Isolated urachal tuberculosis: a rare culprit of abdominal pain and frequent urination



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Isolated urachal tuberculosis: a rare culprit of abdominal pain and frequent urination
A 55‑year‑old diabetic woman presented to our hospital with a 6‑week history of progressively worsening lower abdominal pain. Before her visit to our hospital, she was empirically treated with nitrofurantoin enteric‑coated Tablets for 7 days, prescribed by her primary care physician due to frequent urination apparently caused by urinary tract infection. However, this treatment was not effective. The patient denied any fever, chronic cough, night sweats, or weight loss. She was diagnosed with type 2 diabetes 3 years ago and was put on hypoglycemic therapy, but did not adhere to the prescribed medication. The patient had no history of tuberculosis (TB) infection or contact with TB patients. Abdominal examination revealed a tender mass with indistinct margins in the infraumbilical area.
Laboratory workup showed mild neutrophilia with left shift, but her leukocyte count was normal. Glycated hemoglobin was 7.56% (reference range [RR], 3.90–6.10/μl). Urinalysis revealed microhematuria of 20/µl (RR, 0–11/µl) and leukocyturia of 145/µl (RR, 0–9/µl), but no microorganisms were identified in a 72‑hour culture. The tuberculin skin test (TST) and T‑SPOT.TB tests were positive. A thoracic computed tomography (CT) scan did not confirm any pulmonary or nodal disease. The contrast‑enhanced CT image showed a large granulomatous multilocular lesion with irregular thickening of the wall, heterogeneous enhancement, and adjacent fat stranding (Figure 1A and 1B), all of which were consistent with the infected urachal remnant. However, due to the ineffective use of general antibiotics and positive TST and T‑SPOT.TB tests, we considered the possibility of urachal tuberculosis.
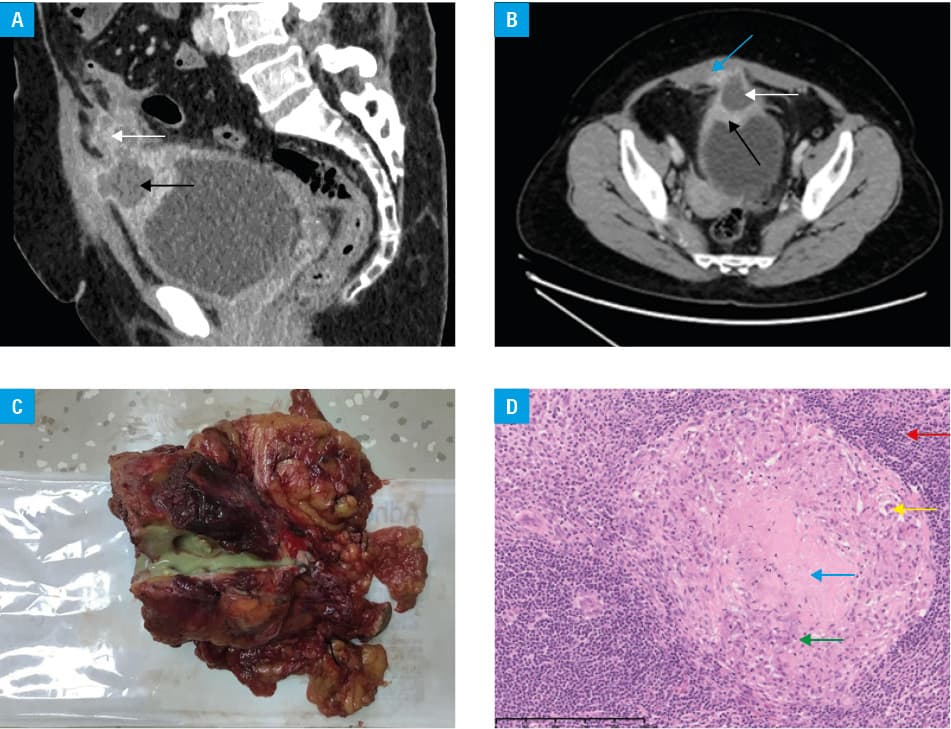
Laparotomy was performed to remove the infiltrative urachal mass together with adjacent parts of the bladder, rectus abdominis muscle, and greater omentum. Gross examination showed a cystic solid mass containing creamy‑yellow fluid and caseous necrotic material (Figure 1C). Pathological examination revealed granulomas with caseous necrosis and Langhans giant cells (Figure 1D), suggesting tuberculosis. The symptoms gradually resolved after the surgery. Given the lack of evidence for pulmonary or other tuberculosis, a diagnosis of isolated urachal tuberculosis infiltrating the bladder, greater omentum, and rectus abdominis was made. The patient was put on a 2‑month initial intensive phase of antituberculosis treatment (pyrazinamide 750 mg, ethambutol 500 mg, rifampicin 600 mg, and isoniazid 300 mg once daily), followed by 4 months of a maintenance phase (isoniazid 300 mg and rifampicin 600 mg once daily). During a 6‑month follow‑up, the patient was asymptomatic and had fully recovered.
Infected urachal remnant is the most common complication of urachal anomalies. The most common cause of infection is Staphylococcus aureus, and Mycobacterium tuberculosis has been reported in rare cases.1,2 We speculated that urachal tuberculosis in our case was due to reactivation of latent TB foci in the immunocompromised state of diabetes mellitus.3 The diagnosis of urachal tuberculosis is often challenging due to its nonspecific symptoms. Moreover, general antibiotic therapy is ineffective. Its CT / magnetic resonance imaging features include irregular wall thickening, heterogeneous enhancement, and adjacent fat stranding that indicate infected urachal remnant.1 Infected urachal remnant is frequently misdiagnosed as malignancy. Hematuria and calcification can be used as features of urachal carcinoma to differentiate it from infected urachal lesions.4 In individuals with recurrent or intractable urinary tract infections, TB should be suspected. Mycobacterial culture of the body fluid or biopsy specimens are considered the gold standard methods for the diagnosis of urachal TB.5 Complete resection of TB lesions followed by adequate postoperative antituberculosis treatment are recommended to prevent recurrent infection.2
- Buddha S, Menias CO, Katabathina VS. Imaging of urachal anomalies. Abdom Radiol (NY). 2019; 44: 3978‑3989. | Crossref
- Ou L, Luo J, Wei Z, et al. Urachal tuberculosis with invasion of the bladder wall: a case report and literature review. Actas Urol Esp (Engl Ed). 2022; 46: 1‑3. | Crossref
- Lee MR, Huang YP, Kuo YT, et al. Diabetes mellitus and latent tuberculosis infection: a systematic review and metaanalysis. Clin Infect Dis. 2017; 64: 719‑727.
- Li S, Meng X, Liang P, et al. Clinical and radiological features of urachal carcinoma and infection. Front Oncol. 2021; 11: 702116. | Crossref
- Zhou XX, Liu YL, Zhai K, et al. Body fluid interferon-γ release assay for diagnosis of extrapulmonary tuberculosis in adults: a systematic review and meta‑analysis. Sci Rep. 2015; 5: 15284. | Crossref
ARTICLE INFORMATION