Lemierre's syndrome: should neck imaging be performed in all young patients with cavitating pneumonia?



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Lemierre's syndrome: should neck imaging be performed in all young patients with cavitating pneumonia?
Lemierre’s syndrome (LS) is typically characterized by internal jugular vein (IJV) thrombophlebitis and anaerobic bacteremia in the context of an oropharyngeal infection. It was first described in 1936 by Andre Lemierre, who published a case series analyzing 20 patients, all of whom displayed this triad.1
LS is most frequently associated with Fusobacterium necrophorum, an anaerobic, gram‑negative bacillus commonly found in the normal flora of the pharynx. It is a virulent organism that can cause an invasive disease due to several factors, including endo- and exotoxins.2 This can result in extension of the infection into the lateral pharyngeal space and, subsequently, into the IJV, causing septic thrombophlebitis and septic emboli of the lung, pleura, bone, and abdominal organs.3
Empirical treatment regimens for LS aim to target F. necrophorum and oral streptococci, and include piperacillin / tazobactam, a carbapenem, or ceftriaxone with metronidazole.4 Duration of antibiotic therapy depends on clinical progress and the presence or absence of septic complications; however, the current recommendation is to continue the therapy for a minimum of 4 weeks.5 Additional aspects to consider are the need for source control in the event of septic collections and whether anticoagulation is required for the thrombus. Currently, it is recommended not to use anticoagulation unless there is progression of the thrombus or persistent bacteremia after 5 days of appropriate antibiotic therapy.4
Following the introduction of antibiotics, the number of LS cases has fallen over the decades, and it is now considered a rare disease.6 It is typically seen in otherwise healthy adolescents, and is often a difficult diagnosis to reach.7
Here, we review 3 normally fit and well patients, who presented to the same health board over a period of 6 months and were each diagnosed with LS. Their presenting symptoms, test results, and suspected sources of infection were not in keeping with the classic triad, and each case posed their own diagnostic challenge. They were all critically unwell and took an average of 13 days to diagnose. We aimed to raise the awareness of atypical presentations of this rare, life‑threatening disease and advocate early imaging of the neck to aid the diagnosis.
Case 1 was a 19‑year‑old woman who presented with swollen neck glands, sore throat, and dry cough. She also complained of shortness of breath, malaise, anorexia, and an intermittent rash. On physical examination she was afebrile, hypotensive, with tender cervical lymphadenopathy, and right basal crackles. Pulmonary infiltrates progressed to bilateral cavitating lesions (Figure 1A–1C) over 48 hours and she rapidly deteriorated, developing fever and respiratory failure requiring regular review by the Critical Care team. Her pyrexia failed to improve despite intravenous administration of co‑amoxiclav and clarithromycin and, subsequently, piperacillin / tazobactam. The diagnosis of LS was raised on the fourth day since her admission. Computed tomography of the neck confirmed a right IJV thrombus (Figure 1D) supporting the diagnosis. Metronidazole was added for anaerobic cover. She gradually improved and was discharged after 14 days of hospitalization with a further 2‑week treatment with co‑amoxiclav and metronidazole. She was not anticoagulated for the thrombus and has recovered well.
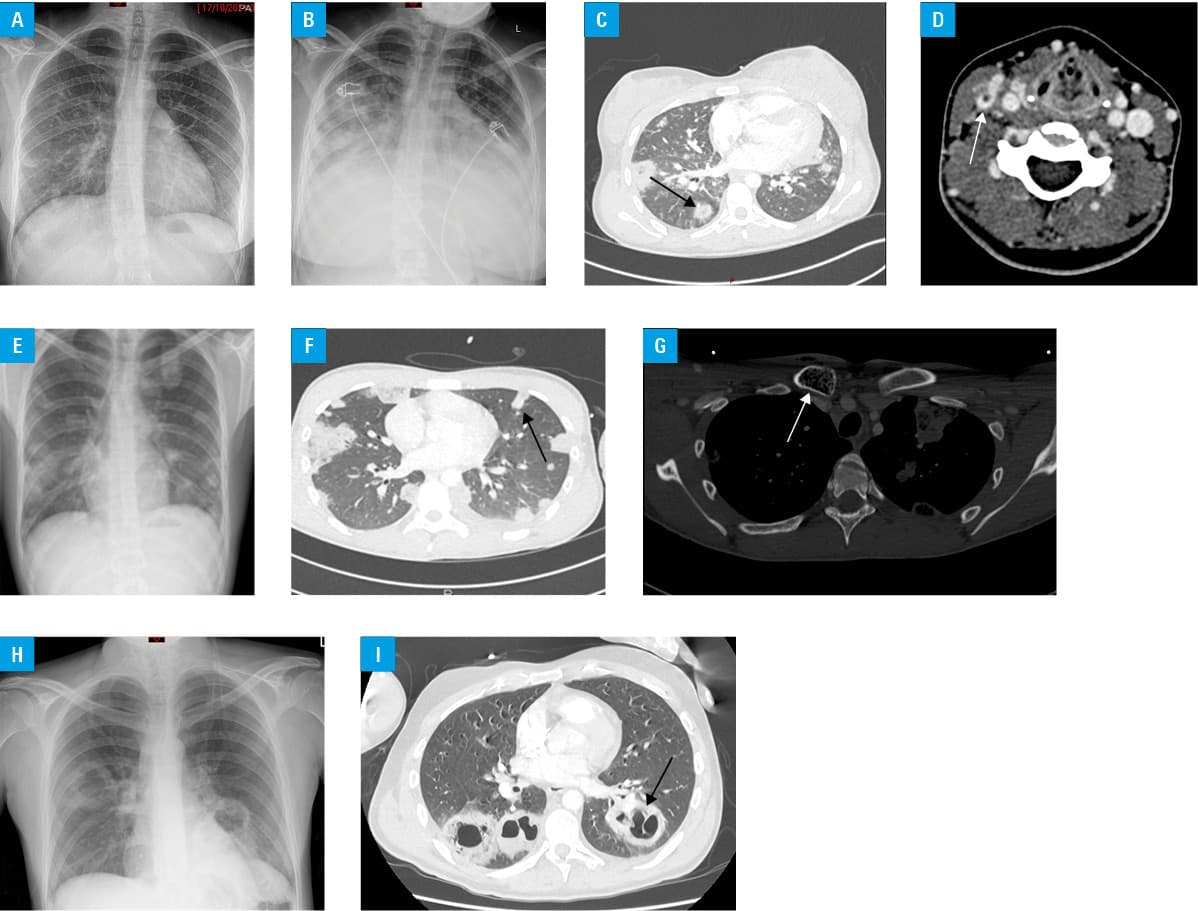
Case 2 was an 18‑year‑old man who was admitted with shortness of breath for 1 week, fever, sore throat, and cough productive of brown sputum which had started after inhaling a large volume of dust whilst demolishing a wall. He was a heavy smoker, including cannabis, worked as a laborer, and had a documented penicillin allergy. Examination revealed tachypnea, tachycardia, and hypoxia which quickly progressed to respiratory failure requiring intubation and ventilation. Imaging tests revealed bilateral, cavitating pulmonary lesions, hepatosplenomegaly, and osteomyelitis of the right clavicular head (Figure 1E–1G). The Infectious Diseases team advised treatment with a combination of meropenem, linezolid, metronidazole, and doxycycline, which was rationalized to meropenem and linezolid after 1 week. Antifungal therapy was added due to a concern regarding a fungal infection and inhalation injury given the history of demolition. He clinically improved but remained pyrexial 3 weeks into his admission. The initial imaging test results were reviewed and an absence of contrast uptake in the left IJV was noted. A neck ultrasound confirmed a thrombus, raising the possibility of LS. The patient was restarted on metronidazole in combination with meropenem. The right clavicular osteomyelitis was revisited and he underwent surgical debridement and local administration of co‑amoxicalv, as the suspicion of penicillin allergy was low. He improved significantly and was afebrile within 24 hours of the surgery. He developed leucopenia in relation to his meropenem treatment and was ultimately switched to oral co‑amoxiclav with additional amoxicillin for a total of 6 weeks. F. necrophorum was detected in the bone biopsy by the bacterial 16S ribosomal RNA (rRNA) polymerase chain reaction (PCR) screening, supporting the diagnosis of LS. A decision to anticoagulate the thrombus was made given the complexity of his case and duration of illness. He was discharged after a total of 44 days in the hospital and has made a full recovery.
Case 3 was a 29‑year‑old man who was admitted with shortness of breath and cough productive of black sputum. He complained of anorexia, malaise, headache, and jaundice. He was a smoker and had a history of recurrent skin abscesses, one of which he had recently drained himself on his jawline. On physical examination he was unwell, febrile, cachectic, and jaundiced, with tachypnea and tachycardia but normal oxygen saturation and blood pressure. He had poor dentition and a chest examination revealed left basal crackles. Imaging tests revealed bilateral cavitating lesions (Figure 1H and 1I), pulmonary emboli, and normal intra‑abdominal organs. A neck ultrasound was unremarkable. During subsequent consultations, he reported several weeks of otorrhea and hearing loss in his right ear. A computed tomography of the head and neck revealed evidence of a right cholesteatoma with a right IJV and proximal sigmoid sinus thrombus in keeping with a diagnosis of LS. His co‑amoxiclav and flucloxacillin regimen was switched to ceftriaxone to cover for central nervous system involvement and metronidazole was added to ensure anaerobic cover. He was ultimately switched to 6 weeks of oral levofloxacin to ensure adequate pseudomonal cover given his cholesteatoma and was discharged with a recommendation for an ear, nose, and throat follow‑up. He was anticoagulated for 3 months for his provoked pulmonary emboli and has recovered from his respiratory illnesses.
Each of these patients posed their own diagnostic challenge despite input from several specialists. They all had a wide range of abnormal test results, which required a multisystem approach.
On review of their initial presentations, the unifying symptoms were cough and shortness of breath. Fever was documented for all patients but not necessarily at the time of presentation. Sore throat and swollen glands were reported by 2 patients and hearing loss with discharge by 1 patient. Raised levels of inflammatory markers were the only abnormal blood test result shared by all 3 patients at the time of admission. Two patients were found to be thrombocytopenic and to have severe renal impairment, and 2 were found to have hyperbilirubinemia. All 3 patients had bilateral, cavitating pulmonary lesions and, subsequently, an IJV thrombus on imaging. Of note, the typical causative organism, F. necrophorum, was not grown on any blood cultures and was only detected in the bone biopsy on bacterial 16S (rRNA) PCR screening in 1 patient.
With regard to the overarching diagnosis of LS, the finding of an IJV thrombus was the result that clinched the diagnosis for these patients. This highlights the importance of early neck imaging in young patients presenting with cavitating pneumonia. Once the diagnosis was made, antibiotic therapy could be rationalized to target the presumed causative organism, F. necrophorum. The underlying suspected source of infection is important to consider when choosing the appropriate antibiotic.
Another important factor demonstrated here is the role of source control in the clinical progress of patients. A significant improvement in pyrexia was seen in one of the patients following surgical debridement, which emphasizes the importance of involving specialists early if interventional procedures may be required.
Finally, with regard to anticoagulation in LS, it is reassuring to note that the patient who did not receive any anticoagulation experienced no adverse outcomes. This supports the concept that anticoagulation is not required when there is a positive clinical response to antibiotic therapy.
The presented cases demonstrate the diagnostic challenge posed by LS, and the role of the neck imaging in the diagnosis. We suggest that clinicians have a low threshold for arranging imaging of the neck when young, typically well patients present with cavitating pneumonia. It should also be remembered that LS does not solely relate to infections of the oropharynx, and other sources, such as the inner ear, need to be considered.
- Lemierre A. On certain septicemias due to anaerobic organisms. Lancet. 1936; 1: 701‑703. | Crossref
- Allen BW, Anjum F, Bentley TP. Lemierre syndrome. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK499846/. Accessed June 16, 2022.
- Jafri FN, Shulman J, Gómez‑Márquez JC, et al. Sore throat, fever, septic emboli, and acute respiratory distress syndrome: a case of Lemierre syndrome. Case Rep Emerg Med. 2018; 2018: 7373914. | Crossref
- UpToDate website. Spelman D. Lemierre syndrome: septic thrombophlebitis of the internal jugular vein. https://www.uptodate.com/contents/lemierre‑syndrome‑septic‑thrombophlebitis‑of‑the‑internal‑jugular‑vein. Accessed June 16, 2022.
- Hagelskjaer Kristensen L, Prag J. Lemierre’s syndrome and other disseminated Fusobacterium necrophorum infections in Denmark: a prospective epidemiological and clinical survey. Eur J Clin Microbiol Infect Dis. 2008; 27: 779. | Crossref
ARTICLE INFORMATION