A 26‑year‑old woman in the 30th week of pregnancy presented for ultrasound examination due to a painless anterior midline cervical mass felt in the hyoid bone region. The lesion had appeared several weeks earlier. The medical history was not contributory. Thyroid gland palpation was otherwise normal, and no cervical lymphadenopathy or tongue protrusion were observed. Thyroid function blood tests were also normal. Detailed neck ultrasound (Figure 1A and 1B) and craniofacial magnetic resonance imaging (Figure 1C and 1D) were performed without contrast due to pregnancy. In Figure 1C and 1D a well‑demarcated polycyclic cystic lesion was observed in the midline in the vicinity of the hyoid bone. The lesion measured 13 × 18 × 23 mm (sagittal × anteroposterior × craniocaudal) and contained multiple internal septa up to 2 mm thick. High protein or post‑hemorrhagic content was observed in some fluid spaces with an increased signal in the magnetic resonance T1‑weighted sequences. The lesion was in the fatty tissue between the platysma and laterally displaced geniohyoid muscles. Posteriorly, it adhered directly to the unchanged hyoid bone and slightly deformed the hyoglossus muscle. There were no signs of infiltration of the surrounding structures. Ultrasound‑guided fine‑needle aspiration cytology (FNAC) of the lesion was conducted based on the imaging results. The biopsy revealed a neoplastic lesion (suggestive of salivary‑derived proliferation). Therefore, the patient was qualified for surgery. The tumor was removed together with the body of the hyoid bone using the Sistrunk’s method in the 34th week of pregnancy due to a strong suspicion of aggressive malignancy based on FNAC results. The surgery and the perioperative period were uncomplicated. The final surgical histopathology demonstrated papillary carcinoma in a thyroglossal duct cyst (Figure 1E‑1G). Histologically, the papillary thyroglossal duct cyst carcinoma was enclosed by a thin wall of connective tissue. A branched framework of papillary glands filled with colloid was identified within the cyst. The papillae were covered by a single layer of epithelial tumor cells with cell nuclei showing typical alterations. The cancer infiltrated the adipose tissue and muscles. The tumor exhibited a similar immunophenotype as the tumors of thyroid origin.
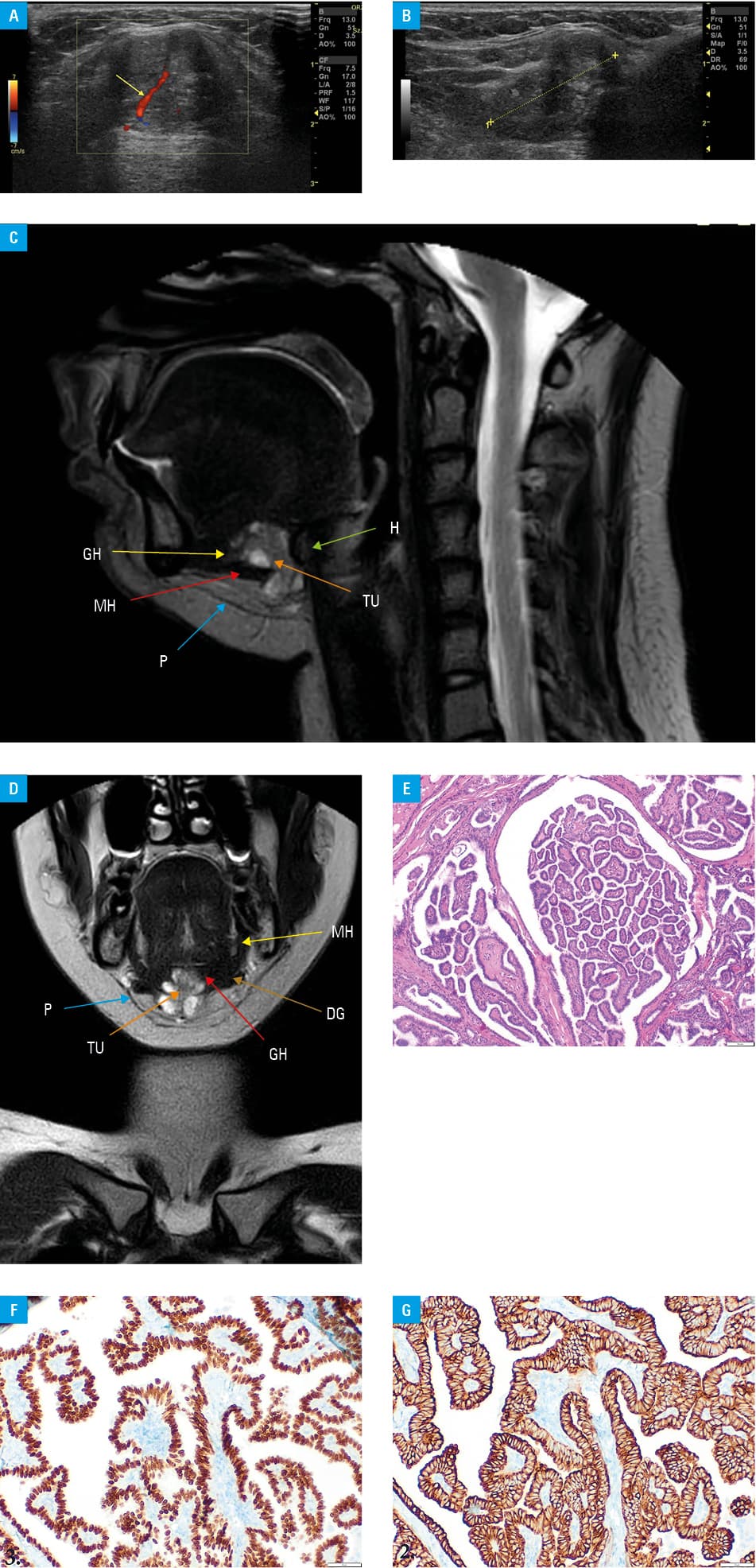
Abbreviations: DG, digastric muscle; GH, geniohyoid muscle; H, hyoid bone; MH, mylohyoid muscle; P, platysma muscle; TU, tumor
At the 40th week of gestation, a healthy baby was delivered without complications. In the second month postpartum, the woman was eligible for a follow‑up thyroidectomy with lymphadenectomy (histopathology revealed colloid nodular goiter with no cancer signs in the thyroid gland and central cervical nodes). The patient was treated with radioactive iodine 131I with the activity of 100 mCi, and advised to take suppressive doses of L‑thyroxine. After a 2‑year follow‑up, thyroglobulin level was undetectable, and the patient showed no tumor recurrence.
The thyroglossal duct cyst (TGDC) is the most common congenital lesion of the neck and usually occurs as a benign cystic mass in the anterior cervical triangle. It affects approximately 7% of the general adult population.1 Embryologically, the thyroid gland arises from the floor of the pharyngeal gut and descends as a diverticulum that remains merged to the gut by a narrow canal—the thyroglossal duct. Typically, the thyroglossal duct obliterates by the 10th week of gestation. Occasionally, it can remain as a cyst or a duct or as an ectopic thyroid tissue within a cyst or a duct.2 Malignant neoplasms arising from TGDC are rare, with an incidence of 1% to 3% of all TGDCs. The women to men ratio is almost 3:1.3 More than 75% of TGDC carcinomas are diagnosed incidentally with definitive histopathology after removal of the apparently benign TGDC. In approximately 25% of cases, clinical or radiological findings raise preoperative suspicion of malignancy.4 Up to 95% of patients with TGDC carcinoma presented with an asymptomatic neck mass. Only about 3% of the patients complain of dysphagia and pain. TGDC carcinoma can arise from the thyroid tissue of the cyst. Therefore, the most common primary TGDC carcinoma is papillary thyroid cancer (in more than 90% of cases).5 The reference surgical technique for TGDC is the Sistrunk’s procedure that comprises resection of the body of the hyoid bone. In high‑risk patients, thyroidectomy is recommended. TGDC papillary carcinoma has a good prognosis, with 5- and 10‑year overall survival rates between 100% and 95.6%, respectively (in comparison, typically located papillary thyroid carcinoma is associated with survival rates of 96% at 5 years, and 93% at 10 years).2
- Lancini D, Lombardi D, Piazza C. Evidence and controversies in management of thyroglossal duct cyst carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2021; 29: 113‑119. | Crossref
- Alatsakis M, Drogouti M, Tsompanidou C, et al. Invasive thyroglossal duct cyst papillary carcinoma: a case report and review of the literature. Am J Case Rep. 2018; 19: 757‑762. | Crossref
- Plaza CP, López ME, Carrasco CE, et al. Management of well‑differentiated thyroglossal remnant thyroid carcinoma: time to close the debate? Report of five new cases and proposal of a definitive algorithm for treatment. Ann Surg Oncol. 2006; 13: 745‑752. | Crossref
- Rayess HM, Monk I, Svider PF, et al. Thyroglossal duct cyst carcinoma: a systematic review of clinical features and outcomes. Otolaryngol Head Neck Surg. 2017; 156: 794‑802. | Crossref
- Huang PK, Hsieh LC, Leu YS. Thyroglossal duct cyst papillary carcinoma with airway compromise. Ear Nose Throat J. 2021 Jun 8. [Epub ahead of print] | Crossref
ARTICLE INFORMATION