IgG4-related disease: sight-threatening orbital disease, spectacular improvement after rituximab therapy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
IgG4-related disease: sight-threatening orbital disease, spectacular improvement after rituximab therapy
IgG4‑related disease (IgG4‑RD) is a multiorgan fibroinflammatory condition, characterized by storiform fibrosis, pseudotumors, obliterative phlebitis, and organ damage, including orbitopathy in IgG4‑related ophthalmic disease (IgG4‑ROD).1 IgG4‑RD diagnostic criteria include diffused swelling or masses in single or multiple organs, elevation of serum IgG4 level (≥ 135 mg/dl; reference range [RR], 5–134 mg/dl), histopathologic examination showing lymphoplasmacytic infiltrations and fibrosis, infiltration of IgG4+ plasma cells with the ratio of IgG4+/IgG+ cells above 40% and above 10 IgG4+ plasma cells / high powered field of a biopsy sample.2,3 Glucocorticosteroids alone or in combination with immunosuppressive therapy remain the first‑line treatment of IgG4‑RD.4 Severe cases of IgG4‑ROD require additional therapy, such as orbital decompression, which not always provides satisfactory results. Therefore, sight‑threatening IgG4‑ROD, especially with keratopathy and / or dysthyroid optic neuropathy (DON), requires off‑label treatment with anti‑CD20 monoclonal antibody, rituximab (RTX).5
A 30‑year‑old man, a smoker, was admitted to the Department of Internal Medicine and Endocrinology in 2012 due to painless bilateral orbitopathy with proptosis, eyelid retraction, and restricted eye motility. His medical history revealed ST‑segment elevation myocardial infarction (MI) treated with percutaneous transluminal coronary angioplasty of the left anterior descending coronary artery, with subsequent heart failure, unilateral renal agenesis, and Hashimoto thyroiditis treated with levothyroxine.
Considering the patient’s thyroid disease and physical examination, Graves’ orbitopathy was first diagnosed. Treatment with intravenous methylprednisolone (ivMP) was introduced. Despite transient improvement following several ivMP courses (cumulative dose, 8 g), the patient experienced further deterioration with sight‑threatening bilateral keratopathy and DON (best corrected visual acuity [BCVA]: right and left eye, 0.8 and 0.7, respectively; RR, 1.0; apical crowding and optic nerve stretching on magnetic resonance imaging), marked proptosis (right and left eye, 29 mm and 32 mm, respectively; RR, <20 mm), and lagophthalmos (right and left eye, 6 mm and 7 mm, respectively; RR, 0 mm) (Figure 1A–1D). The patient received high‑dose ivMP therapy (1 g for 3 consecutive days). Orbital decompression of the lateral and inferior wall with removal of fat was performed in 2014, but with temporary improvement.
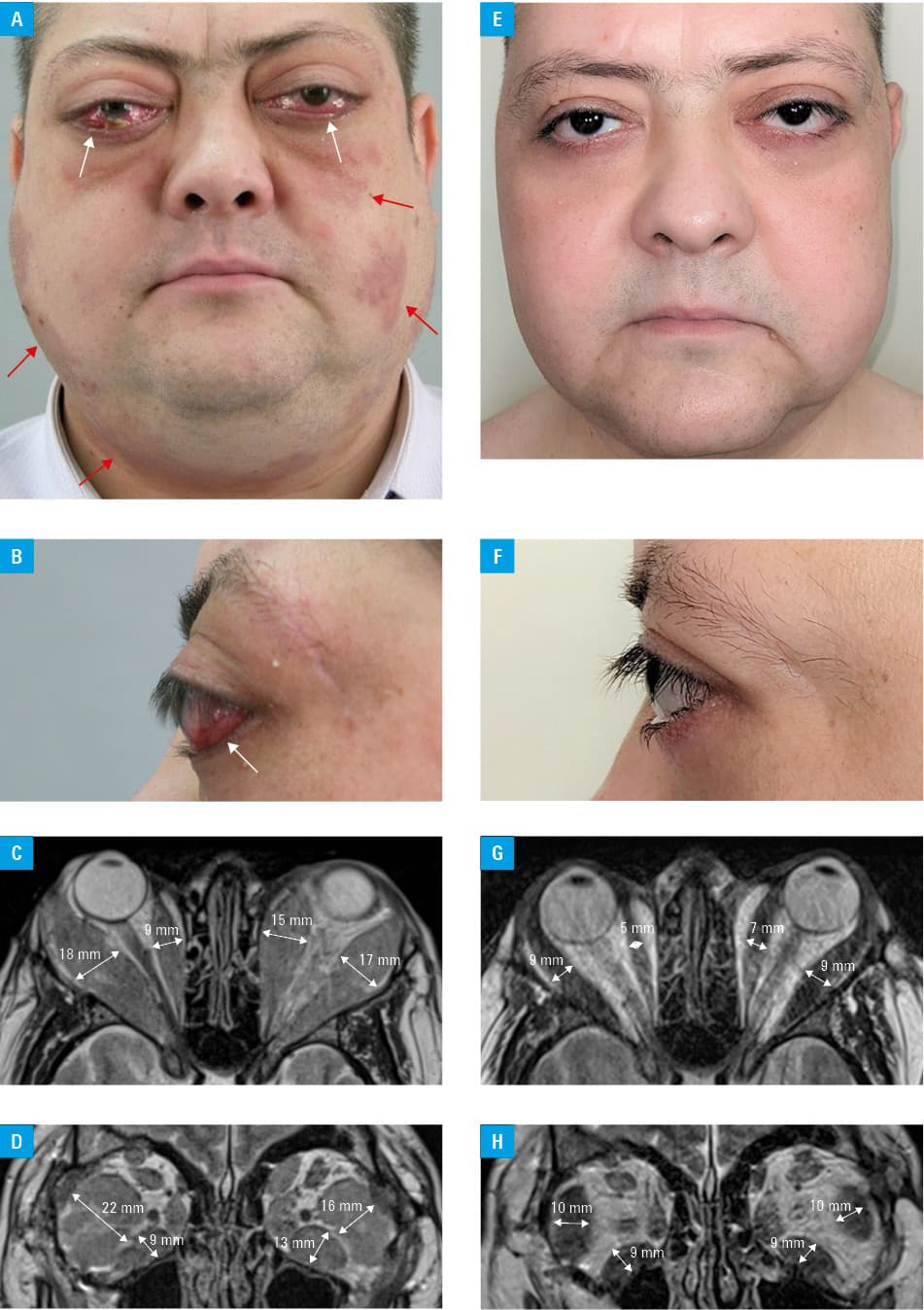
In 2014, the patient began to develop additional signs, that is, cervical, axillary, mediastinal, and pelvic lymphadenopathy (as evidenced by positron emission tomography and computed tomography), enlarged salivary glands, hepatomegaly and skin lesions (Figure 1A) (Supplementary material, Tables S1–S3). Laboratory tests showed elevated serum IgG4 concentrations (770 mg/dl). Histopathologic examination of the skin tissue and orbital fat biopsy (positive for IgG4+ plasma cells) demonstrated lymphoplasmacytic infiltrations rich in IgG4+ plasma cells with fibrosis. Diagnosis of IgG4‑RD was made in 2015. After consulting National Institute of Geriatrics, Rheumatology and Rehabilitation (NIGRiR), treatment with RTX was introduced (2 × 1000 mg at a 2‑week interval) in 2016. Stabilization of IgG4‑RD, including IgG4‑ROD, was achieved with subsequent reduction in the disease activity and proptosis, with resolution of DON, lagophthalmos, lymphadenopathy, and skin lesions.
Following 3 years of sustained improvement, the patient experienced relapse of severe IgG4‑ROD refractory to further ivMP pulses (cumulative dose, 16.5 g). He was referred to NIGRiR, where methotrexate was introduced (25 mg/week, subcutaneously) with poor response. Due to recurrence of sight‑threatening orbitopathy (BCVA, right and left eye, 0.8 and 0.5, respectively; lagophthalmos, 9 mm in both eyes), another course of RTX (2 × 1000 mg at a 2‑week interval; 2 × 1000 mg at a 2‑week interval after 6 months) was applied after approval of Bioethics Committee (KBT‑2/5/2020), with subsequent improvement.
Currently, 2 years following RTX therapy, the patient is in a stable condition, with inactive orbitopathy (BCVA, 1.0; lagophthalmos, 0 mm; proptosis in right and left eye, 25 mm), and correct eye motility (Figure 1E–1H). Severe MI with subsequent exacerbation of the ejection fraction when the patient was 28 years old was suspected to be a cardiovascular manifestation of IgG4‑RD. The patient was referred for further cardiac diagnostics.
In conclusion, spectacular improvement of IgG4‑ROD refractory to the combination therapy with glucocorticosteroids, orbital decompression, and immunosuppressants was achieved following treatment with RTX.
- Zen Y, Nakanuma Y. Pathogenesis of IgG4‑related disease. Curr Opin Rheumatol. 2011; 23: 114‑118. | Crossref
- Umehara H, Okazaki K, Masaki Y, et al. Comprehensive diagnostic criteria for IgG4‑related disease (IgG4‑RD), 2011. Mod Rheumatol. 2012; 22: 21‑30. | Crossref
- Wallace ZS, Naden RP, Chari S, et al. The 2019 American College of Rheumatology / European League Against Rheumatism classification criteria for IgG4‑related disease. Arthritis Rheumatol (Hoboken, NJ). 2020; 72: 7‑19.
- Khosroshahi A, Wallace ZS, Crowe JL, et al. International consensus guidance statement on the management and treatment of IgG4‑related disease. Arthritis Rheumatol (Hoboken, NJ). 2015; 67: 1688‑1699. | Crossref
- Zhang W, Stone JH. Management of IgG4‑related disease. Lancet Rheumatol. 2019; 1: 55‑65. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION