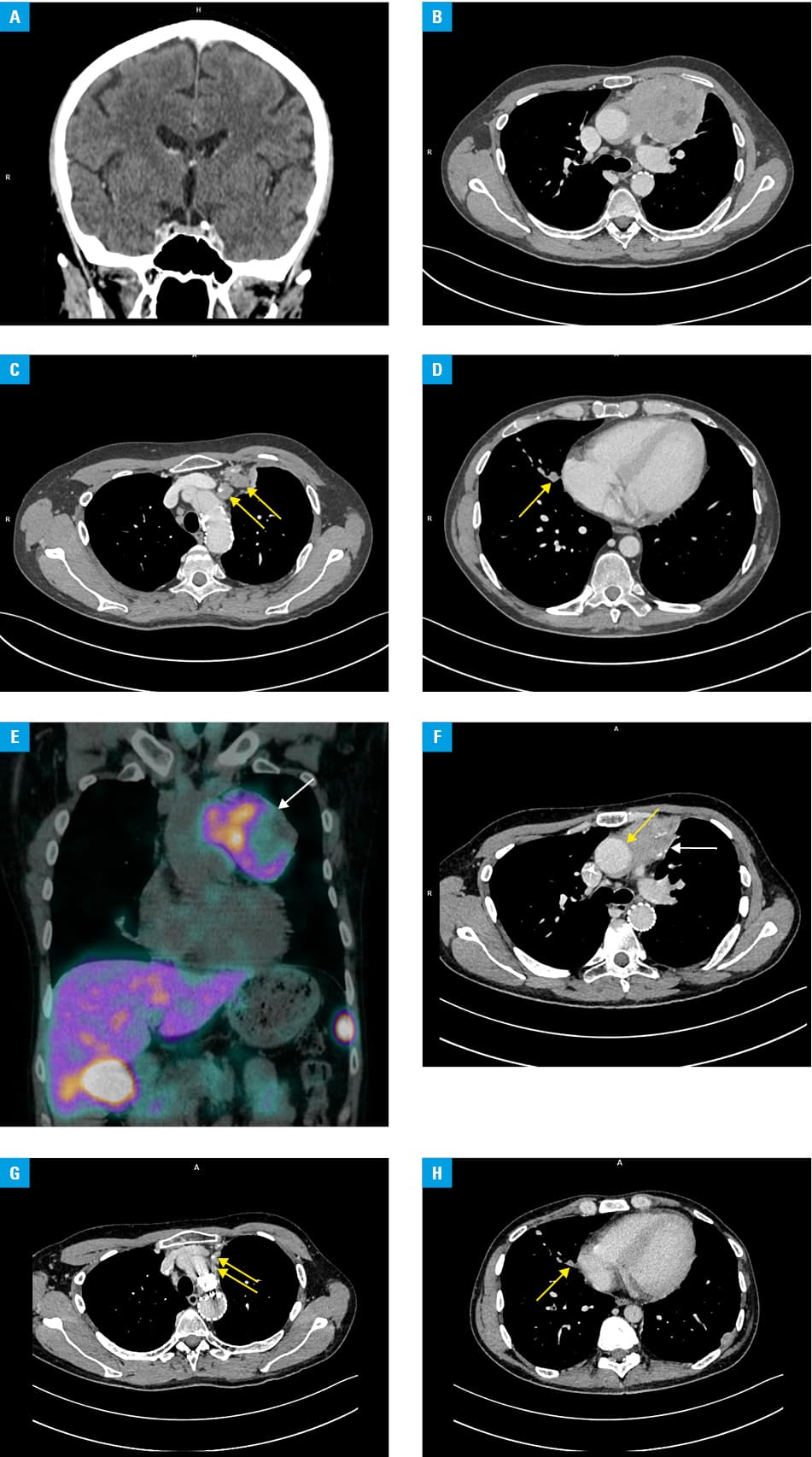
The patient aged 33 years was first admitted to the hospital in February 2020 because of de novo diabetes (a few‑week history of polydipsia and polyuria) and acute worsening of previously controlled hypertension. On physical examination, generalized hyperpigmentation and purple striae were observed. Routine blood tests revealed severe hypokalemia (1.89–2.05 mmol/l; reference range [RR], 3.50–5.10 mmol/l) and metabolic alkalosis (pH, 7.56–7.58; RR, 7.35–7.45; HCO3, 49.7–51.3 mmol/l; RR, 21–27 mmol/l). Chest radiography showed widening of the superior‑left mediastinum. Additional tests were performed and yielded the following results: late‑night serum cortisol 493–768 nmol/l (RR for 4–8 pm, 74–286 nmol/l), 24‑hour urinary free cortisol 1929 nmol/24 h (RR, 12–486 nmol/24 h), plasma adrenocorticotropic hormone (ACTH) 313–317 pg/ml (RR, 7.2–63.3 pg/ml), 8 mg overnight dexamethasone suppression test cortisol 751 nmol/l (RR, <50 nmol/l). The patient was diagnosed with ACTH‑dependent CS. No abnormalities were found on pituitary computed tomography (CT) (magnetic resonance imaging contraindicated due to aortic stent‑graft implantation) (Figure 1A). However, CT showed pathologic masses in the mediastinum (Figure 1B–1D). Videothoracoscopic biopsy of the mediastinal tumor revealed combined LCNEC and AC, most likely of thymic origin (Ki67 proliferative inde × 30%, locally up to 60%; chromogranin A+, CD56+, napsin A-, CD117+, CD5-). Subsequently, technetium‑99m‑hydrazinonicotinyl‑Tyr3‑octreotide (99mTc‑EDDA/HYNIC‑TOC) SPECT‑CT was performed, showing heterogeneous tracer uptake within the lesions (Figure 1E). Chemotherapy with paclitaxel and carboplatin in a weekly metronomic dosing was initiated in April 2020 (26 cycles were given), together with somatostatin analogs (lanreotide 120 mg every 28 days). Treatment with metyrapone was implemented simultaneously to normalize hypercortisolemia (500–1000 mg daily, in divided doses, depending on clinical and laboratory parameters). Between April and May 2021, the patient received radiotherapy to the mediastinum (30 Gy/10 fractions). The patient has been under control for 24 months, his condition has been good, and biochemical parameters have stabilized (24‑hour urinary free cortisol 423–510 nmol/24 h; plasma ACTH 213–295 pg/ml; morning serum cortisol 297–371 nmol/l [RR for 6–10 am, 172–497 nmol/l]). Somatostatin analogs and metyrapone are continued. According to the Response Evaluation Criteria In Solid Tumors 1.1, stable disease was observed in April 2022 (Figure 1F–1H). 99mTc‑EDDA/HYNIC‑TOC SPECT‑CT and 2‑deoxy‑2-[18 F]fluoro‑D‑glucose positron emission tomography‑CT (18F‑FDG PET‑CT) are scheduled to characterize the currently observed lesions.
ECS accounts for about 10%–20% of all endogenous CS cases, with an incidence estimated at 1.4 cases per 10 million per year, and is typically associated with rapid symptom progression (catabolic symptoms, profound hypokalemia, severe hypertension, hyperglycemia).1 Small cell lung cancer and pulmonary neuroendocrine tumors (NETs) are the main reasons for ECS.1 Thymic location of NETs is uncommon and often associated with poor prognosis, although this varies depending on histopathology (including typical carcinoid, AC, LCNEC, and small cell neuroendocrine cancer).1 ECS associated with thymic AC or LCNEC is exceedingly rare and further complicates management. When possible, surgical resection is advised. Typical carcinoid and AC often respond to somatostatin analogs.2 No standard treatment protocol has been established for thymic LCNEC due to its rarity, although the regimen used in pulmonary LCNEC is suggested.3 99mTc‑HYNIC‑octreotide SPECT‑CT or 68Ga‑DOTATATE PET‑CT may be useful diagnostic tools in the case of ECS, especially when anatomical studies fail to find the location (other potential techniques include 18F‑FDG or 18F‑DOPA PET). However, their sensitivity is also limited.4 Treatment options for hypercortisolism include resection of the primary tumor (if possible), pharmacotherapy (including steroidogenesis inhibitors, eg, metopirone or osilodrostat), or, in the case of resistance to other methods, bilateral adrenalectomy.5 Although significant progress has been made in diagnostic methods and treatment modalities, ECS is still a challenging condition and requires cooperation of multidisciplinary teams.
- Young J, Haissaguerre M, Viera‑Pinto O, et al. Cushing’s syndrome due to ectopic ACTH secretion: an expert operational opinion. Eur J Endocrinol. 2020; 182: 29‑58. | Crossref
- Baudin E, Caplin M, Garcia‑Carbonero R, et al. Lung and thymic carcinoids: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow‑up. Ann Oncol. 2021; 32: 439‑451. | Crossref
- Jia R, Sulentic P, Xu JM, Grossman AB. Thymic neuroendocrine neoplasms: biological behaviour and therapy. Neuroendocrinology. 2017; 105: 105‑114. | Crossref
- Senanayake R, Gillett D, MacFarlane J, et al. New types of localization methods for adrenocorticotropic hormone‑dependent Cushing’s syndrome. Best Pract Res Clin Endocrinol Metab. 2021; 35: 101513. | Crossref
- Fleseriu M, Auchus R, Bancos I, et al. Consensus on diagnosis and management of Cushing’s disease: a guideline update. Lancet Diabetes Endocrinol. 2021; 9: 847‑875. | Crossref
ARTICLE INFORMATION