Hereditary hemorrhagic telangiectasia (HHT) or Osler‑Weber‑Rendu syndrome is an autosomal dominant genetic disease, mainly caused by mutations in the ENG, ACVRL1, and SMAD4 genes.1 Incidence varies between 1 in 5000 and 1 in 80 000 people.2,3
Typical clinical presentation includes epistaxis and skin and mucosal telangiectasias observed in 50% to 80% of patients.
A 49‑year‑old woman with varicose veins of the lower limbs and trace mitral and aortic regurgitation, was referred by her primary care physician for diagnostics of hepatopathy in 2013. She was asymptomatic, with slightly elevated aminotransferase levels (Supplementary material, Table S1). Abdominal ultrasound, esophagogastroduodenoscopy, and liver biopsy findings were normal.
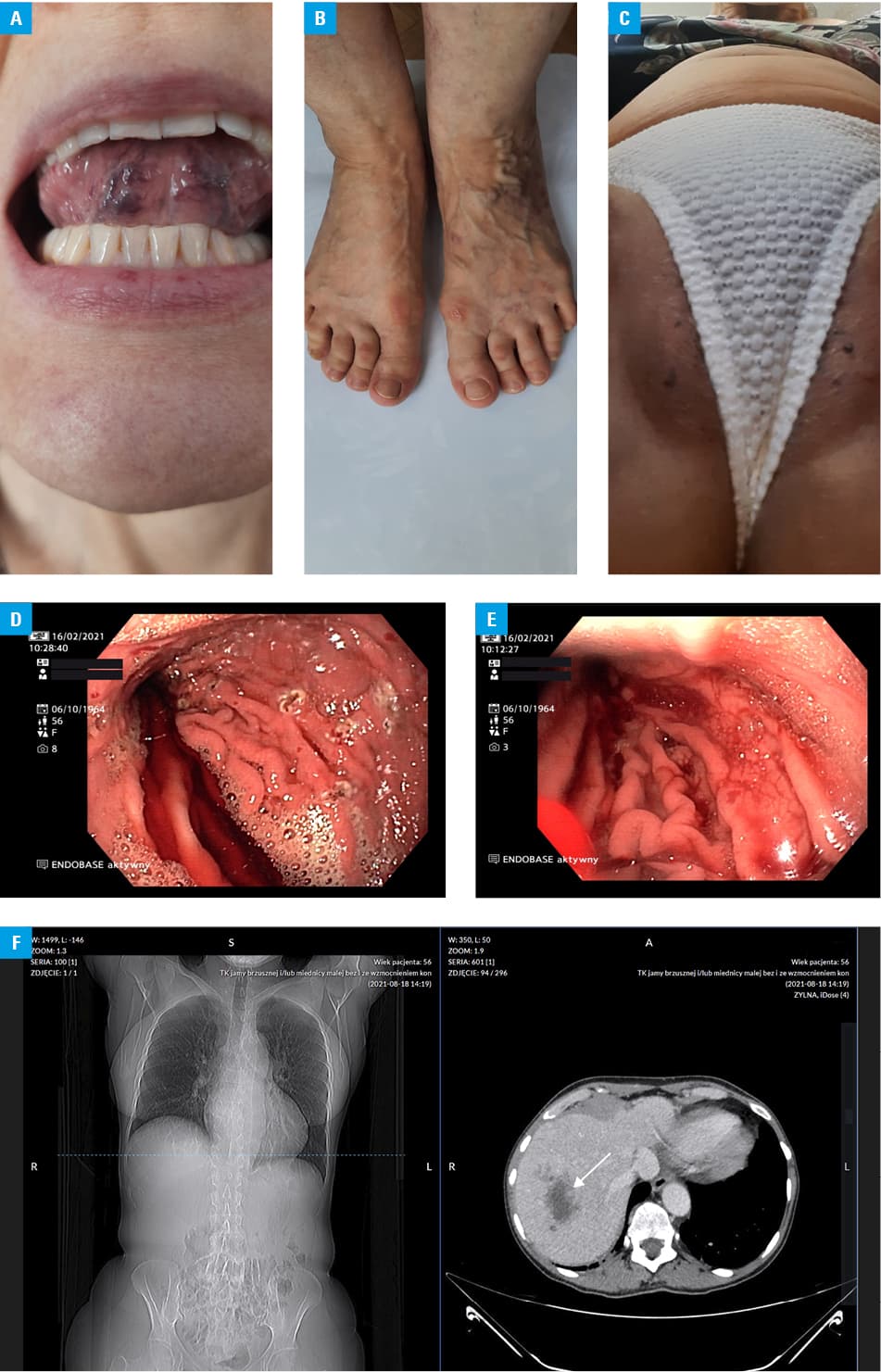
The patient was hospitalized in 2016 for recurrent epistaxis, and minor telangiectasias of the nasal mucosa were then observed. Gastroscopy revealed erythematous gastritis, while colonoscopy was normal. Abdominal computed tomography (CT) showed numerous scattered telangiectasias, very wide tortuous vessel branches of the hepatic artery, and contrasting hepatic veins, confirming the presence of arteriovenous fistulas, leading to HHT diagnosis. The patient presented here fulfils all of the 4 Curacao criteria for diagnosis since her daughter presents the symptoms of HHT (Figure 1A–1C).
On November 6, 2020, the patient was admitted to a hospital due to a SARS‑CoV‑2 infection. She presented with a fever up to 39.5 ºC, headache, sore throat, and generalized myalgia. On examination, she was tachypneic, and her blood oxygen saturation was 84%. Chest CT showed patchy opacities with ground‑glass areas. Treatment included passive oxygen therapy, thromboprophylaxis with a low‑molecular‑weight heparin–enoxaparin 40 mg/0.4 ml daily, and a nonsteroidal anti‑inflammatory drug acetamonphen 1.5 g daily. Six days after the admission, massive epistaxis occurred with a hemoglobin drop to 4.7 g/dl. The patient received 3 units of packed red blood cells (PRBCs) and was transferred to the intensive care unit. Due to increasing circulatory and respiratory failure, she required invasive mechanical ventilation. Sudden cardiac arrest occurred, followed by successful resuscitation and mechanical ventilation in biphasic positive airway pressure (BIPAP) mode with FiO2 0.8, positive end‑expiratory pressure (PEEP) 8 cm H2O, saturation 96%; circulation was stimulated with norepinephrine infusion. Pharmacotherapy included noradrenaline, amiodaron, antibiotics, diuretics, and steroids. After several days, clinical improvement was observed, and the patient was extubated on December 4, 2020.
Hospitalization continued at an internal medicine department until February 8, 2021. Discharge diagnoses included Staphylococcus epidermidis sepsis, hypoxic‑ischemic encephalopathy, cerebellar infarction, peripheral polyneuropathy, right foot drop, and periodic epistaxis. The patient required a transfusion of 4 units of PRBCs and 1 g of iron.
She was readmitted 4 days after her discharge to a rehabilitation hospital due to suspected rebleeding. Gastroscopy showed gastric mucosa with numerous small telangiectasias, covered with streaks of hemolyzed blood. Argon plasma coagulation was performed on over 30 actively bleeding lesions in the stomach (Figure 1D and 1E).
The patient was hospitalized again in August of 2021 due to abdominal pain, and she was diagnosed with bleeding lesions in the stomach and hematoma in the right liver lobe. In the following months, the patient underwent several hospitalizations at our department and 4 argon beamer coagulation treatments for angiectasia in the stomach. Liver hematoma resorbed, and no significant vascular malformations were found in the lungs, central nervous system, spleen, and kidneys (Figure 1F). The patient was vaccinated with the Spikevax‑mRNA‑1273 vaccine on June 15, 2021 and on July 27, 2021. For the next 3 days after the vaccination she had a fever of up to 40 °C and suffered from arthralgia and general fatigue.
On the pathophysiological level, the basic causes of HHT are disturbances of angiogenesis and of the vascular wall integrity that result in telangiectasia, arteriovenous malformations, and arteriovenous fistulas in the gastrointestinal tract, respiratory tract, and brain.4 The impact of endothelial damage is emphasized in the pathogenesis of COVID‑19. In the discussed case, overlapping of these 2 processes led to HHT progression and gastrointestinal and liver bleeding.
SARS‑CoV‑2 infection induced progression of HHT and the occurrence of clinically evident bleeding.
- Berg JN, Gallione CJ, Stenzel TT, et al. The activin receptor‑like kinase 1 gene: genomic structure and mutations in hereditary hemorrhagic telangiectasia type 2. Am J Hum Genet. 1997; 61: 60‑67. | Crossref
- Dakeishi M, Shioya T, Wada Y, et al. Genetic epidemiology of hereditary hemorrhagic telangiectasia in a local community in the northern part of Japan. Hum Mutat. 2002; 19: 140‑148. | Crossref
- Bideau A, Plauchu H, Brunet G, et al. Epidemiological investigation of Rendu‑Osler disease in France: its geographical distribution and prevalence. Popul. 1989; 44: 3‑22. | Crossref
- Shovlin CL, Letarte M. Hereditary hemorrhagic telangiectasia and pulmonary arteriovenous malformations: issues in clinical management and review of pathogenic mechanisms. Thora × 1999; 54: 714. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION