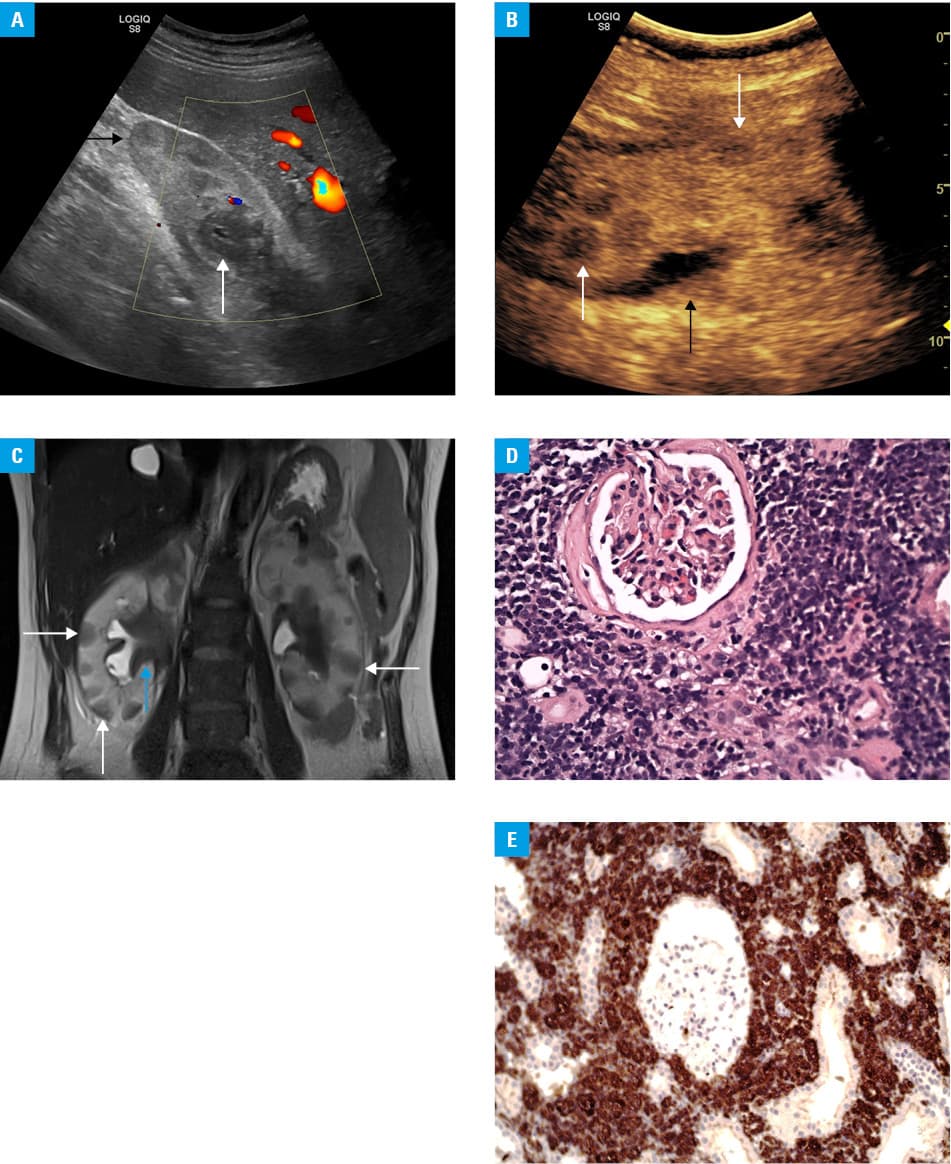
A 43‑year‑old woman with T‑cell acute lymphoblastic leukemia (T‑ALL) was treated with intensive chemotherapy according to protocols for young adults with T‑ALL (Supplementary material, Table S1) followed by hematopoietic stem cell transplantation (HSCT) performed 5 months after the initial diagnosis, and then with cyclosporine A and steroids because of graft versus host disease with hematological remission. Her kidney function was normal at all times (estimated glomerular filtration rate [eGFR] of about 80 ml/min/1.73 m2). Twenty months after HSCT she was admitted to a nephrology department due to acute kidney injury (AKI) with a serum creatinine level of 3.5 mg/dl (reference range, 0.72–1.18 mg/dl) and eGFR of 15 ml/min/1.73 m2, with a trace of protein in urine and normal urine sediment. Diuresis was normal and the patient had no history of hypertension. Abdominal ultrasonography showed slight enlargement of the kidneys with reduced corticomedullary differentiation, multiple solid, focal, hyperechoic lesions in the kidney parenchyma, slight enlargement of the renal pelvises, and thickened mucosa of the ureters (Figure 1A). Contrast‑enhanced ultrasonography confirmed the presence of the abovementioned lesions (Figure 1B). Doppler ultrasonography showed low‑resistance flow at the corticomedullary border. Magnetic resonance imaging revealed numerous solid, focal, T2‑hypointense lesions in the kidney parenchyma. Multiple normal‑size retroperitoneal lymph nodes around the kidneys were observed alongside with a slight enlargement of the liver and signs of inflammation in the bile ducts (Figure 1C). Kidney biopsy revealed infiltration with T‑cell lineage lymphoblasts corresponding with the previous diagnosis of T‑ALL (Figure 1D and 1E). The patient received steroids with cyclophosphamide as the induction of intensive chemotherapy, which led to a rapid improvement of the kidney function and allowed for the administration of further chemotherapy. Unfortunately, she died due to COVID‑19 complications 6 months later.
T‑ALL is an immature lymphoid tumor that preferentially localizes in the bone marrow or lymphoid organs, particularly in the mediastinal lymph nodes and the central nervous system. Kidney injury in T‑ALL encompasses a broad etiological spectrum, such as prerenal AKI, acute tubular necrosis, tumor lysis syndrome, renovascular diseases, obstruction, glomerulonephritis, and electrolyte or acid‑base disturbances. It can also be a consequence of nephrotoxicity. Parenchymal infiltration by the tumor cells is rare, with renal failure due to this cause being even rarer.1
There are only single case reports of kidney infiltration in ALL as a primary manifestation of the disease and as a clinical manifestation of relapse in patients after bone marrow transplantation.2,3 In T‑ALL, up to 70% of adults receiving intensive treatment achieve long‑term survival; however, the prognosis after relapse is still poor (a 5‑year survival rate of 20%).4 A quick and conclusive diagnosis of relapse and identification of the cause of the kidney function impairment are essential for the implementation of appropriate therapy. We presented a case of a patient with a history of HSCT due to T‑ALL, without any signs of disease relapse in peripheral blood, and with AKI as a consequence of parenchymal infiltration by ALL, which was diagnosed based on radiological images and confirmed by kidney biopsy findings.
- Luciano RL, Brewster UC. Kidney involvement in leukemia and lymphoma. Adv Chronic Kidney Dis. 2014; 21: 27‑35. | Crossref
- Saito B, Nakashima H, Ariizumi H, et al. Bilateral renal infiltration of acute lymphoblastic leukemia cells at relapse after allogeneic stem cell transplantation. Rinsho Ketsueki. 2011; 52: 1882‑1887.
- Tamura Y, Sumiyoshi R, Yamamoto T, et al. Bilateral nephromegaly due to direct leukemic cell invasion in the initial and relapse phases of T‑cell acute lymphoblastic leukaemia: a case report. Medicine (Baltimore). 2021; 100: e28391. | Crossref
- Grunenberg A, Sala E, Kapp‑Schwoerer S, Viardot A. Pharmacotherapeutic management of T‑cell acute lymphoblastic leukemia in adults: an update of the literature. Expert Opin Pharmacother. 2022; 23: 561‑571. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION