Recent advances in the diagnosis and management of autoimmune hepatitis
Key words: autoantibodies, autoimmune hepatitis, autoimmune liver diseases, azathioprine, mycophenolate mofetil



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Recent advances in the diagnosis and management of autoimmune hepatitis
Autoimmune hepatitis (AIH) is an acute or chronic inflammatory disease of the liver caused by an immune response of unknown origin. It affects people from all ethnic groups irrespective of age or sex. AIH is characterized by hyperglobulinemia, presence of circulating autoantibodies, and liver inflammation. The clinical picture of the disease varies from asymptomatic or mild to severe acute hepatitis or liver failure. A timely and prompt diagnosis is of utmost importance to prevent progression to advanced liver disease by immediate initiation of immunosuppressive treatment. So far, several diagnostic scoring systems have been proposed, which incorporated demographic data as well as biochemical, clinical, and histological characteristics of the disease. However, due to the high heterogeneity of the disease presentation, diagnosis of AIH remains challenging. Most patients initially respond to first‑line treatment, which consists of corticosteroids combined with azathioprine or mycophenolate mofetil. However, insufficient response to the treatment and intolerance due to side effects are common, so a significant proportion of patients require second- and / or third‑line therapies. Herein, we review the challenges and recent advances in AIH diagnosis and management.
Introduction
Autoimmune hepatitis (AIH) is a complex immune disease of unknown etiology. It is serologically characterized by high levels of aminotransferases, immunoglobulin G (IgG), and autoantibodies, whereas histologically, it can manifest as lymphocytic infiltration of the liver and interface hepatitis.1-3
AIH is a global disease with diverse clinical characteristics and prevalence depending on age, sex, ethnicity, and geographic location.4 The incidence ranges from 0.67 to 2.0 patients per 100 000 people / year, and the prevalence from 4.0 to 24.5 patients per 100 000 people in different regions.5,6 AIH mostly affects women, with a male‑to‑female ratio of 1:4 to 1:6.7,8 It was previously thought that the incidence of AIH peaks in children, teenagers, and adults between the fourth and sixth decade of life.1-3 However, recent research from our group has shown that AIH can also affect patients over the age of 70 years. Notably, the elderly patients presented with a more advanced disease at diagnosis.9
Even though the etiology of AIH is still not clear, there is evidence that the development of the disease is based on genetic predisposition as well as environmental and epigenetic factors.8,10-13 Human leukocyte antigen (HLA) locus is known to interfere with the genetic predisposition to AIH, with the most prominent association found with HLA‑DRB1*0301 and HLA‑DRB1*0401.14 Furthermore, outside of the major histocompatibility complex, many single‑nucleotide polymorphisms have been linked to the clinical phenotype, such as variants of SH2B3 and CARD10,13 CD28‑CTLA4‑ICOS, and SYNPR.15 In this context, we have recently shown in Greek patients with AIH that the IL28B rs12979860 CC genotype is associated with higher rates of successful treatment withdrawal after achievement of complete biochemical response (CBR), while no association was found between PD1.3 polymorphisms and susceptibility to AIH or disease severity at presentation, response to treatment, and outcome.16
Exposure of genetically predisposed individuals to certain environmental factors (viruses, microbes, xenobiotics, drugs, herbal supplements) has been linked to the development of AIH.10,17-22 New data relate AIH to the gut microbiome and immune system activation through gut‑liver axis signaling.23 Finally, DNA methylation, histone adjustments, and micro‑RNAs are examples of epigenetic alterations that may regulate the gene expression even though they do not change the DNA sequence.10 We recently found DNA methylation changes in circulating immune cells and at the histological level in patients with AIH, which were associated with disease activity and influenced by immunosuppressive treatment.12
This review aims to summarize the recent challenges and advances in the diagnosis and management of AIH.
Diagnosis
AIH is diagnosed using a combination of clinical, serological, biochemical, and histological indicators. Exclusion of any other cause of liver disease (viral hepatitis A to E, drug‑induced hepatitis, alcoholic liver disease, primary sclerosing cholangitis, primary biliary cholangitis, variant forms of AIH, Wilson’s disease, nonalcoholic fatty liver disease, α-1 antitrypsin deficiency, hemochromatosis, and celiac disease) is obligatory1-3 (Table 1). A liver biopsy is necessary as part of the diagnostic process, provided there are no contraindications.1-3,7,8
Abbreviations: AIH, autoimmune hepatitis; PBC, primary biliary cholangitis; PSC, primary sclerosing cholangitis |
Viral hepatitis A to E (acute or chronic) |
Drug‑induced liver injury |
Alcoholic liver disease |
PBC |
PSC |
Variant forms of AIH (AIH/PBC, AIH/PSC, autoimmune sclerosing cholangitis in children) |
Wilson’s disease |
Nonalcoholic fatty liver disease |
Hemochromatosis |
α-1 Antitrypsin deficiency |
Celiac disease |
Clinical characteristics
The clinical presentation of AIH in adults is highly heterogeneous. The most prevalent clinical phenotype in about two‑thirds of the patients is marked by an insidious onset, either totally asymptomatic or with the presence of nonspecific symptoms (malaise, fatigue, anorexia, arthralgias, weight loss, etc). Therefore, it is critical to include AIH in the differential diagnosis in all individuals with transaminasemia of any severity, regardless of their ethnicity, sex, or age.1-3 Although an increased IgG level is characteristic of AIH patients, about one‑tenth have a normal IgG concentration at presentation.24 About one‑third of the patients present with acute disease, either with acute exacerbation of chronic AIH or with genuine acute AIH with no histological evidence of chronic liver disease. Due to the fact that liver autoimmune serology tests may be negative and IgG levels can be normal in such cases of acute presentation, clinicians may overlook AIH, although detailed testing for autoantibodies in specialist laboratories may be helpful.7,8,25 Unfortunately, owing to a delay in the diagnosis, one‑third of the patients are already cirrhotic at presentation.26-29 Extrahepatic autoimmune diseases are more prevalent in patients with AIH, with autoimmune thyroid disease being the most common. Moreover, their first‑degree relatives also have a higher rate of autoimmune diseases than the general population. These extrahepatic manifestations could be the leading clinical manifestations at diagnosis.30
Serology
Detection of autoantibodies is essential not only for the diagnosis but also for the classification of AIH.8,31-33 Patients with AIH type 1 (AIH‑1) are positive for antinuclear autoantibodies (ANA) and / or smooth muscle autoantibodies (SMA). Adults with a titer of at least 1:40 and children with a titer of at least 1:20 on indirect immunofluorescence (IIF) are considered positive.33-35 Perinuclear antineutrophil cytoplasmic antibodies (p‑ANCA) may also be detected in AIH‑1. Individuals with AIH type 2 (AIH‑2) are positive for anti–liver kidney microsomal type 1 (anti‑LKM1) or, rarely, for anti–liver kidney microsomal type 3 (anti‑LKM3), and / or anti–liver cytosol type 1 (anti‑LC1) autoantibodies.2,7,31 IIF titers of at least 1:40 in adults and 1:10 in children are considered positive for both anti‑LKM and anti‑LC1 autoantibodies.33-35
The presence of soluble liver antigens / liver pancreas antibodies (anti‑SLA/LP) was formerly considered a third category of AIH. However, such a classification was abandoned when it became clear that the characteristics of AIH patients positive for anti‑SLA/LP do not differ from those of individuals with AIH‑1.36 Anti‑SLA/LP levels should be tested by an enzyme‑linked immunosorbent assay (ELISA) or immunoblotting, and they are detected in 20% to 30% of AIH cases. These antibodies are highly specific for AIH and the discovery of their presence is particularly helpful in patients who are seronegative for the conventional antibodies.37,38 Although there is no strong evidence of a clinically distinct role of these antibodies,37,39 we demonstrated that anti‑SLA/LP–positive patients exhibited a delayed initial CBR, reduced rates of corticosteroid cessation, and lowered rates of remission following complete treatment withdrawal.38 Among other nonconventional antibodies, anti-α-actinin antibodies can predict the response to treatment and, either by themselves or in conjunction with anti–filamentous (F)-actin antibodies, appear to enable identification of patients with active or advanced disease.40-42
Considering the fact that more than 95% of the patients show serological reactivity if autoantibodies are tested according to the guidelines, clinicians should be aware of the importance of the required tests and know how to interpret the laboratory results. IIF is a subjective procedure that should be carried out in strict accordance with the guidelines. Therefore, the International Autoimmune Hepatitis Group (IAIHG) published in 2004 a consensus statement with precise methodological details regarding liver autoimmune serology, in which IIF was suggested as the method of choice to screen for liver‑related autoantibodies.33 The methodology uses a freshly‑fixed rodent multiorgan substrate panel (kidney, liver, and stomach), allowing for the detection of ANA, SMA, anti‑LKM, anti‑LC1, and antimitochondrial antibodies (AMA).1,2,31,33,43 However, in real‑life setting, the use of the abovementioned in‑house substrates in each laboratory locally for a routine screening of the patients with suspected AIH is almost impossible. Therefore, many laboratories use commercially available tissue sections, even though their quality and sensitivity are questionable.8,33 Furthermore, many centers (particularly in the United States) perform ELISA and IIF on HEp‑2 cells instead of rodent tissues, even though the sensitivity and specificity of these tests are debatable, and it is unclear how the results may be translated to fit the diagnostic scores.8,31,43 The reported target autoantigens of the detectable autoantibodies in AIH and their clinical significance are summarized in Table 2.
Antibody | Target autoantigens / detection methods | Clinical significance |
a For updates on their detection by HEp‑2 cells and ELISA, see Table 4 and text.
Abbreviations: ANA, antinuclear antibodies; anti‑CYP2D6, cytochrome P450 2D6 antibodies; anti‑LC1, anti–liver cytosol antibodies type 1; anti‑LKM1, anti–liver kidney microsomal antibodies type 1; anti‑LKM3, anti–liver kidney microsomal antibodies type 3; anti‑Ro52, antibodies against the ribonucleoprotein / Sjogren syndrome A 52 kDa antigen; anti‑SLA/LP, soluble liver antigens/liver pancreas antibodies; ASC, autoimmune sclerosing cholangitis; ELISA, enzyme‑linked immunosorbent assay; FTCD, formiminotransferase cyclodeaminase; HCV, hepatitis C virus; HDV, hepatitis D virus; IBD, inflammatory bowel disease; IIF, indirect immunofluorescence; pANCA, perinuclear antineutrophil cytoplasmic antibodies; pANNA, perinuclear antineutrophil nuclear antibodies; SMA, smooth muscle antibodies UGT1; family 1 of uridine diphosphate glucuronosyl‑transferases; VG, vessel glomerular; VGT, vessel glomerular tubular; others, see Table 1 | ||
ANA | Chromatin, histones, single- and double‑stranded DNA, centromere, cyclin A, ribonucleoproteins; undefined antigens in 20%–30% of cases / IIF on triple rodent tissue substratesa | Defines AIH‑1 but not specific; rarely present in AIH‑2 |
SMA | Filamentous actin, vimentin, desmin; undefined antigens in about 20% of cases / IIF on triple rodent tissue substratesa | Defines AIH‑1 especially if combined with ANA; VG or VGT patterns are highly specific; rarely present in AIH‑2 |
Anti‑LKM1 | CYP2D6 (molecular weight, 50 kDa) / IIF on triple rodent tissue substrates; also identified by ELISA or immunoblotting | Defines AIH‑2; highly specific (absent in AIH‑1) but present in HCV (10% of cases) |
Anti‑LKM3 | UGT1 (molecular weight, 55 kDa) / IIF on triple rodent tissue substrates or immunoblotting | Rare but specific antibody; defines AIH‑2 but present in up to 13% of HDV patients |
Anti‑LC1 | FTCD (molecular weight, 58–62 kDa) / IIF on triple rodent tissue substrates; also identified by ELISA or immunoblotting (very helpful in cases with concurrent anti‑LKM1 detected by IIF) | Defines AIH‑2 (absent in AIH‑1); liver‑specific antibody usually concurrent with anti‑LKM1; can be the only antibody (10% of AIH‑2 cases) |
Anti‑SLA/LP | Synthase converting O‑phosphoseryl‑tRNA (Sep) to selenocysteinyl‑tRNA (Sec) (molecular weight, 50 kDa) / ELISA or immunoblotting | Specific to AIH‑1 (15%–30% of cases; specificity, 99%); rarely present in AIH‑2; concurrent with anti‑Ro52 antibodies (77%–98% of cases); signifies the need for permanent immunosuppression |
pANCA/pANNA | Many reported but actually unknown target autoantigens / IIF on fixed neutrophils | Almost exclusively in AIH‑1 (60%–96%); isolated detection in very few patients; present also in patients with IBD, PSC, and ASC |
Liver histology
Every patient with suspected AIH should have a liver biopsy performed unless there is a contraindication.1-3 Apart from facilitating the diagnosis, liver biopsy is essential to the diagnostic scoring systems.34,35 According to the simplified criteria for AIH diagnosis, the presence of 3 histological characteristics is essential for defining a case as typical: (1) interface hepatitis (inflammation of hepatocytes at the portal‑lobular interface with lymphoplasmacytic cells spreading into the lobule), (2) emperipolesis (presence of a plasma cell or lymphocyte inside the cytoplasm of hepatocytes), and (3) rosettes (a small group of hepatocytes arranged around a small central lumen).35 Recent studies, however, raised doubts about the usefulness of hepatocyte rosettes and emperipolesis as typical AIH characteristics as both findings were suggested to be more indicative of liver cell damage.44,45
The International AIH Pathology Group recently issued a consensus statement46 that proposed a uniform approach to the diagnosis of AIH at the histological level (Table 3). The consensus opinion is that even though emperipolesis and hepatocyte rosettes are not considered specific characteristics of AIH, they can be reported as surrogate markers of the disease severity.46 The authors think that the inflammatory pattern of interface hepatitis and lymphoplasmacytic infiltration appear to be more specific for AIH.46 In the absence of histological lesions suggestive of another disease of the liver, AIH is considered “likely” if there is predominant portal hepatitis with lymphoplasmacytic infiltrates in association with more than mild interface hepatitis and / or more than mild lobular hepatitis. AIH is also considered “likely” if there is predominant lobular hepatitis with or without centrilobular necroinflammation and at least 1 of the following: (1) portal lymphoplasmacytic hepatitis or (2) interface hepatitis or portal‑based fibrosis, again in the absence of histological characteristics suggestive of another hepatic disease.46 Moreover, liver biopsy is crucial to investigate for the presence of variant syndromes of AIH or other concurrent liver diseases, such as alcoholic or nonalcoholic fatty liver disease.2,47-49
Portal hepatitis | Lobular hepatitis |
Likely AIH | |
Portal lymphoplasmacytic infiltration with at least 1 of the following characteristics:
In the absence of histological features suggestive of another liver disease | More than mild lobular hepatitis (with or without centrilobular inflammation) with at least 1 of the following characteristics:
In the absence of histological features suggestive of another liver disease |
Possible AIH | |
In the absence of histological features suggestive of another liver disease
OR
In the presence of histological features suggestive of another liver disease |
In the absence of histological features suggestive of another liver disease
OR
In the presence of histological features suggestive of another liver disease |
Unlikely AIH | |
In the presence of histological features suggestive of another liver disease |
In the presence of histological features suggestive of another liver disease |
The patients who are reluctant or unable to undergo a liver biopsy may benefit from noninvasive methods to assess liver fibrosis at baseline and during follow‑up. Transient elastography (TE) is a well‑validated, noninvasive approach for the evaluation of liver fibrosis, also in patients with AIH,50 as elevations in liver stiffness measurements (LSMs) during the disease process have been associated with the disease progression and outcome.51 Unfortunately, determination of LSMs by TE at baseline is not reliable for the assessment of the fibrosis stage, particularly in the patients with acute hepatitis, due to elevated levels of transaminases. However, even though not reliable for staging, these measurements still seem important, at least as surrogate markers of the necroinflammatory activity of AIH, because they were found to decrease in parallel with the biochemical activity when CBR was achieved. Additionally, a combined 2‑dimensional shear wave elastography of the liver and spleen might be used to potentially solve the problem of fibrosis stage assessment at baseline in the patients with active AIH who are reluctant or unable to undergo the biopsy.52
FibroMeter vibration‑controlled TE (FMVCTE) is an innovative method that combines FibroMeter (FM) values and LSMs. We have recently shown that FMVCTE detects severe fibrosis in the patients with AIH at a similar rate to TE but with better specificity. Biochemical disease activity did not appear to impair their diagnostic accuracy, so both tests could be useful and efficient in detecting AIH patients with severe fibrosis.53
Diagnostic criteria
The clinical, serological, biochemical, and histological characteristics of the patients have been incorporated in several diagnostic criteria proposed for AIH diagnosis.34,35,54,55 The first criteria were developed in 1993 by Johnson et al,54 and they were updated in 199934 with the inclusion of 10 parameters (sex, detection of ANA, SMA, or anti–LKM‑1, alkaline phosphatase‑to‑alaninoaminotransferase [ALT] ratio, serum IgG level, detection of AMA, viral hepatitis B or C, history of alcohol consumption or hepatotoxic drug use, histological characteristics of the liver, and presence of extrahepatic autoimmune diseases).34 This scoring system was characterized by a high level of complexity, inclusion of a variety of parameters of questionable value, and insufficient validation. Our group validated the revised IAIHG score in patients with various liver diseases in 2007.56 It was shown clearly that the revised score was highly specific for the exclusion of AIH but not sensitive enough to identify AIH patients with coexisting liver diseases.
In 2008, the IAIHG simplified the diagnostic criteria by issuing a scoring system comprising only 4 parameters (liver histology, autoantibody titers, serum levels of γ-globulin or IgG, and absence of viral hepatitis).35 The score was found to bear 97% specificity and 88% sensitivity for diagnosing probable AIH and 99% specificity and 81% sensitivity for definite AIH. Several studies were performed to evaluate the simplified score in different centers. In this context, we have shown in a large group of 502 patients with diverse liver diseases including variant syndromes, that the simplified scoring system was less sensitive to exclude AIH in patients with concurrent liver disorders, reiterating the importance of liver biopsy.57 Of note, the IAIHG mentioned serious limitations that should be taken into account, such as the lack of standardization in autoantibody testing that may lead to inadequate scoring values, the need for other conventional methods for the detection of SLA/LP (as these autoantibodies are not detected by IIF), and the fact that the simplified score did not account for ANA and SMA detection by IIF on HEp‑2 cells or ELISA because of the higher titers of ANA/SMA on this specific substrate and the lack of standardization of ELISA tests for ANA and SMA detection.35
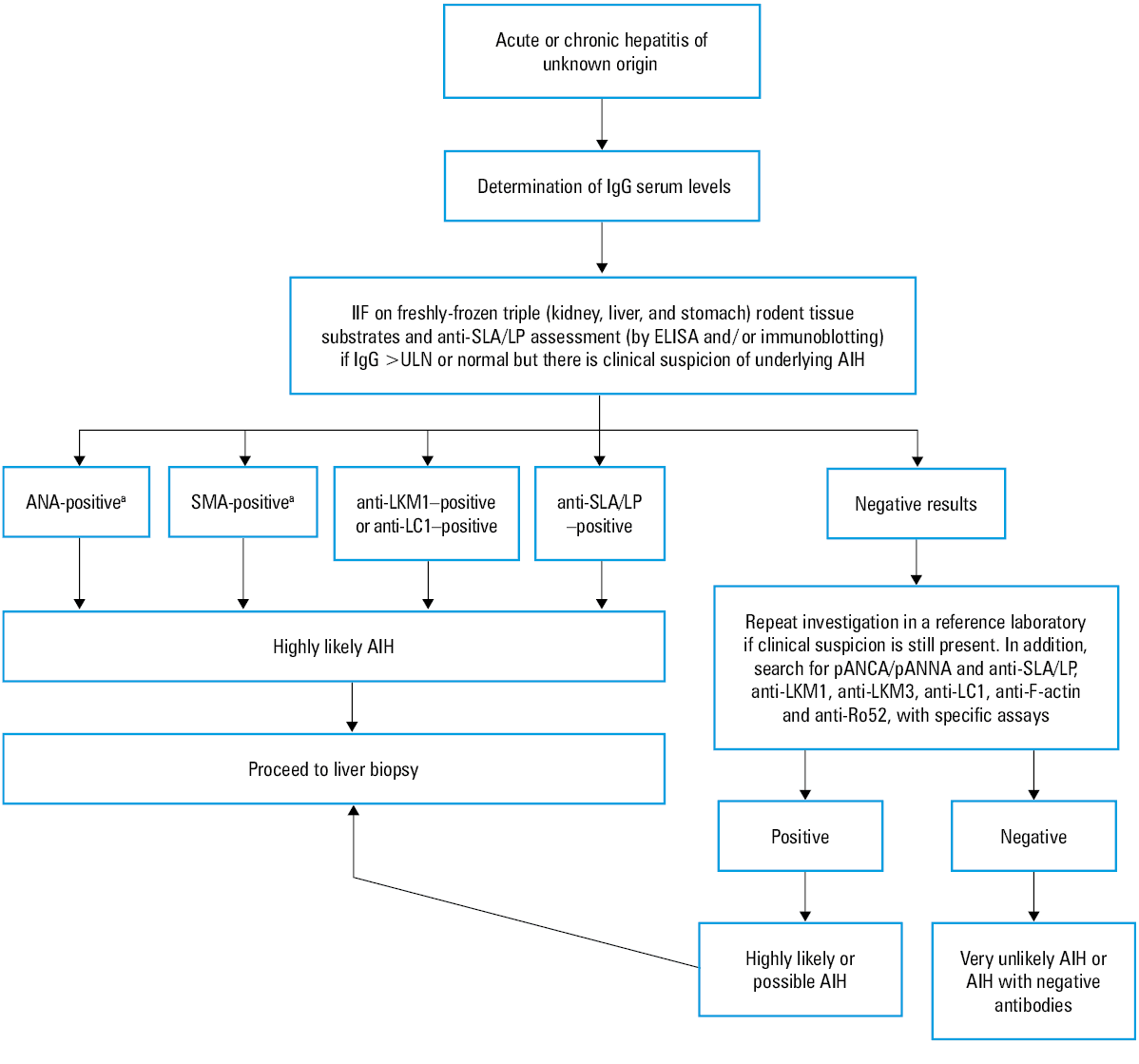
These issues have been recently addressed by the IAIHG55 (Table 4). The investigators compared the results of IIF performed on HEp‑2 cells and rodent tissue sections with respect to the reactivity for ANA and SMA in 113 AIH sera and 202 control samples from 3 European centers. They also investigated 3 different commercial ELISAs for ANA testing and 1 commercial ELISA for SMA testing.55 They concluded that HEp‑2 cells can be used as a reliable alternative substrate to rodent tissue sections if ANA titers are adapted to higher thresholds (≥1:160 for positivity and ≥1:320 for strong positivity). They further emphasized the necessity of reporting SMA patterns, as they confirmed a prior finding that SMA–vessel glomerular / vessel glomerular tubular patterns had the highest specificity for AIH diagnosis and correlated with F‑actin reactivity.58,59 Notably, F‑actin autoantibodies detected by ELISA enabled efficient identification of the subgroup of AIH patients with normal IgG levels. Finally, discrepancies in the performance of different ELISA kits for ANA detection were found, indicating that not only molecularly recognized nuclear antigens but also whole HEp‑2 nuclear extracts should be included to account for unrecognized nuclear autoantigens.55 As the cutoffs for these commercial ELISA kits have not been validated worldwide, there is a need for locally established cutoffs in each laboratory.55 Last but not least, if ELISA testing is negative and clinical suspicion for AIH is high, complementary testing by IIF should be done. A proposed diagnostic algorithm for AIH diagnosis is presented in Figure 1.
Feature | Cutoff | Pointsa |
a Sum of the points achieved (maximum 2 points for autoantibodies)
b IIF: >1:40 when assessed on rodent tissue sections; >1:80 or 1:160 for ANA when assessed on HEp‑2 cells, depending on local standards; ELISA: cutoffs established locally
c IIF: >1:80 when assessed on rodent tissue sections; >1:160 or 1:320 for ANA when assessed on HEp‑2 cells. ELISA: cutoffs established locally. Important note: if ELISA‑based autoantibody assessment is negative despite high clinical suspicion of autoimmune hepatitis, IIF should be performed in addition.
| ||
ANA or SMA/F‑actin | Positiveb | 1 |
ANA or SMA/F‑actin | Strongly positivec | |
Or anti‑LKM | ≥1:40 | 2 |
Or anti‑SLA | Positive | |
IgG | >ULN | 1 |
>1.1 × ULN | 2 | |
Liver histology (with evidence of hepatitis) | Compatible with AIH | 1 |
Typical AIH | 2 | |
Absence of viral hepatitis | Yes | 2 |
≥6: probable AIH | ||
≥7: definite AIH | ||
Abbreviations: anti–F‑actin, anti–filamentous actin antibodies; others, see Tables 1, 2, and 4
New biomarkers
The need for identifying new biomarkers for the diagnosis of AIH is of particular importance. A meta‑analysis by Zhang et al60 showed that ANA have moderate specificity (62%) and sensitivity (65%), while SMAs offer high specificity (93%) but moderate sensitivity (59%).60 On the other hand, anti‑SLA/LP exhibit very low sensitivity (19%) but the highest specificity (99%).60
IgG antibodies with a high capacity to bind to several proteins (human and nonhuman) were recently discovered using a protein microarray and verified using ELISAs in patients with AIH.61 This polyreactive IgG (pIgG) demonstrated a 25% and 14% greater specificity for diagnosing AIH than conventional ANA and SMA testing, respectively, and a considerably higher sensitivity than anti‑LKM and anti‑SLA/LP. Additionally, the new test showed a 12% to 20% higher accuracy than tests for conventional autoantibodies.61 Of interest, pIgG reactivity identified the majority of patients with autoantibody‑negative AIH (88%) and most of the AIH patients with normal IgG levels (71%).61 Moreover, after response to immunosuppression, pIgG values returned to the levels observed in patients with non–AIH liver diseases. The authors stressed that pIgG quantification will not eliminate the necessity for a liver biopsy in patients with AIH, but its high specificity could enhance the preselection for the biopsy and allow for a deferral or cancellation of the procedure in those with a low pretest probability of AIH.61
Treatment
Why should we treat patients with autoimmune hepatitis?
AIH is characterized by the same complications (cirrhosis, liver failure, hepatocellular carcinoma, and finally liver‑related death) as any other liver disease. When approaching patients with unexplained acute or chronic liver disease, keeping an open mind will ensure that this important and potentially treatable condition is not ignored, as the prognosis is poor with a 5‑year mortality rate of 50% if the disease is left undiagnosed and untreated.1-3 Even in the individuals with advanced fibrosis, immunosuppressive therapy can be effective. Indeed, the life expectancy of treated patients after 10 and 20 years of follow‑up may approach 80%.62-64
Indications for treatment
All AIH patients with at least more than mild disease should receive immunosuppression to achieve CBR and histological remission. Maintenance of CBR during maintenance therapy or even after treatment discontinuation prevents the patients from experiencing progression of the liver disease. Patients with severe fibrosis or cirrhosis and necroinflammatory activity should also be treated.1-3
AIH may resolve spontaneously in a proportion of patients, allowing for the therapy to be suspended. These patients should be monitored regularly (eg, every 3–6 months) to prevent missing a subsequent clinical and / or biochemical flare of the disease.1-3,65 The presence and severity of concomitant comorbidities, such as refractory arterial hypertension or diabetes, established osteoporosis, and previous or current psychosis, could influence treatment initiation in elderly asymptomatic patients with mild disease. In such situations, it is preferable to choose a watch‑and‑wait approach with close monitoring. Patients with inactive (“burned‑out”) cirrhosis rarely benefit from treatment and are more likely to experience serious drug‑related side effects.1-3,7
Goal of treatment
The therapeutic aim is to achieve remission of the disease at the histological level with as few drug‑induced complications as possible. Biochemical remission usually occurs 6 to 12 months earlier than the histological remission and its maintenance prevents further progression of liver disease. Biochemical remission also results in the disappearance of AIH‑related symptoms. The ideal outcome is to induce a sustained CBR and histological remission after treatment cessation.1-3
Recently, the IAIHG published a comprehensive assessment of response criteria and end points for AIH treatment to standardize definitions66 (Table 5). This will help hepatologists develop surrogate end points for AIH treatment and agree on end points in clinical studies, while providing patients with a better understanding of their outcomes. In this document, CBR was defined as normalization of both serum IgG and transaminase levels in no more than 6‑months after treatment initiation. Insufficient response was defined as a lack of CBR within 6 months of treatment initiation, although the panel proposed that the period of no more than 12 months since the beginning of therapy could be an alternative. According to the document, insufficient response can only be established in the case when the patient received the standard therapy (predniso[lo]ne at a starting dose of at least 0.5 mg/kg/day and a maintenance dose of up to 10 mg/day, and azathioprine as first‑line or mycophenolate mofetil [MMF] as second‑line therapy at a dose of at least 1–2 g/day, preferably 2 g/day) and compliance was established.66
End point | Definition |
Abbreviations: see Table 4 | |
Complete biochemical response | Normalization of serum transaminases and IgG below ULN no later than 6 months after initiation of treatment |
Insufficient response | Lack of complete biochemical response after 6 months of initiation of treatment |
Nonresponse | <50% decrease of serum transaminases within 4 weeks of initiation of treatment |
Remission | Hepatitis activity index <4/18; could be obtained 12 months after treatment initiation or at any other time point during treatment |
Intolerance to treatment | Any adverse event possibly related to the treatment as assessed by the treating physician, leading to potential discontinuation of the drug |
The IAIHG also simplified the definition of nonresponse to a reduction in serum transaminase levels by less than 50% within 4 weeks of treatment initiation. However, a recent study showed that an 8‑week response predicted a more favorable disease course, with a higher likelihood of achieving and maintaining a sustained CBR, whereas the 4‑week response did not, implying that 4‑week assessment may be a too early time point.67 The panel recognized that a remission of AIH can only be fully established at the histological level by the modified hepatitis activity index (<4/18). This can be assessed 12 months after initiation of treatment or at any time throughout the treatment. Finally, intolerance to treatment was agreed to refer to any adverse event that could be related to the therapy and result in drug withdrawal.66
International and national guidelines recommend that immunosuppressive treatment should be continued for at least 3 years and treatment cessation should be attempted only in those who achieved continuous CBR for at least the last 2 years of treatment.1-3 Especially, the patients characterized by serum ALT levels in the lower half of the upper limit of normal and IgG values below 1200 mg/dl can achieve higher rates of sustained CBR after treatment withdrawal.68 Liver biopsy before treatment withdrawal is advisable in all patients.1-3 The need for a second biopsy before stopping the treatment is due to the fact that normalization of transaminase and IgG values does not necessarily imply histological remission, particularly in cirrhotic patients.69 Indeed, Laschtowitz et al69 showed recently that only 26% of the cirrhotic AIH patients with normal ALT achieved histological remission, in contrast to 88% of the noncirrhotic patients with normal ALT. Adding normal IgG values to the analysis improved the diagnostic performance only modestly, with 29% of the cirrhotic AIH patients with normal IgG and ALT levels achieving histological remission. Apart from assessing the necroinflammatory activity of the disease, liver biopsy can help identify patients with concurrent liver disorders that can emerge during the disease course, such as hepatic steatosis due to corticosteroid treatment that developed in an index patient who initially did not suffer from nonalcoholic fatty liver disease.47,70
Standard treatment
Steroid induction therapy is the first‑line treatment option, followed by maintenance therapy using a steroid‑sparing agent. In this context, predniso(lo)ne alone, or more frequently in association with azathioprine, has been considered for more than 40 years as the first‑line treatment for AIH. Initial nonresponse should immediately raise doubts about AIH diagnosis or indicate problems with adherence to treatment.1-3 The European Association for the Study of the Liver and other societies recommend starting with a dose of 0.5 to 1 mg/kg/day of predniso(lo)ne and progressively tapering it down under rigorous transaminase level monitoring.1-3,7 However, it is critical to emphasize that clinicians should avoid applying the proposed schedules of corticosteroids (both initial dose and tapering) uniformly to all patients. The most appropriate initial dose and tapering should be individualized according to the disease severity at baseline, age, response to treatment, drug tolerance, and comorbidities.1-3,7 Rapid tapering of predniso(lo)ne to minimize adverse effects of corticosteroids is desirable but should be done under careful monitoring of liver biochemistry as the therapy is response‑guided. This approach seems to increase adherence to treatment, which is an important issue in teenagers and young adults.71
Azathioprine should be added after 2 weeks of steroid treatment at a starting dose of 50 mg/day and progressively increased according to the response or potential toxicity up to 1 to 2 mg/kg/day.1-3 The rationale for delaying azathioprine initiation is that it can be potentially hepatotoxic, especially in jaundiced patients, and may cause confusion with respect to the therapeutic response. Azathioprine can cause a variety of side effects (gastrointestinal complications, pancreatitis, arthralgia, fever, skin rash, hepatitis, opportunistic infections, bone marrow suppression, and malignancy).1-3,7,8,72 A recent large, international, retrospective study found that 15% of the patients discontinued azathioprine during the first year of treatment due to side effects, mainly gastrointestinal ones.73 Besides azathioprine intolerance, studies revealed suboptimal CBR in the long‑term (<50% of the patients), while almost none of the patients maintained CBR after azathioprine withdrawal, even though they had been in CBR for more than 2 years before stopping the therapy.74 These issues raise significant concerns about the long‑term efficacy of the standard treatments.
Budesonide is a synthetic glucocorticoid with local action and low systemic bioavailability due to its 90% hepatic first pass effect. The original randomized trial comparing fixed doses of 9 mg/day of budesonide with 40 mg/day of prednisone found that it was an effective substitute of prednisone in the induction treatment of nonsevere acute or chronic AIH without cirrhosis.75 As a result, the American Association for the Study of Liver Diseases (AASLD) suggested budesonide as a possible option for first‑line treatment in AIH.3 However, that study had many limitations: the blinded phase of randomization for a chronic disease with several relapses and remission periods was only 6 months, the normalization of IgG levels was not included in the response criteria, and in contrast to an individualized tapering schedule in the budesonide group according to biochemical response, the prednisone group followed a fixed‑dose reduction schedule regardless of response, which may have resulted in a potential therapeutic bias.75 In addition, surprisingly enough, low response rates and high frequency of side effects were reported in the controls, while data on long‑term efficacy and outcomes (histology, progression, survival) were missing. Moreover, from the pharmacokinetic point of view, tapering of budesonide could be problematic. Notably, no expert reported using budesonide as a first‑line induction agent for the acute presentation of AIH during the survey of the IAIHG.76 Therefore, it appears that the role of budesonide in AIH is mainly based on its efficacy as a maintenance agent in patients without cirrhosis experiencing steroid side effects rather than on its efficacy as a first‑line induction agent.76
MMF inhibits purine synthesis and, consequently, DNA synthesis, resulting in an antiproliferative effect. It inhibits only the type II isoform of inosine‑5΄-monophosphate dehydrogenase in activated T- and B‑cells.77 As a result, MMF seems to provide more potent selective immunosuppression with fewer side effects. Up to the present, real‑world prospective observational studies performed by our group and other researchers demonstrated that MMF may be an alternative and secure first‑line induction treatment for AIH patients with a quick, steroid‑sparing effect.28,29,78 Additionally, these studies reported the highest ever published frequencies of biochemical remission maintenance after stopping the treatment, with a median remission duration of 40 months off treatment, which was associated with a significant improvement at the histological level. Furthermore, a recent meta‑analysis found that in comparison with the standard treatment, MMF as a first‑line therapy achieved higher rates of CBR and lower nonresponse rates.79 Based on the abovementioned trials, in 2015 the Hellenic Association for the Study of the Liver recommended (https://www.eemh.gr/images/files/AIH _guidelines_06‑04‑2015.pdf) the use of MMF—as an alternative to azathioprine—as a potential first‑line agent for the induction and maintenance of response, at least in specialized AIH centers.
To validate the previous findings, we recently presented for the first time a face‑to‑face comparison of the efficacy and safety of MMF versus azathioprine using a very strict propensity matching analysis in treatment‑naïve AIH patients who received induction and maintenance therapy for 3 to 5 years.80 Our findings revealed that MMF was significantly associated with higher CBR rates at the end of the study, whereas the patients from the azathioprine group were more likely to discontinue the treatment because of intolerance and / or insufficient response. Furthermore, at the end of the study, the overall treatment efficacy was significantly higher in the MMF group than in the azathioprine group.80
Acute severe autoimmune hepatitis (AS‑AIH) could be occasionally the cause of acute liver failure that is frequently overlooked and undertreated.81-83 The available data indicate that corticosteroids should be introduced as soon as possible in AS‑AIH cases, as they have been shown to be beneficial in 36% to 100% of the patients.81,84-89 However, failure to improve within the first week should result in a liver transplant emergency listing.1,2,82 In a real‑world study by our group, 34 patients with newly‑diagnosed AS‑AIH without signs of hepatic encephalopathy received intravenous corticosteroids (either 1 g of methylprednisolone for 3 consecutive days followed by 1 mg/kg/day of prednisolone intravenously or 1.5 mg/kg/day of prednisolone intravenously from the beginning). None of the patients needed liver transplantation during the follow‑up, while only 1 died due to sepsis. The response rates were attributed to early initiation of high‑dose intravenous corticosteroids and lower Model for End‑stage Liver Disease scores at presentation.88 Moreover, corticosteroids were also found to improve the outcome of acute liver failure–related AIH.90 Recently, predictive factors for early identification of nonresponse to corticosteroids in patients with AS‑AIH have been proposed.91 In this retrospective study, which needs prospective validation, the international normalized ratio (INR) at the time of corticosteroid initiation and the alterations of bilirubin and INR values proved highly predictive of the need for liver transplantation or death. Briefly, the authors developed the SURFASA score which enabled early (within 3 days of the initiation of corticosteroids) identification of the patients who would not respond to treatment and would require referral for liver transplantation.91
Treatment of relapse
After CBR achievement, AIH can relapse either at induction therapy during tapering or withdrawal of corticosteroids, or after lowering the dose of the drugs at maintenance therapy. Relapse is also very frequent after the complete discontinuation of conventional treatments (corticosteroids with or without azathioprine), which typically occurs within 12 months of cessation of immunosuppression.1,2,7 The definition of relapse is not well‑established but it is characterized by the reappearance of symptoms and / or laboratory indices of active disease, namely, ALT levels equal to or greater than 2 to 3 times the upper limit of normal and / or IgG level elevation, which usually occur before the elevation of transaminases.1,2 Liver biopsy is usually not recommended in this setting, as increased ALT levels are highly predictive if other liver disorders that potentially developed concurrently with the disease course (such as viral hepatitis, drug‑induced liver injury, or steatohepatitis) are excluded.
Treatment of relapse episodes is identical to the initial therapy and is also efficient to reinduce CBR. A transient adaption of corticosteroids at doses higher than those received during the relapse episode is usually needed; then the patients can be managed with the usual doses of maintenance medications.1,2,71 Relapse can also be observed because of nonadherence to treatment, which is particularly frequent among teenagers and young adults. In these cases, psychological advice seems important to convince the patients about the benefits of treatment.
Patients with repeated relapse episodes despite compliance and adequate immunosuppression also represent individuals with insufficient response and therefore, they are potential candidates for long‑term, probably permanent, maintenance therapy with second- or third‑line treatments (see below).66,70
Second- and third‑line treatments in autoimmune hepatitis
While the conventional management of AIH is generally agreed upon, there is still ambiguity about how to manage patients with insufficient response or intolerance to azathioprine. According to a recent position statement of the European Reference Network on Hepatological Diseases and the IAIHG, in the case of insufficient response, determination of 6‑thioguanine (6‑TGN), the active metabolite of azathioprine, is recommended.70 The cutoff for an efficient 6‑TGN level was proposed as 220 pmol/8 × 108 red blood cells in a retrospective study from the United Kingdom.92 In this regard, a recent retrospective analysis93 showed that 6‑TGN can improve the rates of biochemical response in patients with fewer adverse events even at lower concentrations (75–220 pmol/8 × 108 red blood cells). Patients with 6‑TGN levels below the cutoff should be evaluated for nonadherence. If noncompliance is excluded, optimization of 6‑TGN levels by increasing azathioprine dosage up to 2 mg/kg/day should be tried before the initiation of third‑line therapies. In insufficiently responsive AIH patients with 6‑TGN levels above the cutoff, a different diagnosis (or one concurrent with the diagnosis of AIH) should be appraised before standard treatment is intensified or third‑line therapies are introduced.70 Unfortunately, however, determination of 6‑TGN levels is not widely available and can only be performed in a few specialist laboratories, making this strategy questionable in everyday clinical practice.
In the case of intolerance, the same position statement70 suggested the use of 6‑mercaptopurine (6‑MP) or MMF as the second‑line therapy before initiating third‑line therapies. However, the use of 6‑MP as second‑line therapy in AIH patients has not been endorsed by the recent AASLD guidelines,3 as this suggestion was mainly based on a small retrospective study (n = 22; CBR, 36%) from a single center.94 In contrast, the AASLD guidelines support the use of tacrolimus or MMF as the second‑line treatment even though this recommendation was based mainly on a retrospective trial with poorly‑defined follow‑up data, performed on a very heterogeneou groups of AIH patients who were treated with various agents including tacrolimus.3,95 Indeed, there are several similar studies which have shown that calcineurin inhibitors (CNIs) are quite effective, but strict monitoring is required due to their small therapeutic window resulting in significant long‑term toxicity in about 25% to 55% of the patients (neurotoxicity, renal injury, hypertension, diabetes, hyperlipidemia, and secondary malignancies).96-99 The final conclusion from these inconsistencies is that we need randomized controlled trials to draw safe general conclusions on the use of 6‑MP and CNIs in AIH patients with insufficient response and / or intolerance to the first‑line treatment.
The most widely investigated second‑line treatment is that with MMF.1-3 According to a systematic review of 15 studies, biochemical and histological remission was observed in 79% and 89% of the patients treated with MMF, respectively, while liver transplantation was required in 11%, and the mortality rate was 7.2%.96 Another meta‑analysis found that 58% of the patients responded to MMF with low discontinuation rates, while the response was higher in intolerant patients (82% vs 32% in nonresponders).100 The Australian Liver Association Clinical Research Network recently confirmed that MMF is an excellent option for the patients with intolerance of or insufficient response to the first‑line treatment, with responders being older at MMF onset or with lower IgG and INR values at baseline.100
As in other autoimmune and autoinflammatory conditions, B‑cell depletion by using rituximab, a monoclonal anti‑CD20 antibody, is a promising option for nonresponders to standard therapies.1-3,101 The IAIHG published the results of a study on 22 patients who received rituximab in 3 European centers and were followed for up to 24 months post infusion.102 Rituximab was well tolerated, aminotransferases and albumin levels improved significantly and remained stable, while the dose of prednisolone was reduced in 62% of the patients and 71% were free of AIH flares. However, precise rates of CBR on treatment were not reported.
In the context of B‑cell depletion therapies, the use of belimumab, a human monoclonal antibody that inhibits soluble B‑cell activation factor (BAFF), appears appealing in the treatment of refractory AIH patients. BAFF is important for the development and differentiation of B‑lymphocytes but also of activated T‑cells. We recently reported on 2 AIH patients with compensated cirrhosis in whom standard treatments had failed, and who achieved CBR to third‑line belimumab add‑on therapy, while simultaneously achieving histological remission of the disease as attested by serial LSMs by TE and liver biopsy.103 Theoretically, anti‑BAFF therapy can be followed by anti‑CD20 therapies to achieve depletion of B‑memory cells mobilized from lymphoid tissues by anti‑BAFF.3
Finally, the use of tumor necrosis factor α (TNF-α) inhibitors could have a pathophysiological basis for AIH management given that the TNF pathway has been linked to the pathogenesis of the disease. Weiller‑Norman et al104 published their single‑center experience with infliximab on 11 difficult‑to‑treat adult patients, revealing that while half of the patients achieved biochemical response, two‑thirds developed infectious complications.104 However, an increasing number of autoimmune phenomena linked to anti–TNF-α agents have come to light in recent years. Infliximab is a known cause of idiosyncratic or indirect drug‑induced hepatitis and even drug‑induced AIH.105-107 Taken together, TNF-α blocking agents seem to represent a “2‑edged sword” management in AIH. Therefore, the recent AASLD guidelines consider these drugs as having a “definite association” with AIH development.3 In other words, the “dark side” of anti–TNF-α therapy includes induction of autoimmunity and vulnerability to infection, and therefore, we strongly believe that anti–TNF-α–based therapies for AIH should be considered only if other treatment regimens with lower risks of side effects have failed.
Conclusions
Diagnosis of AIH remains challenging, since no single pathognomonic test exists, and the disease presentation is characterized by high heterogeneity at clinical, laboratory, histological, and serological levels. As a result, regardless of ethnicity, sex, or age, it is critical to consider AIH in differential diagnosis of all individuals with transaminasemia of any severity. The precise guidelines for liver autoimmune serology,1,2,7,8 the update on the simplified criteria for AIH,55 the previous35 and recent recommendations for the assessment of the histological criteria of AIH,46 and the systematic review of the response criteria and end points of AIH by the IAIHG66 all aim to facilitate a prompt diagnosis and timely treatment, which is mandatory and life‑saving in patients with active disease. However, the conventional treatment with predniso(lo)ne and azathioprine is far from ideal due to the very high relapse rates after treatment cessation and increased rates of adverse events. Alternative therapies with 6‑MP or MMF, the latter even considered a first‑line therapy in expert centers, seem promising. CNIs and treatment with biologic agents could be beneficial as third‑line treatment options in difficult‑to‑treat patients after careful consideration of the pros and cons in an individualized manner.
A small group of patients with AIH not responding to the abovementioned treatment strategies will need liver transplantation due to the development of decompensated cirrhosis with or without hepatocellular carcinoma, or because of acute severe AIH resulting in acute liver failure (2%–5% of transplant recipients in Europe and the United States, with recurrence rates of 8%–12% and 36%–65% at 1 and 5 years after liver transplantation, respectively).1-3,7,25 However, these specific issues are beyond the scope of this review on the advances in diagnosis and management of AIH.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: autoimmune hepatitis. J Hepatol. 2015; 63: 971‑1004. | Crossref
- Dalekos GN, Koskinas J, Papatheodoridis GV. Hellenic Association for the Study of the Liver Clinical Practice Guidelines: autoimmune hepatitis. Ann Gastroenterol. 2019; 32: 1‑23. | Crossref
- Mack CL, Adams D, Assis DN, et al. Diagnosis and management of autoimmune hepatitis in adults and children: 2019 practice guidance and guidelines from the American Association for the Study of Liver Diseases. Hepatology. 2020; 72: 671‑722. | Crossref
- Czaja AJ. Global disparities and their implications in the occurrence and outcome of autoimmune hepatitis. Dig Dis Sci. 2017; 62: 2277‑2292. | Crossref
- Delgado JS, Vodonos A, Malnick S, et al. Autoimmune hepatitis in southern Israel: a 15‑year multicenter study. J Dig Dis. 2013; 14: 611‑618. | Crossref
ARTICLE INFORMATION