Peripartum cardiomyopathy or acute myocardial infarction: how to face the challenge?



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Peripartum cardiomyopathy or acute myocardial infarction: how to face the challenge?
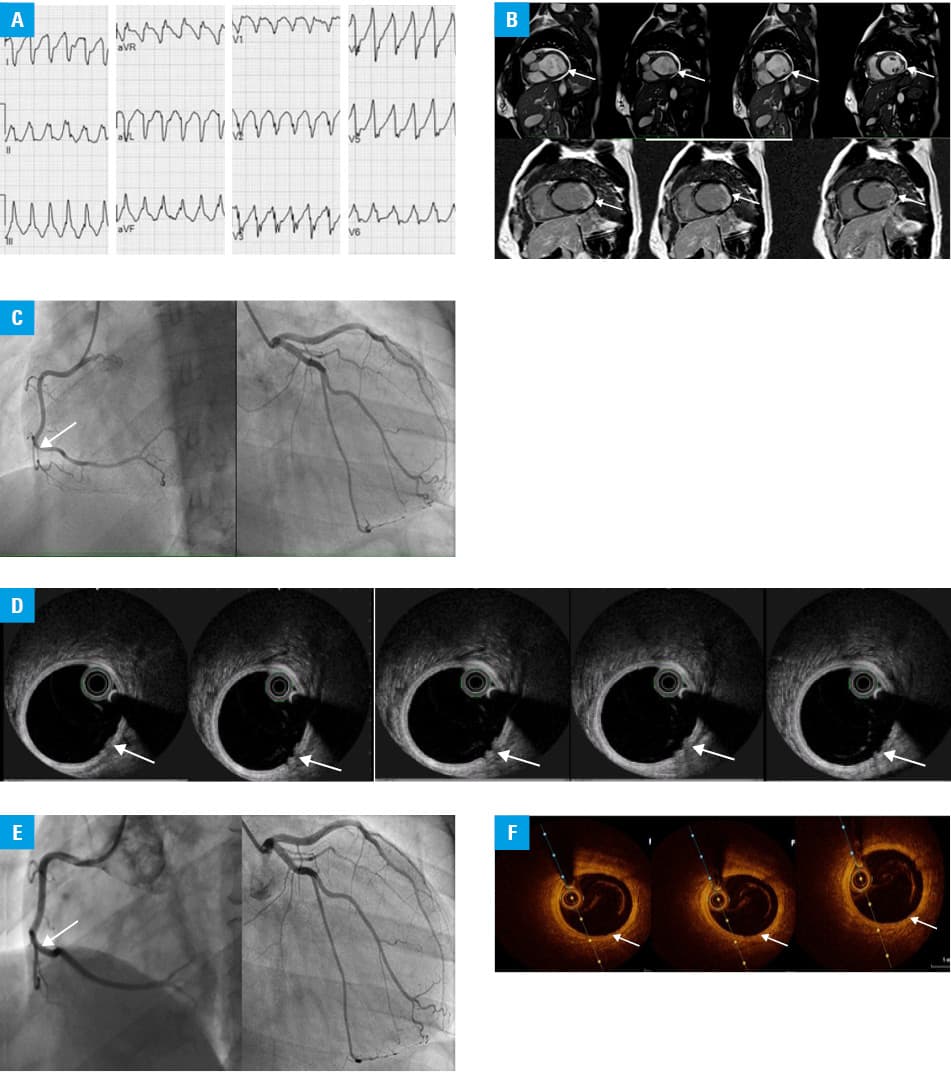
A 36‑year‑old woman developed sudden‑onset chest tightness, tachycardia, and tachypnea 2 hours after natural childbirth (healthy, first child, uneventful, vaginal delivery at 39 weeks of gestation). The patient’s medical history was unremarkable. Initial examination revealed a heart rate (HR) of 140 bpm, blood pressure (BP) 95/60 mm Hg, respiratory rate (RR) 28/min, and elevated levels of troponin (2.3 ng/ml; reference value [RV] <0.05 ng/ml) and N‑terminal pro–B‑type natriuretic peptide (986 pg/ml; RV <125 pg/ml). Electrocardiography recorded monomorphic ventricular tachycardia refractory to intravenous amiodarone therapy (Figure 1A). Effective electrical cardioversion was promptly performed, and the patient was transferred to our cardiology department. Initial transthoracic echocardiography (TTE) showed reduced left ventricular ejection fraction (LVEF, 20%). Computed tomography imaging ruled out pulmonary embolism and significant atherosclerotic plaques in coronary arteries. Due to a suspicion of peripartum cardiomyopathy (PPCM), bromocriptine, oral heart failure therapy (renin‑angiotensin system inhibitor, b‑blocker, mineralocorticoid receptor antagonist), and anticoagulation were initiated. The repeated TTE showed an increase in LVEF to 35% within the next few days and the presence of segmental wall motion abnormalities akinesis of the basal and middle segments of the lateral and inferolateral wall and moderate functional mitral valve regurgitation. Cardiac magnetic resonance demonstrated regional akinesia limited to the corresponding area of TTE with a delayed subendocardial (>70% wall thickness) contrast enhancement, and globally reduced systolic function (LV end‑diastolic volume 251 ml/m²; LVEF, 40%) (Figure 1B). A coronary angiogram (CA) showed nonobstructed coronary arteries. Subsequent intracoronary optical coherence tomography (OCT) showed the presence of a thrombus in the medial segment of the right coronary artery (RCA), without significant vessel lumen occlusion and overt plaque erosion (Figure 1C and 1D). Dual antiplatelet therapy (DAPT) was started with aspirin 75 mg/day and clopidogrel 75 mg/day, while anticoagulation was discontinued. The subsequent testing for thrombophilia and autoimmune disorders was negative. Control TTE revealed an improvement of LVEF to 45%, and the patient was discharged in a good condition on the 5th day. During a follow‑up visit, 3 months later, TTE showed normalization of the LV systolic function (LVEF, 55%) without wall motion abnormalities, while control CA along with OCT of the RCA visualized the residual thrombus in the medial part of the vessel (Figure 1E and 1F). The DAPT continuation was recommended up to 12 months after myocardial infarction (MI).
Ventricular arrhythmia and acute heart failure in the perilabor period can be the manifestation of PPCM, and pregnancy‑related MI (PMI) (Supplementary material, Table S1).1,2 The arrhythmic presentation was reported in 19% of women with PPCM.2,3 In our case, plaque erosion was a cause of PMI and manifested itself as ventricular tachycardia. PMI is a rare entity that mostly presents with ST‑segment elevation MI. The etiology of PMI includes coronary artery dissection, and less often atherosclerosis, thrombosis, or coronary vasospasm.4 Our patient had no classic risk factors. Maternal age older than 35 years is one of the most important risk factors for PMI.5 This case underlines that physicians must be vigilant in considering a broad differential diagnosis in maternal complications of the peripartum and be prepared to face these conditions.
- Merlo AC, Rosa GM, Porto I. Pregnancy‑related acute myocardial infarction: a review of the recent literature. Clin Res Cardiol. 2022; 11: 723‑731. | Crossref
- Bauersachs J, König T, van der Meer P, et al. Pathophysiology, diagnosis, and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail. 2019; 21: 827‑843. | Crossref
- Ciepłucha W, Ciepłucha A, Walgamage T, et al. Peripartum cardiomyopathy ‑ challenges of diagnosis and management. Stay alert and implement BOARD treatment. Kardiol Pol. 2022; 80: 715‑716. | Crossref
- Elkayam U, Jalnapurkar S, Barakkat MN, et al. Pregnancy‑associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation. 2014; 129: 1695‑1702. | Crossref
- Lameijer H, Kampman MA, Oudijk MA, Pieper PG. Ischaemic heart disease during pregnancy or post‑partum: systematic review and case series. Neth Heart J. 2015; 23: 249‑257. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION