A nomogram to predict in-hospital mortality in post-cardiac arrest patients: a retrospective cohort study
Key words: cardiac arrest, in-hospital mortality, MIMIC-IV database, prognosis, risk prediction model



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A nomogram to predict in-hospital mortality in post-cardiac arrest patients: a retrospective cohort study
Introduction: Nomograms of prognosis in patients with a history of cardiac arrest (CA) have been established. However, there are some shortcomings and interferences in their clinical application.
Objectives: Our study aimed at developing a utility nomogram to predict the risk of in‑hospital death in post‑CA patients.
Patients and methods: We retrospectively extracted data from the MIMIC‑IV database. The least absolute shrinkage and selection operator logistic regression and multivariable logistic regression were used to investigate independent risk factors. A nomogram defined as a prediction model was established for these independent risk factors. The model performance was measured by examining discrimination (area under the receiver operating characteristic curve [AUC]), calibration (calibration curve analysis), and utility (decision curve analysis [DCA]).
Results: A total of 1724 post‑CA patients were enrolled in the study. Of those, 788 survived and 936 died. The incidence of in‑hospital death was 54.3%. In this nomogram, the predictors included age, malignant cancer, bicarbonate, blood urea nitrogen, sodium, heart rate, respiratory rate, temperature, SPO2, norepinephrine prescription, and lactate level. The internally validated nomogram showed good discrimination (AUC 0.801; 95% CI, 0.775–0.835). The calibration curve analysis and DCA confirmed that this prediction model can be clinically useful.
Conclusions: We established a risk prediction model based on the admission characteristics to accurately predict the clinical outcome in post‑CA patients. The nomogram might help with the risk identification and individual clinical interventions.
What's new?
The evaluation of clinical outcomes could reduce the in‑hospital mortality of patients with previous cardiac arrest (CA). Predictors of post‑CA outcomes to reduce in‑hospital mortality are yet to be identified. We built a clinical prediction model capable of identifying the post‑CA patients at a risk of in‑hospital mortality. This model provided an excellent prediction of in‑hospital death and could be applied by clinicians as a reference to prevent the fatal events in post‑CA patients.
Introduction
Cardiac arrest (CA) is common worldwide, as approximately 292 000 adults experience an in‑hospital CA (IHCA),1 and 420 000 people are diagnosed with out‑of‑hospital CA (OHCA) in the United States each year.2 Recently, a study on the nationwide emergency department sample from the United States reported that the in‑hospital survival rate of all CAs was only 28.7%. Furthermore, the incidence of CA is increasing year by year.3 Early evaluation of in‑hospital mortality in post‑CA patients plays a vital role in improving their prognosis and reducing mortality.4 This approach could be an effective reference point for in‑hospital treatment and integrated post‑resuscitation care. Clinical risk models are useful tools for evaluating the risk of adverse clinical outcomes.5-9 In recent years, clinical risk models have been widely applied to evaluate the prognosis of critical patients. More than 81 clinical risk models of CA have been published at present. However, only a small number of them have been rigorously validated.10
Currently, the prediction models of in‑hospital death in post‑CA patients have been established. However, there are still some shortcomings and interferences. These defects create inaccuracies in the model application and provide erroneous guidance for clinicians. In addition, these models mainly focused on the onset information of CA, such as a location, emergency medical services arrival time, whether the event had been witnessed, and so on.11-13 However, the patients’ clinical data after hospitalization are also likely to be related to in‑hospital death. Herein, we aimed at building and developing a novel nomogram based on the clinical information after hospitalization in post‑CA patients. The nomogram can refine the scores of each predictor to separately evaluate the probability of death. It is advisable in clinical practice to identify the post‑CA patients at a higher risk of in‑hospital death. This study would be of great value for decision‑making, treatment, and intensive care in the post‑CA patients.
Patients and Methods
Data source
We obtained primary data from the MIMIC‑IV database. It contains all medical record numbers corresponding to the patients who were admitted to an intensive care unit (ICU) or emergency department between 2008 and 2019 in the Beth Israel Deaconess Medical Center. The current version of the MIMIC‑IV database is 1.0. After completion of an online training at the National Institutes of Health, one of our authors (CJ, certification ID: 8979131) was granted permission to access the database. Our study relied exclusively on publicly available and anonymized data. Therefore, it did not require individual patient permission. We conducted the study according to relevant guidelines aimed at the patients’ privacy protection.
Population selection
In the MIMIC‑IV database, we identified adult patients (>18 years old) diagnosed with CA at a hospital admission. The codes of the data extraction were the International Classification of Diseases, Ninth Revision (ICD‑9) diagnosis code 4275 and the International Classification of Diseases, Tenth Revision (ICD‑10) diagnosis codes I46, I462, I468, and I469. CA was defined as the cessation of cardiac activity characterized by unresponsiveness, no normal breathing, and no signs of circulation.14 The exclusion criteria included pregnancy and postpartum, unavailable medical records, missing blood biochemical and blood gas analysis data, and missing survival outcome data.
Clinical and laboratory data
Data records included the patient characteristics and data on comorbidities, vital signs, and laboratory tests. We extracted the patient’s first recorded vital sign data and laboratory data following the admission. The vital signs included body temperature, systolic blood pressure, diastolic blood pressure, mean blood pressure (MBP), heart rate, respiratory rate, and pulse oximetry–derived oxygen saturation (SPO2). The laboratory data included creatinine, anion gap, pH, lactate, blood urea nitrogen (BUN), chloride, glucose, hemoglobin, hematocrit, white blood cell count, platelet count, serum potassium, serum sodium, calcium, and international normalized ratio (INR). During the hospitalization, the therapy included vasoactive medications (norepinephrine) and continuous renal replacement therapy (CRRT). Each patient’s acute physiology score II15 and sequential organ failure assessment16 were also computed. The primary end point was in‑hospital death, defined as mortality status at the hospital discharge.
Statistical analysis
Firstly, we deleted the variables with significant data missing (over 20% of the total data), and for the variables with missing data below 20% of the total data, we used multiple imputation to impute the missing data.17 The new dataset was divided into development and validation cohorts (approximately 2:1). We applied development and validation datasets to establish and validate the prediction model, respectively. Continuous variables were expressed as median (interquartile range [IQR]) or mean (SD). Categorical variables were expressed as numbers (percentages). We performed group comparisons using the t test or the Wilcoxon rank‑sum test for continuous variables and the χ2 test or the Fisher exact test for categorical variables. Secondly, the least absolute shrinkage and selection operator (LASSO) logistic regression analysis were used to identify candidate predictors with large regression coefficients. Thirdly, multivariable logistic regression analysis was performed to identify independent risk factors and establish the risk model based on the training dataset. In the model, the score of each predictor was calculated based on the coefficients of logistic regression variables. A nomogram was used to visualize the model. The model discrimination was assessed by receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) of 0.75 or more indicated good discrimination. The prediction accuracy of the risk model was determined by calibration plots and the Hosmer–Lemeshow test. The decision curve analysis (DCA) evaluated the clinical utility of the nomogram by quantifying net benefits against a range of threshold probabilities. These results were expressed by odds ratios (ORs) with 95% CIs. All the tests were 2‑tailed, and a P value below or equal to 0.05 was considered significant. The statistical analyses were performed with R software version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of the study patients
A total of 1724 patients diagnosed with post‑CA syndrome, of whom 1055 were men and 669 were women, were enrolled in this study. The flow chart of participant enrollment in this study is shown in Supplementary material, Figure S1. The average (SD) age was 66.36 (16.28) years. As many as 936 patients died during the hospitalization, 551 (58.87%) of whom were men. The in‑hospital death incidence was 54.3% (936/1724). As many as 42.52% of the patients had congestive heart failure and 29.18% had a history of myocardial infarction. Further 12.47% had a history of malignant cancer or malignant cancer. The survivors had higher blood pressure, SPO2, temperature, and hemoglobin levels. The patients who received norepinephrine and CRRT therapy were more likely to die in the hospital. There were no significant differences in sex or comorbidities between the survival group and the death group except for malignant cancer (Table 1). The whole sample was randomly divided into a training set and a test set with the proportion of 7:3, and there was no significant difference in the variables between the training set and the test set (Table 2).
Characteristics | Total (n = 1724) | Survival (n = 788) | Death (n = 936) | P value |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
SI conversion factors: to convert anion gap to mmol/l, multiply by1, BUN to mmol/l, by 0.357, creatinine to µmol/l, by 88.4, glucose to mmol/l, by 0.0555, hemoglobin to g/l, by 10.
Abbreviations: APSII, acute physiology score II; bpm, beats per minute for heart rate; bpm, breath per minute for respiratory rate; BUN, blood urea nitrogen; DBP, diastolic blood pressure; ICU, intensive care unit; INR, international normalized ratio; MBP, mean blood pressure; SBP, systolic blood pressure; SOFA, sequential organ failure assessment; SPO2, pulse oximetry–derived oxygen saturation; WBC, white blood cell | ||||
Age, y, mean (SD) | 66.36 (16.28) | 64.88 (15.89) | 67.61 (16.5) | <0.001 |
Male sex | 1055 (61.19) | 504 (63.96) | 551 (58.87) | 0.31 |
SBP, mm Hg, mean (SD) | 112.36 (17.08) | 115.65 (14.77) | 109.60 (18.36) | <0.001 |
DBP, mm Hg, mean (SD) | 61.78 (11.86) | 62.81 (10.84) | 60.91 (12.60) | <0.001 |
MBP, mm Hg | 76.44 (11.87) | 78.40 (10.26) | 74.80 (12.85) | <0.001 |
Heart rate, bpm, mean (SD) | 86.25 (18.66) | 82.40 (16.60) | 89.48 (19.66) | <0.001 |
Respiratory rate, bpm, mean (SD) | 21.15 (4.54) | 20.08 (4.18) | 22.06 (4.63) | <0.001 |
Temperature, °C, mean (SD) | 36.48 (1.07) | 36.73 (0.79) | 36.27 (1.21) | <0.001 |
SPO2, %, mean (SD) | 96.16 (5.87) | 97.59 (2.22) | 94.95 (7.49) | <0.001 |
Comorbidities | ||||
Diabetes | 638 (37.01) | 292 (37.06) | 346 (36.97) | >0.99 |
Hypertension | 620 (35.96) | 296 (37.56) | 324 (34.62) | 0.41 |
Myocardial infarction | 503 (29.18) | 244 (30.96) | 259 (27.67) | 0.29 |
Congestive heart failure | 733 (42.52) | 362 (45.94) | 371 (39.64) | 0.10 |
Chronic pulmonary disease | 463 (26.86) | 220 (27.92) | 243 (25.96) | 0.52 |
Malignancy | 215 (12.47) | 68 (8.63) | 147 (15.71) | <0.001 |
Laboratory parameters | ||||
Anion gap, mEq/l | 16.50 (14.00–20.25) | 16.50 (14.00–20.25) | 18.00 (15.00–22.125) | <0.001 |
BUN, mg/dl | 26.50 (18.00–41.50) | 22.75(16.00–36.50) | 29.50 (19.50–46.63) | <0.001 |
Bicarbonate, mmol/l | 21.00 (17.50–24.50) | 22.50 (19.50–25.00) | 19.00 (16.00–22.50) | <0.001 |
Creatinine, mg/dl | 1.40 (0.95–2.275) | 1.20 (0.85–1.95) | 1.60 (1.00–2.46) | 0.11 |
Chloride, mmol/l | 104.00 (99.5–108.00) | 104.00 (100.00–107.50) | 105.00 (99.5–108.50) | 0.09 |
Glucose, mg/dl | 165.00 (131.50–220.25) | 151.75 (124.50–200.13) | 172.75 (136.00–243.25) | <0.001 |
Hematocrit, % | 32.97 (7.08) | 33.03 (7.13) | 32.83 (6.97) | 0.04 |
Hemoglobin, g/dl | 10.69 (2.42) | 10.71 (2.45) | 10.64 (2.36) | <0.001 |
WBC, 109/l | 12.60 (9.15–16.6) | 13.05 (9.40–17.78) | 13.60 (9.70–18.35) | <0.001 |
Platelets, 109/l | 194.75 (145.00–258.50) | 193.00 (138.25–264.75) | 185.0 (126.88–258.13) | 0.009 |
pH | 7.32 (7.24–7.38) | 7.35 (7.28–7.39) | 7.29 (7.20–7.36) | <0.001 |
Lactate, mmol/l | 3.10 (1.85–5.30) | 2.35 (1.60–3.80) | 4.23 (2.35–6.80) | <0.001 |
Potassium, mmol/l | 4.30 (3.90–4.80) | 4.25 (3.90–4.70) | 4.30 (3.90–4.90) | 0.03 |
INR | 1.40 (1.20–1.80) | 1.30 (1.15–1.55) | 1.50 (1.25–2.10) | <0.001 |
Sodium, mmol/l | 139.00 (136.00–142.00) | 138.50 (136.00–141.00) | 139.50 (136.00–143.00) | 0.001 |
Renal replacement therapy | 202 (11.72) | 81 (10.28) | 121 (12.93) | 0.15 |
Norepinephrine | 1111 (64.44) | 409 (51.90) | 702 (75.00) | <0.001 |
Scoring systems | ||||
SOFA | 9.00 (6.00–12.00) | 8.00 (5.00–12.00) | 11.00 (8.00–13.00) | <0.001 |
APSII | 70.00 (48.00–94.00) | 72.00 (52.00–95.00) | 69.00 (48.00–92.00) | 0.03 |
ICU stay, d | 3.52 (1.53–7.68) | 4.64 (2.45–9.17) | 2.61 (0.94–5.88) | <0.001 |
Hospital stay, d | 9.03 (3.52–20.43) | 14.78 (8.31–27.26) | 4.79 (1.41–11.80) | <0.001 |
Characteristics | Total (n = 1724) | Training dataset (n = 1207) | Test dataset (n = 517) | P value |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
SI conversion factors: see Table 1
Abbreviations: see Table 1 | ||||
Age, y, mean (SD) | 66.36 (16.28) | 66.51 (16.04) | 66.04 (16.69) | 0.49 |
Male sex | 1055 (61.19) | 760 (62.97) | 295 (57.06) | 0.27 |
SBP, mm Hg, mean (SD) | 112.36 (17.08) | 112.72 (17.16) | 111.53 (16.89) | 0.19 |
DBP, mm Hg, mean (SD) | 61.78 (11.86) | 61.84 (12.03) | 61.64 (11.46) | 0.74 |
MBP, mm Hg, mean (SD) | 76.44 (11.87) | 76.68 (11.91) | 75.89 (11.77) | 0.21 |
Heart rate, bpm, mean (SD) | 86.25 (18.66) | 86.77 (18.37) | 87.25 (19.24) | 0.06 |
Respiratory rate, bpm, mean (SD) | 21.15 (4.54) | 21.06 (4.46) | 21.36 (4.71) | 0.21 |
Temperature, °C, mean (SD) | 36.48 (1.07) | 36.49 (1.04) | 36.27 (1.13) | 0.52 |
SPO2, %, mean (SD) | 96.16 (5.87) | 96.24 (5.72) | 94.95 (6.19) | 0.39 |
Comorbidities | ||||
Diabetes | 638 (37.01) | 436 (36.12) | 202 (39.07) | 0.46 |
Hypertension | 620 (35.96) | 429 (35.54) | 191 (36.94) | 0.74 |
Myocardial infarction | 503 (29.18) | 369 (30.57) | 134 (25.92) | 0.16 |
Congestive heart failure | 733 (42.52) | 528 (43.74) | 205 (39.65) | 0.34 |
Chronic pulmonary disease | 463 (26.86) | 317 (26.26) | 146 (28.24) | 0.56 |
Malignancy | 215 (12.47) | 147 (12.18) | 68 (13.15) | 0.68 |
Laboratory parameters | ||||
Anion gap, mEq/l | 16.50 (14.00–20.25) | 16.50 (14.00–20.25) | 17.0 (14.0–20.5) | 0.27 |
BUN, mg/dl | 26.5 (18.0–41.5) | 26.5 (18.0–41.5) | 24.5 (16.5–43.5) | 0.98 |
Bicarbonate, mmol/l | 21.0 (17.5–24.5) | 21.0 (17.5–24.5) | 20.5 (17.0–24.0) | 0.07 |
Creatinine, mg/dl | 1.40 (0.95–2.275) | 1.40 (0.95–2.275) | 1.40 (0.90–2.20) | 0.31 |
Chloride, mmol/l | 104.0 (99.5–108.0) | 104.0 (99.5–108.0) | 105.0 (99.5–108.5) | 0.55 |
Glucose, mg/dl | 165.00 (131.50–220.25) | 165.00 (131.50–220.25) | 161.0 (125.0–224.5) | 0.98 |
Hematocrit, % | 32.97 (7.08) | 33.03 (7.13) | 32.83 (6.97) | 0.59 |
Hemoglobin, g/dl | 10.69 (2.42) | 10.71 (2.45) | 10.64 (2.36) | 0.59 |
WBC, 109/l | 13.05 (9.40–17.78) | 13.05 (9.40–17.78) | 13.0 (9.5–17.4) | 0.77 |
Platelets, 109/l | 193.00 (138.25–264.75) | 193.00 (138.25–264.75) | 184.5 (133.5–246.0) | 0.08 |
pH | 7.32 (7.24–7.38) | 7.32 (7.24–7.38) | 7.31 (7.22–7.37) | 0.09 |
Lactate, mmol/l | 3.10 (1.85–5.30) | 3.10 (1.85–5.30) | 3.30 (1.85–5.60) | 0.11 |
Potassium, mmol/l | 4.3 (3.9–4.8) | 4.3 (3.9–4.8) | 4.30 (3.95–4.85) | 0.97 |
INR | 1.4 (1.2–1.8) | 1.4 (1.2–1.8) | 1.35 (1.20–1.80) | 0.25 |
Sodium, mmol/l | 139 (136–142) | 139 (136–142) | 139 (136–142) | 0.7 |
Renal replacement therapy | 202 (11.72) | 137 (11.35) | 65 (12.57) | 0.58 |
Norepinephrine | 1111 (64.44) | 782 (64.79) | 329 (63.64) | 0.86 |
Scoring systems | ||||
SOFA | 9 (6–12) | 9 (6–12) | 10 (6–13) | 0.34 |
APSII | 70 (48–94) | 70 (48–94) | 70 (52–93) | 0.92 |
Predictors of in‑hospital mortality
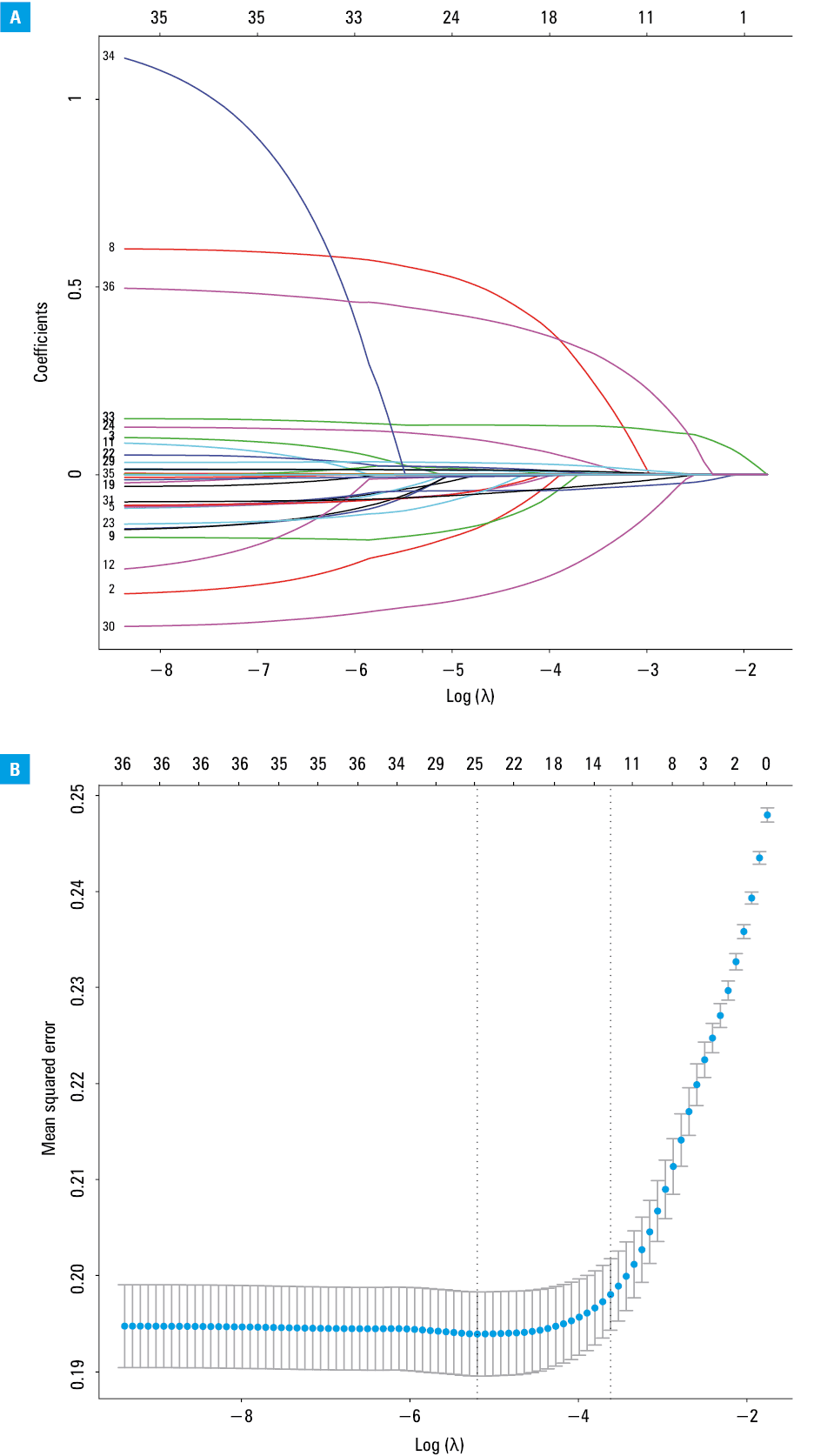
The LASSO logistic regression, which is useful for the preliminary selection of predictors, shrinks the coefficients of less important variables to 0. It selected 14 predictors with large regression coefficients, including age, sex, malignant cancer, bicarbonate, BUN, sodium, heart rate, respiratory rate, temperature, SPO2, MBP, norepinephrine prescription, INR, and lactate, as shown in Figure 1A and 1B. Multivariable logistic regression analysis demonstrated that 11 factors were independently associated with in‑hospital mortality in the post‑CA patients. These were age (OR, 1.33; 95% CI, 1.09–1.61), malignancy (OR, 1.76; 95% CI, 1.16–2.66), bicarbonate (OR, 0.74; 95% CI, 0.60–0.92), BUN (OR, 1.35; 95% CI, 1.17–1.56), sodium (OR, 1.22; 95% CI, 1.04–1.42), heart rate (OR, 1.62; 95% CI, 1.32–2.00), respiratory rate (OR, 1.34; 95% CI, 1.09–1.66), temperature (OR, 0.80; 95% CI, 0.73–0.88), SPO2 (OR, 0.78; 95% CI, 0.67–0.92), norepinephrine prescription (OR, 1.63; 95% CI, 1.23–2.16), and lactate (OR, 1.87; 95% CI, 1.49–2.35) (Table 3).
Variable | LASSO logistic regression | Multivariable logistic regression | ||
OR (95% CI) | P value | OR (95% CI) | P value | |
Age, y | 1.25 (1.03–1.53) | 0.03 | 1.33 (1.09–1.61) | <0.001 |
Male sex | 0.79 (0.60–1.04) | 0.09 | – | – |
Malignancy | 1.77 (1.17–2.70) | 0.007 | 1.76 (1.16–2.66) | 0.008 |
Bicarbonate, mmol/l | 0.75 (0.60–0.93) | 0.008 | 0.74 (0.60–0.92) | 0.007 |
BUN, mg/dl | 1.35 (1.16–1.56) | <0.001 | 1.35 (1.17–1.56) | <0.001 |
Sodium, mmol/l | 1.22 (1.04–1.43) | 0.01 | 1.22 (1.04–1.42) | 0.01 |
Heart rate, bpm | 1.59 (1.29–1.96) | <0.001 | 1.62 (1.32–2.00) | <0.001 |
Respiratory rate, bpm | 1.36 (1.10–1.68) | 0.004 | 1.34 (1.09–1.66) | 0.006 |
Temperature, °C | 0.79 (0.72–0.87) | <0.001 | 0.80 (0.73–0.88) | <0.001 |
SPO2, % | 0.79 (0.67–0.93) | 0.004 | 0.78 (0.67–0.92) | 0.003 |
MBP, mm Hg | 0.87 (0.73–1.04) | 0.12 | – | – |
Norepinephrine | 1.60 (1.20–2.12) | 0.001 | 1.63 (1.23–2.16) | <0.001 |
INR | 1.03 (0.95–1.13) | 0.43 | – | – |
Lactate, mmol/l | 1.81 (1.43–2.29) | <0.001 | 1.87 (1.49–2.35) | <0.001 |
Nomogram of in‑hospital mortality
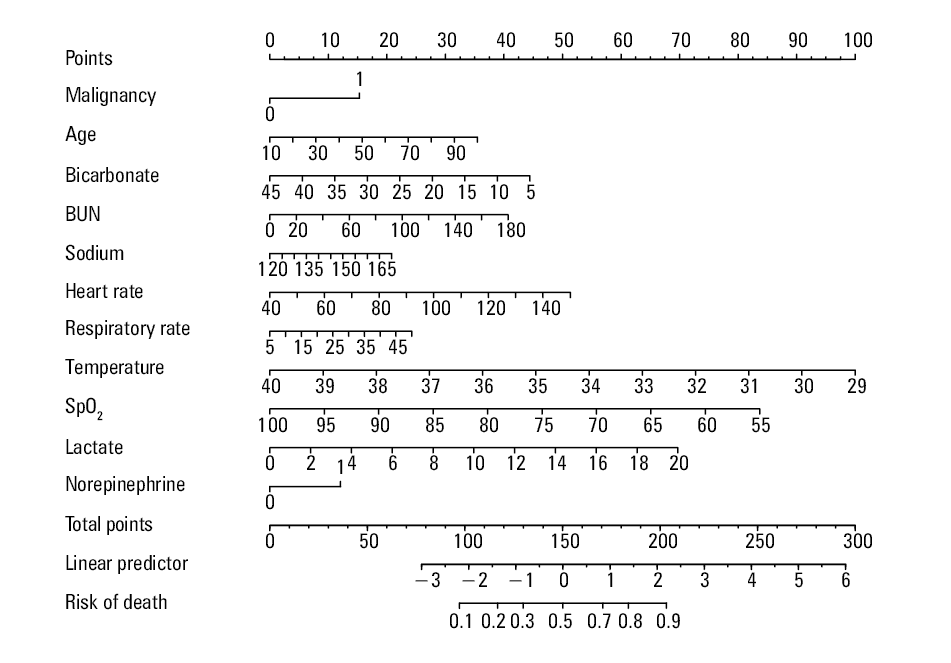
A nomogram was constructed to estimate in‑hospital death in the post‑CA patients. This nomogram contained 11 independent predictors: age, malignancy, bicarbonate, BUN, sodium, heart rate, respiratory rate, temperature, SPO2, norepinephrine use, and lactate (Figure 2). For example, a 70 year old (risk factor score [RFS], 23 points) patient with malignancy (RFS, 15 points) experienced cardiac arrest. His clinical data on admission were as follows: bicarbonate 20 mmol/l (RFS, 27.5 points), BUN 40 mg/dl (RFS, 9 points), sodium 135 mmol/l (RFS, 6 points), heart rate 100 bpm (RFS, 27.5 points), respiratory rate 25 bpm (RFS, 10 points), temperature 37 °C (RFS, 27.5 points), SPO2 95% (RFS, 9 points), lactate 4 mmol/l (RFS, 13 points), and norepinephrine treatment (RFS, 12 points). His total score was approximately 179.5 points, and the risk of in‑hospital mortality was 78%.
Evaluation and validation of the nomogram
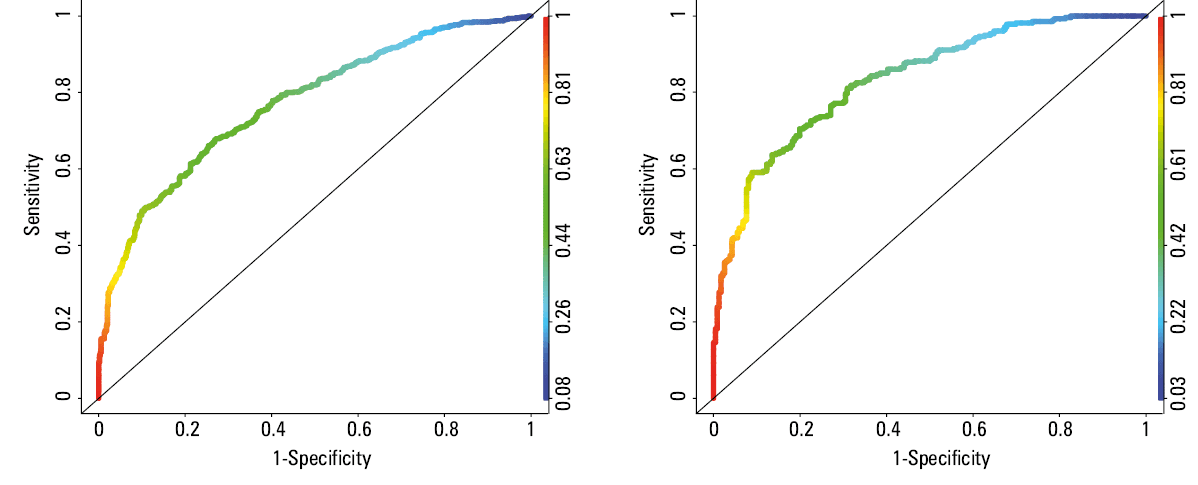
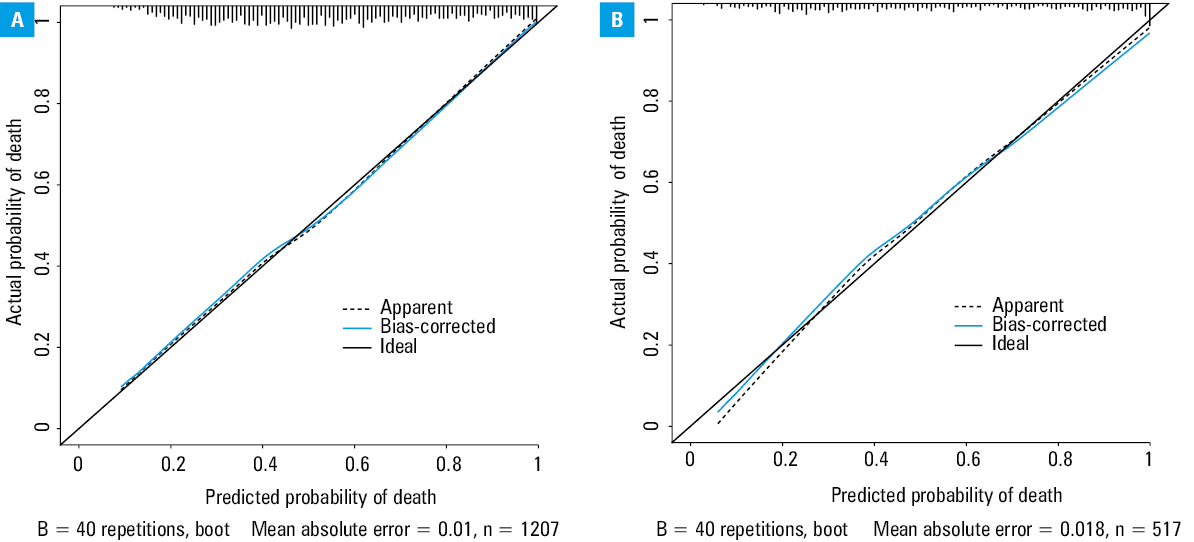
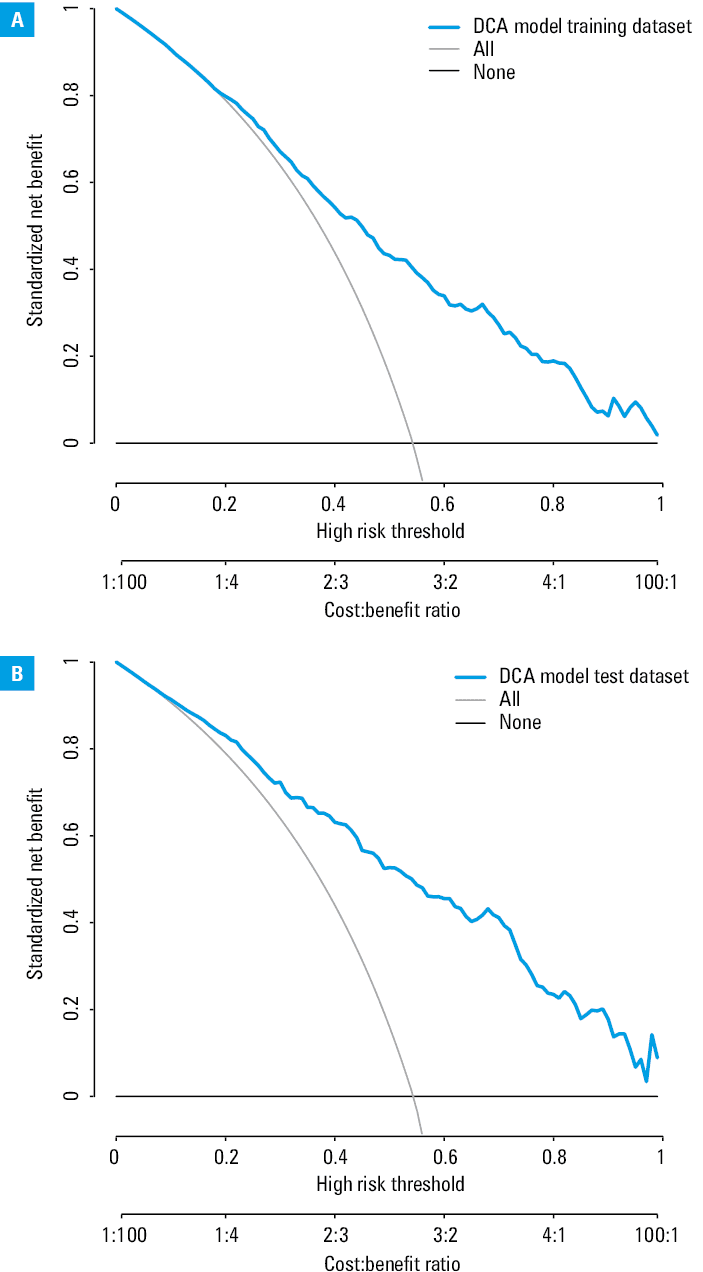
The nomogram had a good discriminating ability in the training set (AUC = 0.787; 95% CI, 0.753–0.821) and test set (AUC = 0.801; 95% CI, 0.778–0.824) (Figure 3A and 3B). On the calibration plots, death rates predicted by the model were close to the observed death rates (Figure 4A and 4B). DCA demonstrated that this nomogram has good clinical utility (Figure 5A and 5B).
Discussion
We included 1724 post‑CA patients from a large intensive care medical database. The in‑hospital mortality incidence in the post‑CA patients was 54.3%. This study showed that age, malignancy, bicarbonate, BUN, sodium, heart rate, respiratory rate, temperature, SPO2, norepinephrine use, and lactate levels were useful in predicting the risk of in‑hospital death in the post‑CA patients. Furthermore, a nomogram was established to evaluate individual in‑hospital death risk. This nomogram was shown to provide excellent guidelines and clinical benefits.
CA is a dangerous and life‑threatening condition. A large number of studies have investigated the factors that contribute to poor clinical outcomes in the post‑CA patients during hospitalization. Previous clinical risk models of CA focused on the on‑admission information of CA rather than the post‑admission clinical information.11-13 These approaches also neglected the importance of vital signs, laboratory tests, and clinical comprehensive scores for in‑hospital death. We believe these data are likely to be much more related to in‑hospital death in the post‑CA patients. Therefore, this study focused on the first clinical data recorded after the patient admission, including comorbidities, vital signs, blood test results, and treatment modalities. This is the first paper to report on the use of hospitalization clinical data, other than the onset information, to predict in‑hospital death in the post‑CA patients.
This study showed that malignancy was an independent risk factor for in‑hospital death. However, this finding is still controversial in light of the results of previous studies. An earlier study18 found that cancer was not associated with mortality in the short or long term after successful resuscitation in CA patients. In contrast, a study on the National Inpatient Sample from the United States reported that in‑hospital CA patients with cancer had poorer survival rates during hospitalization.19 We suspected that the patients with advanced malignancy were more likely to suffer from CA. Their odds of surviving CA are low due to their poor physical condition or multiple organ failure. Issa et al20 found that lactate level and vasopressors administration predicted in‑hospital death in post‑CA patients. Our study supports this conclusion. Lactate level (OR, 1.87; 95% CI, 1.49–2.35) and norepinephrine treatment (OR, 1.63; 95% CI, 1.23–2.16) positively correlated with in‑hospital death. We found no association between sex and in‑hospital mortality in the post‑CA patients. Two previous studies reported that women were at a greater risk of in‑hospital death than men after CA.21,22 A meta‑analysis23 demonstrated that women had lower chances of survival from hospital admission to discharge (OR, 0.59; 95% CI, 0.48–0.73). However, Winther‑Jensen et al24 proposed that female sex was not related to higher mortality in the patients successfully resuscitated from OHCA. Another meta‑analysis demonstrated that women had an increased (OR, 1.10; 95% CI, 1.03–1.20; P = 0.006, I2 = 61%) survival rate after CA.25 These studies have yielded conflicting results on the relationship between sex and clinical outcomes in post‑CA patients. This discrepancy deserves further studies.
Our study is the second to establish a nomogram to predict in‑hospital mortality in the post‑CA patients. Bae et al26 established a nomogram based on data from 982 CA patients, and selected 12 predictors to develop the scoring system applied to adult nontraumatic CA patients. The condition of post‑CA patients is extremely complex and may vary considerably. There is a significant proportion of patients suffering from post‑CA syndrome. Therefore, current standards advocate that clinicians should assess the prognosis after spontaneous return of circulation within 72 hours in coma patients.27 Clinical information collected at admission of the post‑CA patients could be highly useful for the prediction of in‑hospital mortality. Early prediction of in‑hospital mortality is an important tool for clinicians to discuss decision‑making with the patient’s family. Our risk model can individually score post‑CA patients and guide the risk stratification. According to the model, clinicians can identify the patients at a high risk of in‑hospital death and decide on the treatment to improve its medical efficiency. In addition, clinicians can use this nomogram to continuously evaluate the prognosis of comatose patients after spontaneous return of circulation within 72 hours based on the clinical observation indicators (vital signs and laboratory test results).
Study limitations
There are several limitations of this study. Firstly, the study included only adult patients who were resuscitated at the site of CA and could be transported to the hospital or those who experienced CA in the hospital. Additionally, the CA patients during pregnancy or postpartum were excluded. Therefore, the nomogram does not apply to all patients with CA. Secondly, we only included the clinical data collected within 24 hours after admission and did not consider the data collected at the CA onset (the time from CA onset to beginning of the resuscitation) or prehospital care (chest compressions, administration of adrenaline, or defibrillation). Thirdly, our study did not further analyze the mechanisms of CA, such as ventricular fibrillation, asystole, acute pulmonary thromboembolism, and other conditions. It is necessary to conduct a subgroup analysis of specific mechanism of CA in future studies. Finally, the CA patients in our analysis included both OHCA and IHCA. The IHCA patients are usually sicker and have a higher burden of comorbidities than the OHCA patients at the baseline level. This may have impacted our findings.
Conclusions
We established a nomogram based on the admission data in post‑CA patients. This risk model could provide valuable insights into subsequent medical decisions.
- Holmberg MJ, Ross CE, Fitzmaurice GM, et al. Annual incidence of adult and pediatric in‑hospital cardiac arrest in the United States. Circ Cardiovasc Qual Outcomes. 2019; 12: e005580.
- Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014; 129: e28‑292.
- Ravindran R, Kwok CS, Wong CW, et al. Cardiac arrest and related mortality in emergency departments in the United States: analysis of the nationwide emergency department sample. Resuscitation. 2020; 157: 166‑173. | Crossref
- Girotra S, Chan PS, Bradley SM. Post‑resuscitation care following out‑of‑hospital and in‑hospital cardiac arrest. Heart. 2015; 101: 1943‑1949. | Crossref
- Bai ZH, Guo XQ, Dong R, et al. A nomogram to predict the 28‑day mortality of critically ill patients with acute kidney injury and treated with continuous renal replacement therapy. Am J Med Sci. 2021; 361: 607‑615. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION