Giant intracerebral schwannoma of the skull base misinterpreted as a macroprolactinoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Giant intracerebral schwannoma of the skull base misinterpreted as a macroprolactinoma
Intracranial schwannomas are benign tumors, accounting for between 6% and 8% of all intracranial tumors, with the majority arising from the vestibular division of the vestibulocochlear cranial nerve, whereas intracerebral schwannomas account for less than 1% of intracranial schwannomas.1 Most schwannomas are derived from cranial nerves, except for the optic and olfactory nerves, which are devoid of sheaths containing Schwann cells. The characteristic features of intracranial schwannomas are slow growth as well as well‑limited margins, displacement of local structures, and expansion of osseous foramina on imaging.2
We present a case of a 41‑year‑old woman with no family history of the disease described (approximately 18% of solitary schwannomas occur in patients with neurofibromatosis type 23). The symptoms included dizziness, numbness of the right upper limb, visual acuity disturbances in the right eye, recurrent miscarriage, galactorrhea (because of an elevated prolactin concentration of 165 µg/l [reference range, 5–25 µg/l], temporarily treated with bromocriptine). The visual field examination showed left‑sided upper quadrant amblyopia. On neurological examination, the pupils were equal in size, with correct response to light, no cranial nerve deficits were found, and the strength and muscle tone of the limbs were normal. Preoperative magnetic resonance imaging (MRI) of the brain revealed a giant cystic lesion on the left side of the middle cranial fossa with a heterogeneous contrast enhancement of approximately 6 × 6 × 6.5 cm. The lesion infiltrated the left cavernous sinus, the sella turcica, the suprasellar region, the left posterior cranial fossa, and the left pterygopalatine fossa, and there was a slight peritumor edema in the left temporal lobe (Figure 1A–1D). Computed tomography (CT) of the head showed involvement of the skull base with bone erosion (Figure 1E and 1F). The patient was referred for surgical removal of the tumor. Left fronto‑parietal‑temporal craniotomy was performed with total tumor resection. Pathological findings were consistent with a diagnosis of conventional schwannoma, which showed typical Antoni A and Antoni B areas (Figure 1G). Postoperative CT confirmed that the tumor was completely resected. At the 6‑month follow‑up the patient showed a slight improvement in visual acuity in the left eye and no neurological symptoms.
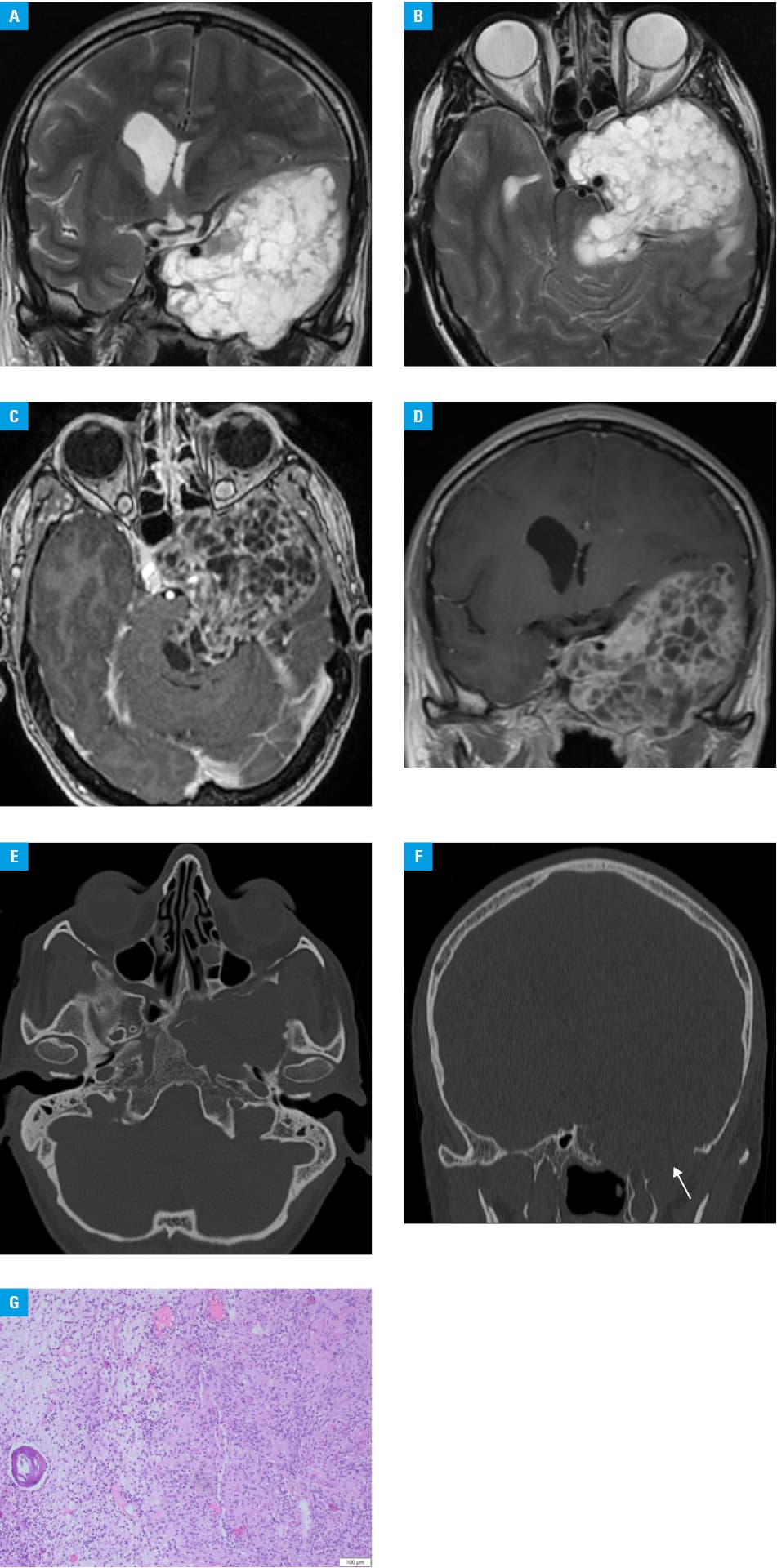
We present an unusual case of a giant intracerebral schwannoma. Due to atypical features on MRI and unspecific clinical symptoms on examination (no cranial nerve palsy), the correct diagnosis was missed preoperatively. Based on the MRI results, showing a cystic‑solid tumor with involvement of the left cavernous sinus, the sella turcica, as well as the suprasellar region, a proliferative lesion of the pituitary macroadenoma or craniopharyngioma was suspected. Because of bone erosion and typical location at the skull base (off the midline), chondrosarcoma of the sphenoid wing was also considered, while a schwannoma was not taken into consideration preoperatively.4 Approximately 90% of intracranial schwannomas arise in cerebellopontine angles in relation to the vestibular nerve.5 The presented case is extremely rare and could pose a diagnostic problem for specialists.
- Yufei G, Zhigang Q, Dongyuan L, et al. Intracerebral schwannoma: a case report and literature review. Oncol Lett. 2018; 16: 2501‑2510.
- Skolnik AD, Loevner LA, Sampathu DM, et al. Cranial nerve schwannomas: diagnostic imaging approach. Radiographics. 2016; 36: 1463‑1477. | Crossref
- Kahraman G, Celtikci P, Karasu S. Radiological screening for hereditary cancer predisposition syndromes. In: Osman O, Selman U, Rifat L, eds. Prophylactic Surgery. Springer Nature Switzerland AG; 2021: 497‑512. | Crossref
- Louis DN, Perry A, Wesseling P, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Onc. 2021; 21: 1231‑1251. | Crossref
- Takeuchi Y, Arakawa Y, Yokoo H, et al. Intra‑cerebellar schwannoma with various degenerative changes: a case report and a systematic review. BMC Neurol. 2022; 22: 66. | Crossref
ARTICLE INFORMATION