Sarcoidosis is a generalized granulomatous disease that may involve critical organs. The course of the disease can be highly variable. The clinical picture is often nonspecific, which creates diagnostic problems and makes it difficult to choose an appropriate treatment.1,2
A 39‑year‑old man with a 10‑year history of lung sarcoidosis was admitted to the cardiology department due to chest pain. The patient did not take any medications on a permanent basis. He had a history of joint pain, palpitations, and an episode of presyncope. Laboratory workup showed elevated levels of troponins. Electrocardiography (ECG) revealed dynamic changes in the T wave in leads V3–V6. Transthoracic echocardiography recorded abnormalities of segmental contractility of the left ventricle (LV), normal dimensions of the heart chambers, hypokinesis of the basal inferior wall segment, and the distal interventricular septum (IVS) segment with borderline global left ventricular systolic function (left ventricular ejection fraction [LVEF], 50%) and impaired LV global longitudinal strain (LVGLS, 13.3%) and segmental longitudinal strain (Figure 1A). The clinical presentation indicated non–ST‑segment elevation myocardial infarction and an urgent coronary angiography was performed. The procedure did not show any significant abnormalities; therefore, the diagnostic workup was extended. Control troponin T levels remained elevated at 0.053 ng/ml (reference range <0.014 ng/ml). C‑reactive protein levels were within the reference range (<5 mg/l). During the hospitalization no hypercalcemia or hypercalciuria were found. Due to the suspicion of myocarditis or an active form of cardiac sarcoidosis, additional tests were done. Chest X‑ray findings were unremarkable.
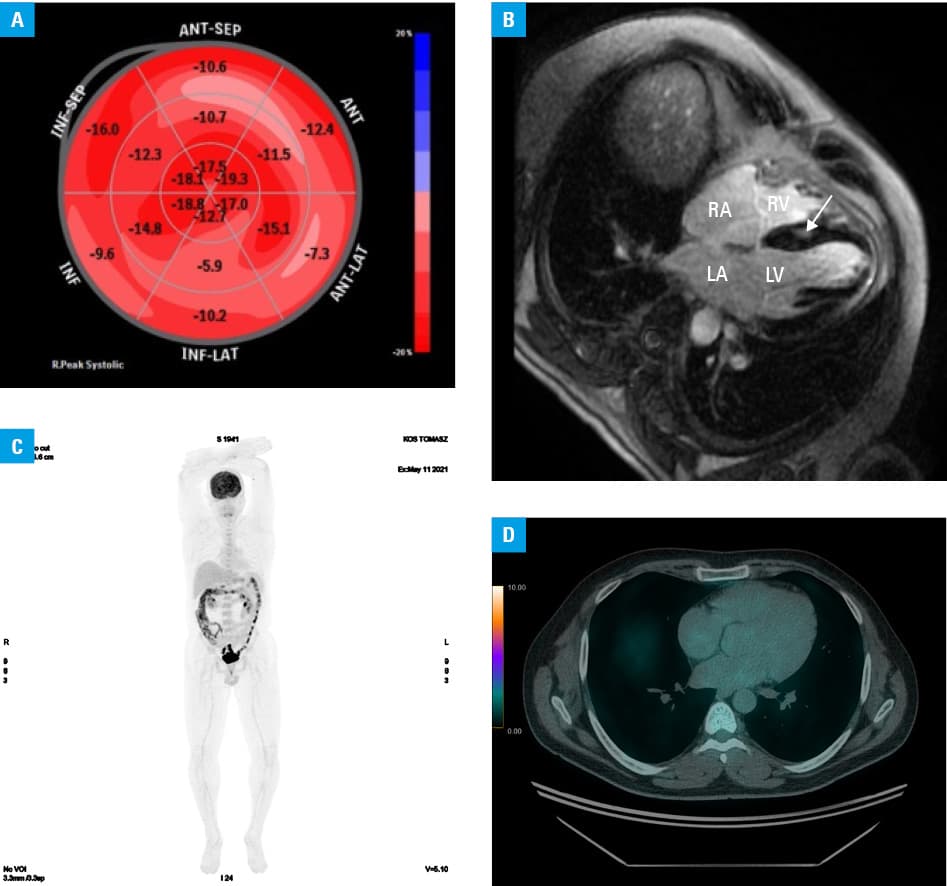
A 24‑hour ECG recording showed sinus rhythm with an average heart rate of 52 bpm without arrhythmias, conduction disturbances, or pathological pauses. Abdominal ultrasound revealed no abnormalities, whereas cardiovascular magnetic resonance (CMR) showed LV hypertrophy, focal intramuscular enhancement in the medial segment of the IVS, subepicardial late gadolinium enhancement in most LV and right ventricular (RV) inferior wall segments, LVEF of 48%, and RV ejection fraction of 66%. The image did not meet the criteria for arrhythmogenic RV cardiomyopathy (Figure 1B). Despite elevated levels of myocardial damage markers, positron emission tomography (PET) ruled out the presence of active cardiac sarcoidosis (Figure 1C and 1D). The patient had no indications for steroids or electrotherapy. This created a dilemma regarding the choice of further treatment.
One month after discharge, follow‑up laboratory investigations showed hypercalcemia and hypercalciuria, which were the basis for the implementation of steroid treatment. It led to a temporary regression of symptoms and an improvement in the LV systolic function (LVEF, 54%; LVGLS, 16.1%; hyperkinesis of the apical and periapical segments).
The described clinical case shows that despite performing all the necessary diagnostic tests for active sarcoidosis, there are still many uncertainties as to the choice of further treatment.3,4 The dynamic clinical picture, elevated troponin levels, as well as variability in echocardiography and CMR imaging indicated an active form of sarcoidosis in the myocardium, which, however, was not confirmed by PET. Therefore, despite so many additional tests, there were still many doubts as to the further therapeutic procedure and the presence of indications for steroid treatment.
- Llanos O, Hamzeh N. Sarcoidosis. Med Clin North Am. 2019; 103: 527‑534. | Crossref
- Sève P, Pacheco Y, Durupt F, et al. Sarcoidosis: a clinical overview from symptoms to diagnosis. Cells. 2021; 10: 766. | Crossref
- Katakami N. Hypercalcemia in sarcoidosis [in Japanese]. Nihon Rinsho. 2002; 60: 1778‑1784.
- Tan JL, Fong HK, Birati EY, et al. Cardiac sarcoidosis. Am J Cardiol. 2019; 123: 513‑522. | Crossref
ARTICLE INFORMATION