Association between inherited thrombophilia and venous thromboembolism in patients with non-O blood type: a meta-analysis
Key words: ABO group, factor V Leiden, G20210A prothrombin mutation, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Association between inherited thrombophilia and venous thromboembolism in patients with non-O blood type: a meta-analysis
Introduction: Hereditary conditions, including non‑O blood group or thrombophilic alterations such as factor V Leiden (FVL) and G20210A prothrombin mutation (G20210A PTM), are usually considered risk factors for venous thromboembolism (VTE).
Objectives: This meta‑analysis was carried out to find out if simultaneous occurrence of FVL or PTM and the non‑O blood group may increase the risk of developing VTE.
Patients and methods: MEDLINE and EMBASE databases were explored until March 2021. Eleven publications, comprising 82 465 patients, and 6 studies, including 70 004 patients, were analyzed to evaluate the association between FVL/non‑O group and PTM/non‑O group, respectively. Pooled odds ratios (OR) and 95% CIs were obtained by a random‑effects model.
Results: Nearly 6% of the enrolled patients manifested both FVL and the non‑O group, whereas only 1.4% had PTM and the non‑O group. The VTE risk was considerably amplified in FVL and the non‑O group (OR, 5.94; 95% CI, 5.33–6.61; P <0.01), more than if just 1 of these 2 risk factors was present. The equivalent population attributable risk (PAR) of VTE was around 21%. The patients with PTM and the non‑O group manifested a significantly augmented risk of VTE (OR, 4.01; 95% CI, 3.00–5.36; P = 0.01), although PAR was considerably lower (3.7%).
Conclusions: The co‑occurrence of FVL and the non‑O group enhances the risk of VTE that could have clinical influence and drive therapeutic corrections. The coexistence of PTM and the non‑O blood group seems to play a less important role in the incidence of VTE.
What's new?
The risk of venous thromboembolism determined by the presence of a single inherited thrombophilic alteration, such as factor V Leiden or prothrombin mutation, is difficult to estimate. Nevertheless, the coexistence of these disorders with a blood group other than O considerably increases the risk of venous thromboembolism in the general population. Since the analysis of the blood group can be easily performed, in all patients with other risk factors for venous thromboembolism particular attention should be given to those with the blood groups other than O.
Introduction
Factor V Leiden mutation (FVL) and G20210A prothrombin mutation (G20210A PTM) are the most prevalent genetic causes of thrombophilia.1 Numerous case‑control, cohort studies and meta‑analyses have established that these 2 mutations are associated with an increased risk of venous thromboembolism (VTE), especially in the patients with homozygosity or double heterozygosity.2,3 Indeed, combined hereditary thrombophilias, homozygous FVL or G20210A PTM, antithrombin deficiency, antiphospholipid syndrome, homozygous deficiency of protein C, and homozygous deficiency of protein S are generally considered strong risk factors for VTE.4,5 In a recent meta‑analysis,6 FVL was associated with an increased risk of VTE in both heterozygotes and homozygotes (odds ratio [OR], 4.38; 95% CI, 3.48–5.51 and OR, 11.45; 95% CI, 6.79–19.29, respectively). The OR for G20210A PTM was 2.80 (95% CI, 2.25–3.48) for heterozygotes and 6.74 (95% CI, 2.19–20.72) for homozygotes. The presence of combined heterozygosis is a rare condition, generally considered to be associated with a 10- to 20‑fold increase of VTE risk;4 however, in this analysis, its presence did not appear to confer an additional risk for the first VTE beyond the sole presence of FVL (OR, 3.42; CI 95%, 1.65–7.13).6
On the other hand, the ABO blood group also has a great impact on hemostasis, as it has significant quantitative and qualitative effects on many aspects of the von Willebrand factor (VWF) biology.7-9 Specifically, VWF and Factor VIII levels are greater in individuals with blood groups different than O.10 Furthermore, in individuals with the blood group O, VWF is more vulnerable to proteolysis by disintegrin and metalloproteinase ADAMTS 13. In addition, recent evidence suggested that the ABO group significantly affects platelet plug formation at sites of vascular injury (primary hemostasis).10
Numerous studies and 2 current meta‑analyses have evaluated the connection between the ABO blood group and both venous and arterial thrombosis.11,12 Specifically, the rate of the non‑O blood group was notably higher in individuals with VTE than in controls with an ensuing pooled OR above 2.0.12
Contrastingly, the prevalence and the burden of FVL and G20210A PTM in individuals with different ABO groups have only been assessed in small studies with conflicting results.
Therefore, the objectives of this meta‑analysis were to most reliably assess the presence of both of these hereditary thrombophilic disorders in individuals with the non‑O blood group and to evaluate the potential association between these different prothrombotic alterations and the non‑O group.
Methods
A prospectively developed protocol detailed specific objectives, criteria for the study selection, approaches to assessing the study quality, outcomes, and statistical methods.
Study identification
Attempts were made to identify all published studies that evaluated the association of the 2 most common inherited thrombophilic abnormalities (FVL and G20210A PTM) and the ABO group using the MEDLINE (1994 to March 2021, week 2) and EMBASE (1994 to March 2021, week 2) electronic databases. Articles published before 1994 were excluded, since the role of activated protein C resistance / FVL was established that year. The search strategy was carried out without any language restriction, and the keywords and subject headings used are listed in Table 1.
Database (from 1994 to week 2 of March 2021) | |
Abbreviations: mp, multipurpose | |
Embase | (‘blood group abo system’/exp OR ‘blood group abo system’ OR ‘blood group antigen’/exp) AND (‘blood clotting factor 5 leiden’/exp OR ‘blood clotting factor 5 leiden’ OR ‘prothrombin’/exp) |
Medline | 1 ABO Blood‑Group System/ (15 141)
2 Factor V.mp. (9507)
3 Prothrombin/ (10 753)
4 Factor V/ (6600)
5 Thrombophilia/ (6752)
6 2 or 3 or 4 or 5 (22 849)
7 1 and 6 (70) |
Our research was supplemented by manually reviewing abstract books from the Congress of the International Society on Thrombosis and Haemostasis (ISTH) and reference lists of all retrieved articles. In addition, recent issues of the journals dedicated to thrombosis and hemostasis were manually searched, and content experts for additional published or unpublished trials were contacted.
Study selection
Study selection was independently performed by 2 reviewers (MN and LS). When necessary, disagreements were resolved via discussion and the opinion of a third reviewer (FP) was sourced. The included studies met the following criteria: 1) the study population was of ABO type; 2) separate data for patients with or without VTE were available; 3) data defining the blood groups as either A, B, AB and O, group O and non‑O were extractable; and 4) FVL and / or G20210A PTM were assessed in patients and in controls.
Case reports, case series of patients, reviews, and nonhuman studies were excluded. It was decided that if multiple papers concerning a single study were available, only the most recent publication would be used, and if necessary, it would be then supplemented with data from earlier publications. To assess the agreement between the reviewers on the study selection, we used the κ statistic that measures the agreement beyond chance.13
Data extraction and study validity assessment
Data extraction
The following data were extracted by 2 reviewers (MN and LS): 1) study characteristics (year of publication, design, study center); 2) patient and control characteristics (number of individuals studied, mean age, variation in age, sex, and race); 3) prevalence of ABO genotypes in VTE patients and in controls; 4) prevalence of FVL and / or G20210A PTM in VTE patients and in controls.
Any disagreements were resolved by consensus based on the opinion of the third reviewer (FP), if necessary. If the required data could not be located in the published report, the corresponding author was contacted by email.
Study validity assessment
The assessment of the study validity was independently carried out by 2 unmasked investigators (MN, LS). As the use of quality scoring systems in observational studies is controversial,14 it was decided to assess the study quality with the Newcastle–Ottawa Scale.15 The studies were conferred a maximum of 4 stars for selection, 1 star for comparability, and 3 stars for outcome assessment, with more stars indicating better quality. The maximum possible score was 8. For the purpose of the current review, the studies that received at least 7 stars were considered of high quality (Table 2).
Study, year | Type of study (origin) | Thrombophilic factors evaluated | Study sample, n | Cases, n (hetero- / homozygous) | Cases, description | Median age cases, y | Controls, n (hetero-/homozygous) | Controls, description | Median age control, y | Aim |
Abbreviations: ARIC, Atherosclerosis Risk in Communities; AT III, antithrombin III; BMI, body mass index; CHS, Cardiovascular Health Study; DVT, deep venous thrombosis; F, factor; FVL, factor V Leiden; ICD, International Classification of Diseases; MTHFR, methylene tetrahydrofolate reductase; PE, pulmonary embolism; PTM, prothrombin G20210A mutation; VTE, venous thromboembolism; VWF, von Willebrand factor | ||||||||||
Morelli,24 2004 | Case‑control (Dutch) | ABO group, FVL, FVIII, VWF | 942 | 471 | Patients <70 y with first, objectively confirmed DVT | 46 | 471 | Healthy volunteers with the same sex, age, no biologic relationship, no history of venous thromboembolism, no use of coumarin‑derivatives for at least 3 months and no known malignant disorders | 46 | To study the effect of ABO genotype on thrombosis risk in a large population‑based, case‑control study of venous thrombosis (Leiden Thrombophilia Study [LETS]) |
Ohira,23 2006 | Nested case‑control (North American) | ABO group, FVL, PTM (homozygous and heterozygous) | 1500 | 492 (FVL: not specified, PTM: 16/0) | Patients with objectively confirmed DVT or PE | 62.6 | 1008 (FVL: not specified, PTM: 20/0) | Two controls per case matched for age (5‑year groupings), sex, race (African Americans, white), follow‑up time (event date within 2 years of controls assigned date), and study (ARIC, CHS) | 62.5 | To examine the association between ABO blood type and incident VTE while investigating potential effect modifiers of the association in a large sample of African American and white people |
Jukic,26 2009 | Case‑control (Croatian) | ABO group, FVL, PTM (heterozygous), MTHFR mutation | 329 | 129 (FVL: 29/0, PTM: 6/0) | Patients with objectively confirmed DVT or PE | 46 | 200 (FVL: 7/0, PTM: 7/0) | Asymptomatic and healthy blood donors | 40 | To assess the association between ABO blood group genotype and genetic risk factors for thrombosis (FVL, PTM, and MTHFR reductase C677T mutations) in the Croatian population and to determine whether genetic predisposition to thrombosis risk is higher in non‑O blood group genotypes than in O blood group genotypes |
Lima,25 2009 | Case‑control (Brazilian) | ABO blood group, FVL | 116 | 65 | Patients with objectively confirmed DVT | 34 | 51 | Age- and sex‑matched individuals with no history of thrombosis | – | To investigate the relationship between DVT and the association of AB genotypes and FVL in the population of the state of Pernambuco in Brazil |
Sode,21 2013 | Cohort (Danish) | ABO blood group, FVL, PTM (heterozygous and homozygous) | 66 001 | 4558 (FVL: 359/28, PTM: 65/2) | Patients with ICD code for VTE at the discharge | 60 | – | – | – | To test the hypothesis that ABO blood type alone and in combination with mutations in FVL and PTM is associated with the risk of VTE and myocardial infarction in the general population |
Spiezia,20 2013 | Case‑control (Italian) | ABO group, AT III, protein C and protein S deficiencies, FVL, PTM | 1424 | 712 | Patients with first, objectively confirmed proximal DVT (with or without PE) | 58.2 | 712 | Healthy volunteers, referred in the same study period to the blood bank, matched for age (SD, 3 years) and sex | 58 | To confirm the association of non‑O blood groups with DVT, to assess its strength, and to investigate the impact of thrombophilia on this association |
Canonico,29 2007 | Case‑control (French) | ABO group, FVL, PTM (heterozygous and homozygous) | 881 | 271 (FVL: not specified, PTM: 20/0) | Postmenopausal women between 45–70 y with first objectively confirmed idiopathic VTE | 61.6 | 610 (FVL: not specified, PTM: 11/0) | Age- and sex‑matched healthy individuals with no history of thrombosis | 61.5 | To investigate the association of VTE with ABO blood type and the potential effect modifiers for this association among postmenopausal women |
Ribeiro,22 2016 | Population‑based case‑control (Dutch) | ABO group, FVL, obesity | 11 253 | 4956 | Patients with objectively confirmed DVT or PE | 49 | 6297 | Age- and sex‑matched healthy individuals with no history of thrombosis | 48.1 | To investigate whether FVL with the non‑O blood group modifies VTE risk in individuals with different BMI |
Mohammed,28 2020 | Case‑control (Iraqi) | ABO group, FVL, PTM | 100 | 50 | Patients with first, objectively confirmed VTE | 34 | 50 | Healthy, age‑matched, unrelated volunteers from the same region, referred to in the same study period | 37 | To investigate the association and risk of having different ABO blood groups along with 3 thrombophilia mutations, as well as 3 thrombophilia markers in a group of patients with unstimulated thrombosis in comparison with healthy subjects |
Tregouet,19 2009 | Case‑control (French) | ABO group, FVL (heterozygous) | 1951 | 1150 (395/0) | Patients with objectively confirmed VTE | – | 801 (180/0) | 475 healthy French white patients without a personal history of cardiovascular disease (including VTE) and 326 healthy French white heterozygotes for the FVL or FII 20210A mutations | – | To investigate whether the effect of the ABO blood groups could be modulated by FVL and PTM mutations |
Hiltunen,27 2006 | Nationwide, population‑based, nested case‑control (Finnish) | Pregnancy, ABO group, FVL (heterozygous and homozygous) | 711 | 70 (6/1) | Women with ICD code for VTE during pregnancy or puerperium | 31.3 | 641 (14/0) | Women without complications sampled randomly (every 46th pregnancy) | 28.8 | To assess the risk for pregnancy‑associated VTE of FVL, PTM, FV A4070G, MTHFR C677T, TFPI C536T, PROC T38853G, FXIII V34L, blood group, age, and BMI, and their interactions and public health impact |
Statistical analysis
The pooled OR of the associations between different blood groups and genotypes and VTE was calculated using the Review Manager (RevMan, version 5.3.3 for Windows, Oxford, England; The Cochrane Collaboration, 2014). ORs and 95% CIs were calculated using a random effects model (DerSimonian and Laird method).16 Statistical heterogeneity was evaluated using the I2 statistic, which assesses the appropriateness of pooling the individual study results.17 The I2 value provides an estimate of the amount of variance across studies due to heterogeneity rather than chance. I2 below 30% designates mild heterogeneity, 30% to 60% moderate heterogeneity, and above 60% indicates substantial heterogeneity. When heterogeneity was present, repeated analyses were performed by removing 1 study at a time to assess the source of the heterogeneity. Furthermore, 2 subgroup analyses were planned. In the first one, the studies conducted in non‑Western countries were left out, to specifically explore the role of the thrombophilic abnormalities in the Caucasian patients. In the second one, the studies involving only women were excluded in order to minimize sex disparities.
Finally, the effect of the association of blood group genotypes with the most common inherited thrombophilic abnormalities (FVL and G20210A PTM) on VTE risk was evaluated.
The proportion of VTE in the population that could be attributed to the coexistence of the non‑O blood group and FVL or G20210A PTM (population attributable risk [PAR]) was estimated as follows:
PAR = 100 × [prevalence (OR – 1)/prevalence (OR – 1) + 1]
For this calculation, the fixed effects model was used, and the prevalence of exposure was estimated as the genotype frequency among control patients.
Publication bias
The publication bias was explored using funnel plots of effect size against a standard error.18
Results
Study selection
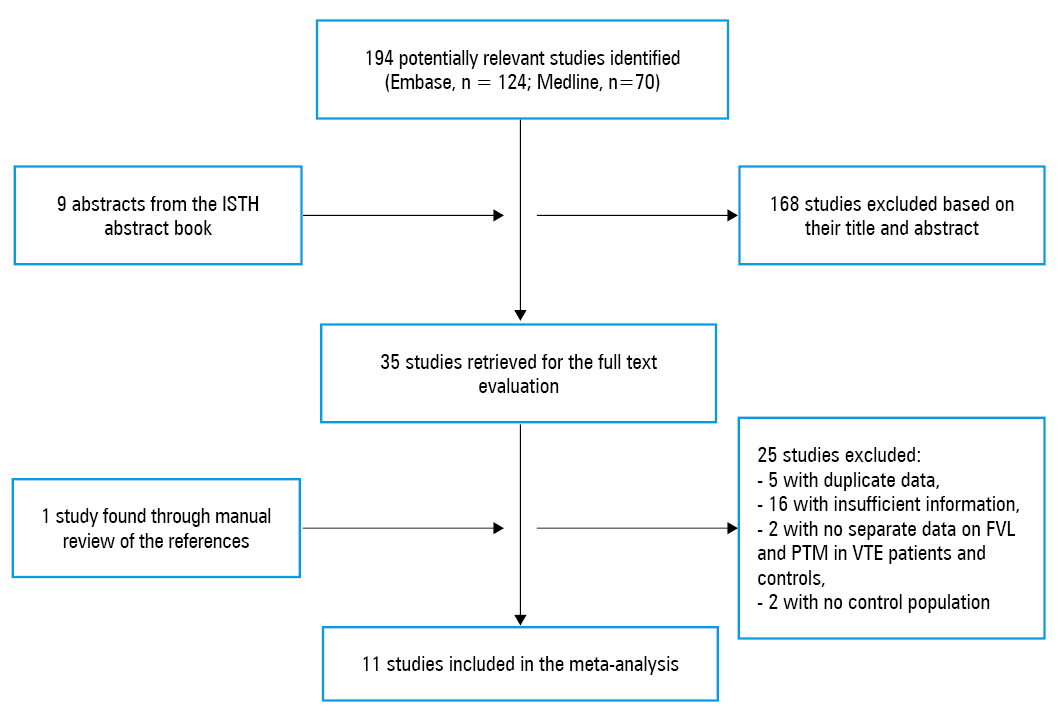
A total of 194 studies were retrieved through our search strategy, including 70 from Medline and 124 from Embase databases (Figure 1). In addition, 9 unpublished articles were detected among ISTH abstracts. As many as 168 studies were discarded after screening the title and abstract using the predefined inclusion and exclusion criteria, leaving 35 studies for a more detailed evaluation. The interobserver agreement for the study selection was excellent, with a κ of 0.91. Furthermore, 1 study was detected by a manual review of the references of selected studies and current reviews. Of the 36 retrieved studies, 25 were thereafter eliminated for the subsequent reasons: 18 did not assess the connection between the ABO blood group and VTE, nor did they provide separate data on the frequency of the blood group in VTE patients and in controls, 2 did not have a control population, 5 did not include original data or were duplicates. Of the 11 selected articles,19-29 3 included data from more than 1 study.19,21,23 Thus, 14 studies reported in 11 publications were contained in our systematic review. Additional data were provided by the authors of 1 publication.19
Abbreviations: ISTH, International Society on Thrombosis and Haemostasis; others, see Table 2
Characteristics of the studies
Baseline characteristics of the analyzed studies are summarized in Table 3. All the papers were written in English; 1 of the 11 publications comprised was a population cohort study21 and 10 were case‑controls.19,20,22-29 A particular study looked at the FVL and G20210A PTM in women with thromboembolism during pregnancy or puerperium,27 whereas another examined the link of VTE with the ABO blood group among postmenopausal women.29 Only 6 studies specified the number of heterozygotes and homozygotes for FVL and G20210A PTM.19,21,23,26,27,29 Double heterozygosis was not reported in the included studies.
Study | Year | Selection | Comparability | Exposure | |||||
*Asterisks are used as stars. | |||||||||
Sode21 | 2013 | * | * | * | * | * | * | * | * |
Jukic26 | 2009 | * | – | * | * | – | * | * | * |
Ohira23 | 2006 | * | * | – | * | * | * | * | * |
Lima25 | 2008 | * | – | – | * | * | * | * | * |
Hiltunen27 | 2006 | * | * | – | * | * | * | * | * |
Morelli24 | 2005 | * | * | * | * | * | * | * | * |
Spiezia20 | 2013 | * | * | * | * | * | * | * | * |
Ribeiro22 | 2016 | * | * | * | * | * | * | * | * |
Tregouet19 | 2009 | * | * | * | * | * | * | * | * |
Canonico29 | 2008 | * | * | – | * | * | * | * | * |
Mohammed28 | 2020 | * | * | * | * | * | * | * | * |
Study quality
The quality of the studies was for the most part high. Quality assessment items are shown in Table 2. Nine of the 11 publications received at least 7 stars on the Newcastle–Ottawa Scale and were categorized as being of high quality, with only a few individuals randomly excluded from either case or control groups. In addition, in 6 out of 10 case‑control publications, the controls were matched with patients for sex and age. All the included studies were published in peer‑reviewed journals.
Association between blood group and inherited thrombophilic abnormalities
Factor V Leiden
Eleven publications totaling 9689 VTE patients and 72 776 controls assessed the connection between blood group and FVL.19-29 Considering the O group without FVL as the reference group, the risk of VTE seemed to be progressively higher in the non‑O blood group–FVL negative individuals (OR, 1.78; 95% CI, 1.69–1.89) and in the O blood group–FVL positive people (OR, 3.03; 95% CI, 2.61–3.52), with a maximum risk in the non‑O blood group–FVL positive patients (OR, 5.94; 95% CI, 5.33–6.61) (Figure 2). Heterogeneity among the studies was considerable (I2 = 81%) and did not drop following progressive removal of the papers. A funnel plot of OR vs standard error was marginally asymmetric with an absence of studies in the bottom left‑hand corner, implying the presence of the publication bias.
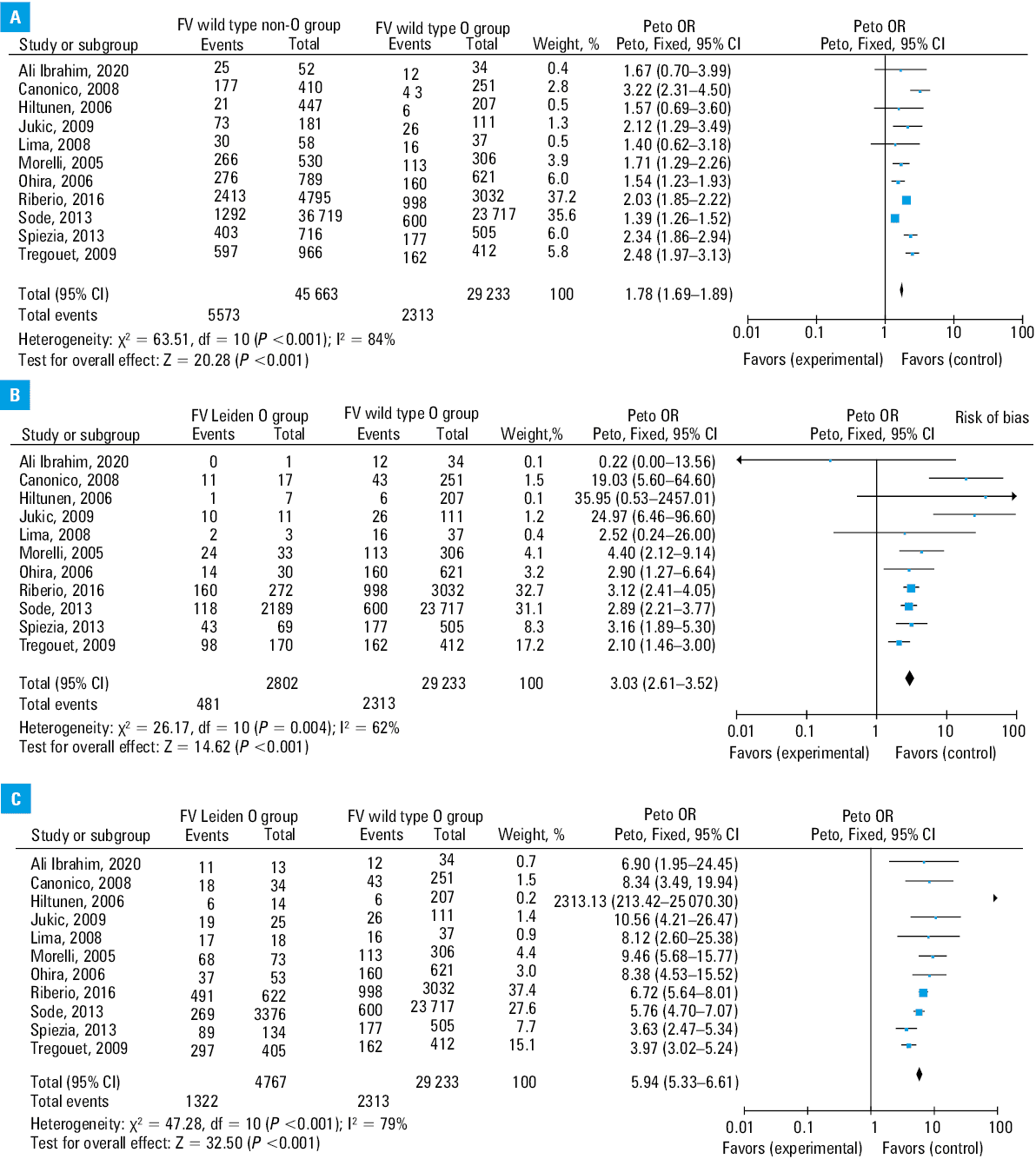
Abbreviations: df, degrees of freedom; OR, odds ratio
The corresponding PAR of VTE was 21% for the non‑O blood group–FVL positive patients.
Mutation G20210A of factor II
Only 6 publications totaling 3849 patients and 70 004 controls provided separate data on the frequency of G20210A PTM in the patients with different blood groups.19,21,23,26,28,29 Considering the O group without G20210A PTM as the reference group, the risk of VTE appeared to continuously increase in the non‑O blood group–PTM negative individuals (OR, 1.54; 95% CI, 1.43–1.66) and in the O blood group–PTM positive individuals (OR, 2.41; 95% CI, 1.67–3.49), with a maximum risk in the non‑O blood group–PTM positive patients (OR, 4.01; 95% CI, 3.00–5.36) (Figure 3). Heterogeneity among the studies was considerable (I2 = 66%) and did not drop following progressive removal of the studies. A funnel plot of OR vs standard error was symmetric, suggesting a lack of publication bias. The corresponding PAR of VTE was 3.7% for the non‑O blood group–PTM positive patients.
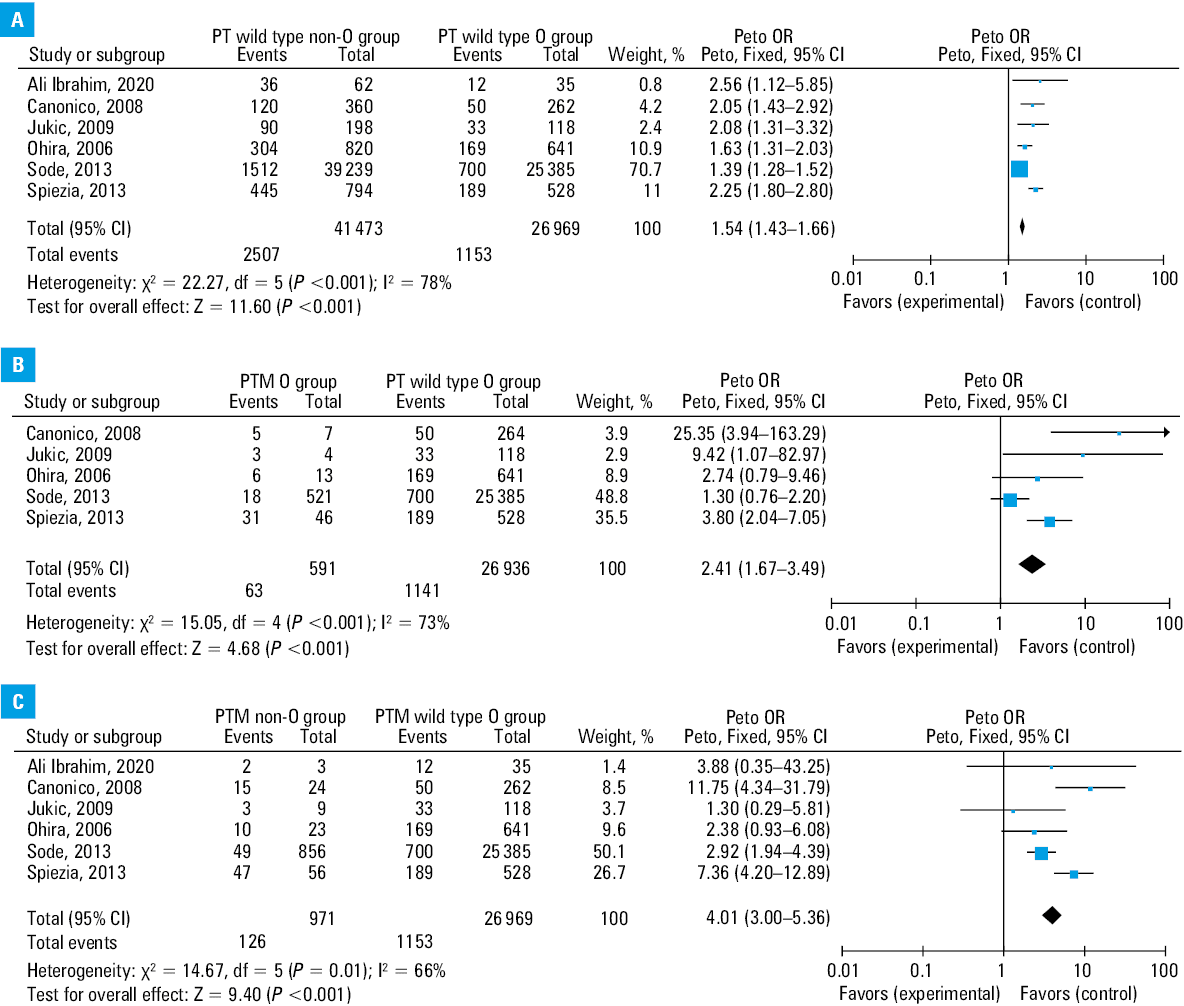
Abbreviations: PT, prothrombin; PTM, prothrombin mutation; others, see Figure 2
Subgroup analyses
Results of subgroup analyses containing only the Western population19-22,24,26-29 yielded similar results (OR, 5.85; 95% CI, 5.25–6.53 for the FVL non‑O blood group vs the FV wild type O group, and OR, 4.24; 95% CI, 3.13–5.75 for the G20210A PTM non‑O group vs the PTM wild type O‑group). The results were analogous also when the studies including only women were excluded from the analysis27,29 (OR, 5.83; 95% CI, 5.23–6.50 for the FVL non‑O blood group vs the FV wild type O group, and OR, 3.63; 95% CI, 2.68–4.92 for the G20210A PTM non‑O group vs PTM wild type O group).
Discussion
This large meta‑analysis, including 11 publications for over 85 000 patients and controls, aimed to assess the connection between FVL or G20210A PTM and the non‑O blood group. Our study results showed that both these thrombophilic conditions are considerably related to an increased risk of VTE in the patients with the non‑O blood group.
The strength of our finding is additionally supported by the results of the subgroup analyses.
One of these subgroups analyzed mostly European studies, excluding 1 study conducted in Latin America25 and 1 including white North Americans, African Americans, and 6 other ethnicities.23
Indeed, several evidences suggest that VTE incidence is the highest in individuals of African ancestry, followed by Caucasians, intermediate in Hispanics, and the lowest in Asians.30 The allele frequency of FVL is approximately 5% in Europe (18% among VTE patients), with a tendency for a north‑south gradient. Its highest prevalence is seen in the Northern Europe and the lowest prevalence (0%–1.5%) in some Southern Slavic countries. The G20210A PTM allele seems to be limited to Caucasians, with an overall prevalence ranging from 0.6% to 4% in healthy people (7% in VTE patients). The mutation is more common in the Southern than Northern Europe, manifesting a gradient opposite to that of FVL.30 On the other hand, the regional distribution of different blood types varies across continents, with the O‑group being more frequent in the Latin Americans, North Americans, Africans, Caribbeans, and Asians, and the A group being more frequent in the Europeans.31,32
In the current analysis, when the ABO blood type and FVL or G20210A PTM genotype were combined, a stepwise increase in the risk of VTE was observed, along with a trend of multiplicative influence for FVL and an additive effect for G20210A PTM. The PAR of VTE was 21% in the non‑O blood group–FVL positive patients and 3.7% for the non‑O blood group–G20210A PTM positive patients. This finding suggests that the non‑O blood group confers an increased likelihood of developing VTE, and this risk is particularly high in FVL individuals, irrespective of the presence of homozygous or heterozygous genotypes and the specific type of the non‑O blood group. Considering the high prevalence of the non‑O blood group and FVL in the general population, the recognition of the coexistence of these abnormalities may have a considerable clinical impact in terms of prophylactic and therapeutic strategies, especially in high‑risk subgroups of patients, and when combined with nongenetic risk prediction scores.33,34
In fact, de Haan et al34 examined the performance of different single nucleotide polymorphism (SNP) tests for the prediction of incident VTE and found out that a parsimonious model comprising the 5 SNPs most strongly associated with VTE and including also ABO, FVL, and G20210A PTM, performed as well as the full 31‑SNP model. The area under the curve (AUC) for a risk model based on known nongenetic risk factors was 0.77 (95% CI, 0.76–0.78).34 Combining the nongenetic and genetic risk models improved the AUC to 0.82 (95% CI, 0.81–0.83).34 More recently, Evensen et al35 performed a population‑based case‑cohort study to estimate the proportion of VTEs that could be attributed to established prothrombotic genotypes. Six SNPs, comprising ABO, FVL, and G20210A PTM, were confirmed as significantly associated with VTE. The cumulative PAR for the 6‑SNP model was 45.3% for total VTE and 61.7% for unprovoked VTE. The PAR of the established prothrombotic genotypes was higher in DVT than in pulmonary embolism, and higher in the young than in the elderly patients.35
Furthermore, the awareness of the presence of the non‑O blood group in mildly thrombophilic patients could be useful for the VTE recurrence risk evaluation.36 Indeed, in the patients with mild thrombophilia, specifically heterozygous forms of G20210A PTM or FVL, the relative risk of recurrent VTE was only slightly elevated at 1.4 (95% CI, 1.0–1.8) and 1.5 (95% CI, 1.1–1.9), respectively.37 Therefore, in the absence of other risk factors, an extended anticoagulation is not warranted based on mild thrombophilia alone.38 Conversely, previous studies have demonstrated that the non‑O blood type is associated with a significant and clinically relevant increased risk of recurrent VTE.39,40 In particular, in a prospective study carried out by Gandara et al39 during 1552 patient‑years, 101 events occurred in 380 non‑O patients (6.5 events per 100 patient‑years; 95% CI, 5.3–7.7), as compared with 14 events in 129 O‑group patients during a follow‑up of 560 patient‑years (2.4 per 100 patient‑years; 95% CI, 1.3–3.7). Similarly, in another study,40 which investigated the role of the ABO blood group in the persistence of residual vein thrombosis (RVO), a multivariate analysis revealed that the non‑O blood group was considerably linked to a greater RVO risk (OR, 3.71), along with active cancer (OR, 5.54), and femoral involvement (OR, 3.35). In contrast, severe thrombophilia did not correlate with RVO (OR, 1.32; 95% CI, 0.56–3.11).
Our meta‑analysis contains some possible limitations. Firstly, the application of formal meta‑analytic methods to observational studies is questionable, because the bias implicit to the study design could distort the strength of associations within the data.14 To reduce this potential bias as much as possible, a decision was made to perform different subgroup analyses to exclude studies enrolling only women or studies involving non‑Caucasian patients. Secondly, studies included in our meta‑analysis had different inclusion and exclusion criteria, and combining results across studies may not be appropriate. In addition, the heterogeneity across the studies, calculated using the I2 statistic, was high, implying caution in the interpretation of the results. Nevertheless, the decision was made to combine the results using the random‑effects model, an approach that considers the variance among the studies. Lastly, as there was no specific research for grey literature, the existence of the publication bias could not be excluded. Since it is recognized that the publication bias can affect the results of meta‑analyses, we attempted to evaluate it using a funnel plot. The funnel plot that took into consideration the G20210A PTM appeared symmetric, which implied a lack of the publication bias. Conversely, in the funnel plot that assessed the FVL, an absence of studies in the bottom left‑hand corner implied that smaller, unpublished studies that showed a reduced risk of VTE in the O blood group patients with FVL were excluded from our meta‑analysis.
Nevertheless, as our results were based on data for more than 85 000 patients and the outcomes were consistent among the studies, insertion of these studies and elimination of the bias, if it indeed existed, is extremely unlikely to have affected our results. In conclusion, the results of our meta‑analysis showed that the simultaneous presence of FVL and the non‑O group is associated with almost 6‑fold increased risk of VTE. Furthermore, the population‑attributable risk of FVL to VTE is not trivial among the non‑O group patients. Therefore, the ABO blood group investigation should be included in all diagnostic workups, as the increased risk of VTE could have clinical effects and may lead to therapeutic adjustments.
The association between the prothrombin mutation and the non‑O blood group seems to play a less important role in the incidence of VTE.
- Rosendaal FR, Reitsma PH. Genetics of venous thrombosis. J Thromb Haemost. 2009; 7: 301‑304. | Crossref
- Rodeghiero F, Tosetto A. Activated protein C resistance and factor V Leiden mutation are independent risk factors for venous thromboembolism. Ann Intern Med. 1999; 130: 643‑650. | Crossref
- Segal JB, Brotman DJ, Necochea AJ, et al. Predictive value of factor V Leiden and prothrombin G20210A in adults with venous thromboembolism and in family members of those with a mutation: a systematic review. JAMA. 2009; 301: 2472‑2485. | Crossref
- Nicolaides A, Fareed J, Kakkar AK, et al. Thrombophilia. Clin Appl Thromb Hemost. 2013; 19: 177‑187. | Crossref
- Bravo‑Pérez C, de la Morena‑Barrio ME, Vicente V, Corral J. Antithrombin deficiency as a still underdiagnosed thrombophilia: a primer for internists. Pol Arch Intern Med. 2020; 130: 868‑877. | Crossref
ARTICLE INFORMATION