Smoking cessation after coronary angiography and percutaneous coronary intervention
Key words: coronary angiography, coronary artery disease, smoking, smoking cessation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Smoking cessation after coronary angiography and percutaneous coronary intervention
Introduction: Smoking is a crucial modifiable risk factor for coronary artery disease. However, effective support in smoking cessation (SC) and data regarding factors related to SC are still inadequate.
Objectives: We aimed to assess SC rates and factors related to effective SC in patients after coronary angiography (CA).
Patients and methods: Patients who underwent CA between 2014 and 2018 at a single center in Poland were screened for active smoking. After at least 6 months after the procedure, the patients were contacted by telephone to obtain information about their current smoking status and history of smoking during the follow‑up.
Results: A total of 3719 consecutive patients were screened. Of these, 921 (24.8%) declared active smoking. At least 6 months after CA, 241 patients were available for a follow‑up interview. The mean (SD) age of the patients was 61.2 (9.3) years, 168 (69.7%) were men, and 115 (47.7%) had acute coronary syndrome. The mean (SD) duration of hospitalization was 6 (4.4) days, and 67 patients (27.8%) were scheduled for a second‑stage procedure. A total of 80 patients (33.2%) declared SC at the 6‑month follow‑up. The multivariable logistic regression analysis indicated that duration of hospitalization equal to or greater than 4 days (odds ratio [OR], 3.62; 95% CI, 1.9–6.89), the Fagerström score equal to or lower than 4 points (OR, 1.96; 95% CI, 1.01–3.79), a scheduled second hospitalization (OR, 2.54; 95% CI, 1.32–4.86), and a smoking load greater than or equal to 51 pack‑years (OR, 2.28; 95% CI, 1.16–4.47) increased the chance of SC.
Conclusions: A substantial number of patients who underwent CA were current smokers, with low SC rates in the follow‑up. A prolonged hospital stay, scheduled second hospitalization, low nicotine dependence but also a high load of pack‑years increased the chances of SC, which underscores the need for intensive and repetitive in‑hospital counseling in the whole population of smokers.
What's new?
Smoking is a major avoidable cause of premature deaths in Poland; however, data on smoking cessation rates, effective support, and factors related to smoking cessation are still inadequate. In a cohort of smoking patients who underwent coronary angiography we found that prolonged hospital stay, along with a scheduled second hospitalization, low nicotine dependence, and a high load of pack‑years are factors related to successful smoking cessation. These findings indicate the need for intensive in‑hospital support and repetitive counseling for smoking cessation in this group of patients.
Introduction
There are approximately 1.1 billion adult smokers and at least 367 million smokeless tobacco users globally. According to the World Health Organization, consumption of tobacco kills up to 50% of its users, resulting in more than 8 million deaths each year. This points to tobacco consumption as the leading cause of preventable diseases and deaths.1
The age‑standardized prevalence of global tobacco smoking has decreased from 26.9% to 20.2% since the beginning of the 21st century, and is projected to decline to 15.5% by 2025.1 Evidence suggests that the majority of current smokers (70%) are self‑motivated or exhibit an intention to stop smoking.2 Another study indicated that approximately 90% of current tobacco users regret having started smoking,3 and a similar percent of interviewees stated that they would intend to quit smoking had the process involved no “suffering.”4 However, these intentions and desires are often counteracted by reality.
Along with the reduction of tobacco consumption, the rate of premature deaths in Poland has decreased significantly in the last decade.5 The role of smoking in the development of atherosclerosis and an increased risk of acute coronary syndrome (ACS) in smokers have been widely documented.6-8 The proportion of smokers among the patients with established coronary artery disease (CAD) has not changed substantially, and equals about 50%. Most of them try to stop smoking following a coronary event.9 Smoking has also been consistently identified in the literature as the primary risk factor for acute myocardial infarction (AMI) in the Polish population.10 A recent study11 confirmed that among the patients with AMI younger than 40 years there is a significantly higher number of current smokers than in those aged 40 years or older (37.5% vs 23%; P <0.001). Smoking cessation (SC) is one of the most effective preventive measures for AMI.12 A meta‑analysis of studies involving patients with AMI with a follow‑up of 2 to 10 years indicated that the individuals who had quit smoking showed an almost 50% reduction in overall mortality (odds ratio [OR], 0.54, 95% CI, 0.46–0.62).13 This indicates that smoking cessation is highly beneficial for a variety of reasons, yet only a fraction of tobacco users actually make an actual effort to quit.
Coronary angiography (CA) is the most important approach for the diagnosis of chronic coronary syndrome (CCS). The procedure may be considered a teachable moment for smokers that may enhance their motivation for a change of habits.14 Moreover, support provided at the right time can encourage SC.14,15 Finally, understanding of the factors related to effective SC after coronary events that led to CA is crucial for modeling SC programs.
The present study aimed to estimate the proportion of patients who declared successful SC after CA performed at a single Polish center, and to identify the determinants of and factors influencing successful SC.
Patients and methods
Study population
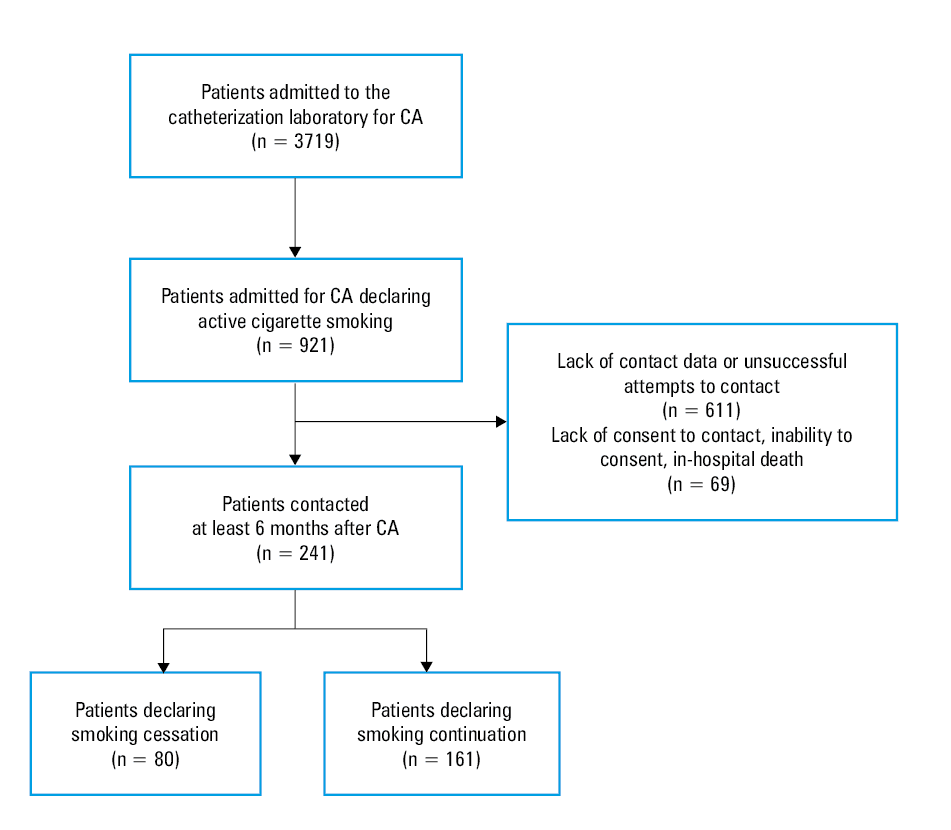
This was a prospective investigation of active smokers scheduled for a diagnostic CA. Out of 3719 patients hospitalized in the Department of Cardiology of the Grochowski Hospital in Warsaw, Poland, between January 2014 and November 2018, who underwent a diagnostic CA due to CCS or ACS, a total of 921 individuals self‑reported active smoking and were prescreened. Of these, 241 were contacted at least 6 months after the procedure and were interviewed by telephone. The remaining 680 individuals were not contacted for reasons listed in Figure 1. The screening was based on a preprocedural questionnaire that required the patients to declare their smoking status. Active smoking was defined as having smoked at least 1 cigarette in the last 30 days and at least 100 cigarettes in the entire life.16 Conversely, nonsmoking was defined as having smoked less than 1 cigarette in the last 30 days and a self‑declaration of nonsmoking.17,18 The patients who declared active smoking were approached during hospitalization, and those aged 18 years or older were invited to participate in this study. Age, sex, medical history, nicotine dependence, and readiness for SC were determined at baseline. The patients were contacted via telephone at least 6 months after CA, and were asked about their current smoking status and the history of smoking during the follow‑up. Information on other possible determinants of SC, such as the level of education, living with a life partner, passive smoking, and participation in a cardiac rehabilitation program was also gathered. The questionnaires were completed by physicians who contacted the patients. Data regarding hospital stay, potential complications, staged procedures, and clinical status were obtained from the medical documentation. A flowchart of the study is shown in Figure 1.
Ethical considerations
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Center of Postgraduate Medical Education (16/PB/2014; 10/PB‑A/2015). All the patients provided their informed consent before enrolment. The study was registered at clinicaltrials.gov as part of a larger project, with a trial identifier NCT040784702.
Nicotine dependence status
The Fagerström and smoking motivation tests were used to assess the nicotine dependence and SC motivation, respectively. The Fagerström test is the most commonly used tool to evaluate nicotine dependence. Scores of 6 points or greater predict a high level of nicotine dependence and indicate the need for a higher level of behavioral support that may be ensured by pharmacological aid.19,20
Interventions and end points
At discharge, all patients were advised to stop smoking and received low‑intensity counseling that focused on the benefits of quitting, especially on the reduced risk of cardiovascular disease. The primary end point was self‑reported SC at the 6‑month follow‑up. The secondary end points were factors that influenced effective SC.
Statistical analysis
Baseline data are presented as mean and SD or median and interquartile range (IQR) for normally or non‑normally distributed continuous variables, respectively, and as frequency for categorical variables. The Shapiro–Wilk test was used to assess the normality of data distribution. Univariable and multivariable logistic regression models were used to identify the covariates associated with higher odds of SC. The following variables were included in the model: age (assigned according to quartiles: 26–54 years, 55–61 years, 62–66 years, ≥67 years), sex, duration of hospitalization (1–3 days, ≥4 days), the reason for percutaneous coronary intervention (PCI; CCS or ACS), a scheduled second hospitalization, referral for coronary artery bypass grafting, hyperlipidemia, hypertension, diabetes mellitus, history of PCI, chronic obstructive pulmonary disease, previous ACS, peripheral artery disease, documented SC indication, participation in a cardiac rehabilitation program, level of education (primary school vs higher than primary school), the Fagerström index, and the load of pack‑years. A backward selection at the level of 0.1 was implemented to fit the model and identify factors at a level of significance of 5%. The ORs with 95% CIs were calculated. A P value below 0.05 was considered significant. All analyses were performed using the Stata 14.1 software (StataCorp, LP, College Station, Texas, United States).
Results
The patient characteristics are presented in Table 1. Among the 241 individuals available for the follow‑up interview, 168 (69.7%) were men. The mean (SD) age of the patients was 61.2 (9.3) years, and 115 individuals (47.7%) had ACS. The median (IQR) hospitalization duration was 5 (3–8) days, and a second‑stage procedure was planned for 67 patients (27.8%). A total of 124 participants (60.2%) declared that they intended to stop smoking, 31 (12.9%) had no previous SC attempts, and 76 (31.5%) participated in a cardiac rehabilitation program. At the end of the follow‑up, 161 patients (66.8%) declared persistent smoking with active tobacco use during the previous 6 months, and 80 (33.2%) declared SC with less than 1 cigarette smoked during the preceding 30 days. Furthermore, 24 patients (9.9%) did not receive written information regarding SC on the discharge card. Passive smoking was declared by 110 patients (45.6%). Any form of pharmacological treatment (nicotine substitute therapy, cytisine, varenicline, or bupropion) for SC was prescribed for 64 patients (26.5%). In the group declaring SC immediately after the hospitalization, 40 (50%) patients withdrew from smoking, and 74 (92.5%) indicated health issues as the main reason for SC. Seventy patients (29%) considered SC before the hospitalization, while 65 (27%) declared that they considered SC during the hospitalization.
Variable | Patients declaring smoking continuation (n = 161) | Patients declaring smoking cessation (n = 80) | P value |
Data are presented as number (percentage) of patients unless indicated otherwise.
Abbreviations: ACS, acute coronary syndrome; IQR, interquartile range; PCI, percutaneous coronary intervention | |||
Age, y, mean (SD) | 61 (9) | 62 (9.8) | 0.55 |
Male sex | 111 (68.9) | 57 (71.25) | 0.71 |
Duration of hospitalization, d, median (IQR) | 3 (3–6) | 7 (3–11) | <0.001 |
PCI due to ACS | 55 (47.8) | 60 (52.2) | <0.001 |
Diabetes | 36 (22.4) | 17 (21.3) | 0.84 |
Hypertension | 116 (72) | 54 (67.5) | 0.47 |
Hyperlipidemia | 79 (49) | 46 (57.5) | 0.22 |
History of ACS | 29 (18) | 7 (8.75) | 0.06 |
History of PCI | 34 (21.1) | 6 (7.5) | 0.007 |
Scheduled second hospitalization | 32 (19.9) | 35 (43.8) | 0.005 |
Participation in a cardiac rehabilitation program | 41 (25.5) | 35 (43.8) | 0.004 |
Passive smoking | 78 (49) | 32 (41) | 0.24 |
Living alone | 31 (19.6) | 13 (16.5) | 0.55 |
In the univariable logistic regression analysis, longer duration of hospitalization (≥4 days; OR, 4,25; 95% CI, 2.33–7.71), ACS on admission (OR, 3.7; 95% CI, 2.09–6.55), a scheduled second hospitalization (OR, 3.13; 95% CI, 1.74–5.64), and participation in a cardiac rehabilitation program (OR, 2.28; 95% CI, 1.29–4.01) were associated with higher odds of SC, whereas a history of PCI (OR, 0.3; 95% CI, 0.12–0.75) correlated with a lower likelihood of SC. In multivariable logistic regression analyses, the strongest determinant for SC was hospitalization duration of 4 days or longer (OR, 3.62; 95% CI, 1.9–6.89), followed by a scheduled second hospitalization (OR, 2.54; 95% CI, 1.32–4.86), a smoking load of 51 pack‑years or greater (OR, 2.28; 95% CI, 1.16–4.47), and a Fagerström index of 4 points or lower (OR, 1.96; 95% CI, 1.01–3.79) (Table 2).
Variable | OR (95% CI) | P value |
Abbreviations: OR, odds ratio | ||
Duration of hospitalization ≥4 d | 3.62 (1.9–6.89) | <0.001 |
Scheduled second hospitalization | 2.54 (1.32–4.86) | 0.005 |
Smoking load ≥51 pack‑years | 2.28 (1.16–4.47) | 0.02 |
Fagerström score ≤4 points | 1.96 (1.01–3.79) | 0.045 |
Discussion
In the cohort of patients who underwent CA, 33.2% stopped smoking during the 6‑month follow‑up. The strongest determinant of successful SC was prolonged hospital stay. Other strong determinants were repeated hospitalization, low nicotine dependence measured by the Fagerström index, and a high load of pack‑years.
In the present study, the percentage of patients who smoked before CA was 24.8%, and was similar to that in the general Polish population. The WOBASZ and WOBASZ II studies revealed a decrease in the number of active smokers in Poland, but still reported that in 2014, 30% of men and 21% of women were active tobacco users.21 The rates of active smokers with established CAD in the European populations from the EUROASPIRE II–IV trials were rather constant, with a slight decrease from 21% in 2000 to 18% in 2013.9 In our study, the rate of patients who stopped smoking was substantially lower than that reported in the EUROASPIRE IV study derived from Poland (33.2% vs 48%, respectively).13 That study differed significantly from ours with respect to the sample size (137 vs 241 patients, respectively); however, in both studies, the patients received only minimal counseling, including information on the potential risks related to smoking continuation. Also, the definition of smoking in the present analysis was similar to that used in the EUROASPIRE IV study, taking into consideration smoking in the month preceding the completion of the questionnaire. The overall SC rate in the EUROASPIRE IV study varied substantially between countries and ranged from 29% to 73%.13
In the present study, the determinants of successful SC were prolonged hospital stay, repeated hospitalization, low nicotine dependence, and a high load of pack‑years. Interestingly, most of the previous studies identified similar predictors.
We found that prolonged hospital stay increased the likelihood of SC. It is possible that this teachable moment14 played a role that was further strengthened by the length of the hospital stay. Data regarding the smoking ban during hospitalization and compliance with this recommendation were not collected in the present study; however, we believe that prolonged discontinuation of smoking may facilitate the process of quitting. Additionally, counseling initiated during the hospitalization increases the chances of SC.22 Hopner et al23 reported that a longer hospital stay and a higher number of newly prescribed drugs tended to be associated with SC.23 In their study, the patients who experienced complications had a higher chance of SC. In the present study, we did not evaluate the frequency of postprocedural complications, but a longer hospital stay is likely to be associated with more complications. A short hospital stay at the time of the index myocardial infarction (MI) was associated with a lower chance of SC in a study by Gerber et al.24 Repeated hospitalization as a determinant of SC may be attributed to a similar problem, that is, CAD extension. Rehabilitation following a cardiovascular event was related to a higher likelihood of SC in the POLASPIRE study.25 In our work, the univariable analysis showed that SC occurred more frequently among the patients who participated in a cardiac rehabilitation program; however, this finding was not confirmed in the multivariable analysis. Of note, our study might be biased due to the low participation rate. It may be assumed that the patients who completed the follow‑up were among the more compliant ones, who were more likely to attend a rehabilitation program.
The high load of pack‑years as a determinant of SC may be paradoxical. Pack‑years refer to a combination of the load and duration of smoking. Most studies link the smoking load with a higher risk of persistent smoking.26 However, data regarding the age of the patients in this respect are conflicting. In a study of heavily‑smoking patients who experienced AMI at a young age, a history of MI due to tobacco use was associated with a higher risk of persistent smoking.24 In a study of the Polish population, Kozieł et al25 identified older age as a factor linked to a higher likelihood of SC; however, a longer duration of smoking was linked to a lower possibility of SC in the same study. In the EUROASPIRE IV study, Snaterse et al13 reported that older age was linked to a higher chance of SC (OR, 1.50; 95% CI, 1.09–2.06).
Pharmacotherapy significantly increases the rate of SC, but it is rarely implemented in clinical settings.25,27 Only 64 patients (26.5%) in the present study used any form of pharmacological aid aimed at facilitating SC. We failed to find any correlation between drug use and SC; however, as we reported previously,28 cytisine use may be effective only in the patients who completed the treatment. We did not analyze e‑cigarette usage, which might be relevant with respect to effective SC but is also associated with harmful effects.29 The relatively low SC rates, along with low levels of pharmacological support, may suggest that physicians pay little attention to smoking as a risk factor.30
Other predictors of persistent smoking after AMI identified in the previous studies were sociodemographic factors, such as a low level of education, low family income, and the lack of a steady partner.24 We also analyzed these factors but failed to find any correlation with SC.
The Fagerström index reflects the level of nicotine dependence. We found that the index level of 4 points or lower was related to a higher chance of SC. This is consistent with previous findings suggesting nicotine dependency to be a barrier to successful SC.31,32 The mean Fagerström index found in our analysis was similar to that previously reported in a cross‑sectional European study (4.4 vs 5.0, respectively).33
Passive smoking is associated with an increased cardiovascular risk and a decreased chance of SC. Although we did not find a significant correlation between these factors in the multivariable analysis, previous studies confirmed passive smoking as a factor decreasing the chances of SC.25,34,35
Study limitations
Data regarding smoking addiction and nicotine dependence, as well as sociodemographic information were self‑reported, which may be a substantial limitation, as this method is prone to measurement bias. Moreover, SC was not validated using an objective test. Additionally, a substantial number of patients were not available for the follow‑up questionnaire; therefore, the results might be biased due to the low participation rate. A recently published study by Kamiński et al36 investigated the effect of pictorial warnings placed on the cigarette packs, which were introduced in the period coinciding with the trial screening; however, these warnings decreased the sale of cigarettes nonsignificantly, and only in the first year after their introduction, and are unlikely to influence our results.
Conclusions
The study indicated that a significant group of patients who underwent CA were current smokers. Self‑reported SC rates after the procedure were still relatively low. Prolonged hospital stay, repeated hospitalization, and low nicotine dependence measured using the Fagerström index, as well as a high load of pack‑years increased the chances of SC. The results highlight the need for an intensive and repetitive in‑hospital counseling with respect to SC in all smokers.
- World Health Organization. WHO global report on trends in prevalence of tobacco use 2000‑2025, third edition 2019. https://www.who.int/publications/i/item/who‑global‑report‑on‑trends‑in‑prevalence‑of‑tobacco‑use‑2000‑2025‑third‑edition. Accessed November 8, 2021.
- West R. Assessment of dependence and motivation to stop smoking. BMJ. 2004; 328: 338‑339. | Crossref
- Fong GT, Hammond D, Laux FL, et al. The near‑universal experience of regret among smokers in four countries: findings from the International Tobacco Control Policy Evaluation Survey. Nicotine Tob Res. 2004; 6: 341‑351. | Crossref
- Mullins R, Borland R. Do smokers want to quit? Aust N Z J Public Health. 1996; 20: 426‑427. | Crossref
- Moryson W, Stawińska‑Witoszyńska B. Trends in premature mortality rates among the Polish population due to cardiovascular diseases. Int J Occup Med Environ Health. 2022; 35: 27‑38. | Crossref
ARTICLE INFORMATION