Type 2 diabetes mellitus (T2DM) has become a ubiquitous metabolic disease. It shows a great variety of clinical presentations, some of which are rare and not well understood. One of such uncommon neurological manifestations is diabetic striatopathy (DS), also referred to as nonketotic hyperglycemic hemichorea or chorea hyperglycemia basal ganglia syndrome. It is seen mostly in elderly T2DM women with hyperglycemia, predominantly without ketosis, and is characterized by choreiform movements of the body due to a dysfunction of the basal ganglia. Because of its rarity, the pathophysiology of this condition is poorly understood, and there are no established guidelines regarding treatment strategies. Lack of familiarity with this uncommon manifestation can lead to a missed diagnosis or even a misdiagnosis.
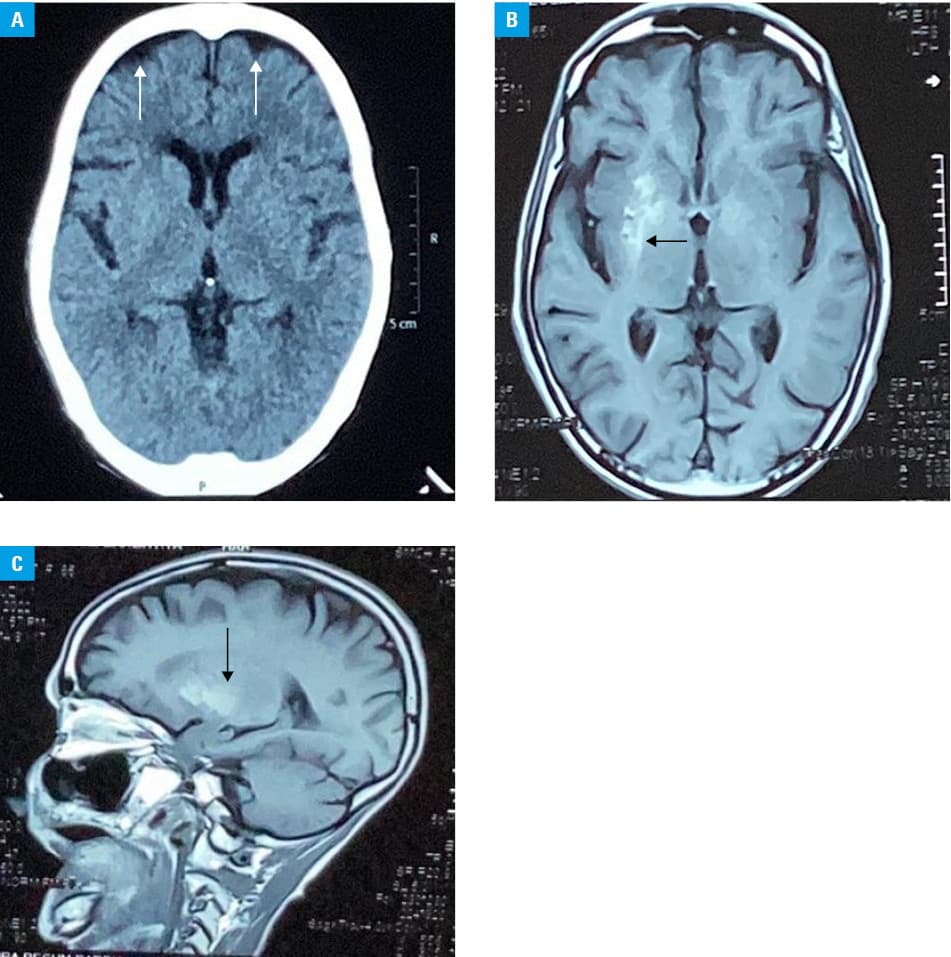
We describe a case of a 65‑year‑old postmenopausal woman who presented with abnormal movements on the left side of the body. She had a history of long‑standing T2DM and had been taking insulin irregularly. The abnormal body movements were of a sudden onset, starting 30 days prior to the presentation. They were of a rapid, dance‑like, continuous nature. Initially, they involved only the left hand fingers but they subsequently moved up proximally to involve larger muscle groups. Also, the amplitude of the movements had been increasing gradually. The shoulder joint muscles were mostly spared. The left leg became involved 3 days before the presentation and clumsy, fidgety movements around the left knee and left ankle joint could be observed. The trunk, neck, and face were spared, as was the right side of the body. The clinical picture was suggestive of hemichorea, wherein the distal joints are more involved than the proximal ones; and the symptoms subsided completely during sleep, which invariably happens in chorea. Vital signs were normal, and the neurological examination revealed reduced muscle tone across the left wrist and left elbow joint. The patient’s higher mental functions were normal, with no dissociative features suggestive of an underlying psychiatric condition. The capillary blood glucose level was measured using a strip‑based glucometer, which indicated a highly elevated glucose concentration exceeding 600 mg/dl (reference range, 70–139 mg/dl). The patient was admitted and intravenous crystalloids were administered to correct dehydration. Also, an infusion of regular insulin was started. The blood glucose level was reduced on the day of the admission but the symptoms of chorea continued. A non–contrast‑enhanced computed tomography (CT) scan of the brain was also performed on the first day, and revealed no abnormalities except for age‑related atrophy (Figure 1A). Chorea was still present after 3 days of hospitalization despite euglycemia; therefore, oral clonazepam (0.5 mg once daily) was added in the hope that a gamma‑aminobutyric acid (GABA) receptor agonist would reduce the symptoms. Brain magnetic resonance imaging (MRI) was performed, and the results showed hyperintensity on T1‑weighted imaging in the right lentiform nucleus, with no changes in the thalamus on that side (Figure 1B and 1C). The T1‑weighted lesion was localized contralaterally to the side of hemichorea, which involved the left side of the body. A triad of hyperglycemia with hemichorea and a striatal T1‑weighted hyperintense lesion contralateral to the side of chorea led to the diagnosis of DS. A T2‑weighted MRI scan showed a heterogeneously hyperintense lesion in the right lentiform nucleus. The patient was discharged on request of her family as the symptoms of chorea were not nullified or minimized after 6 days of euglycemia and 3 days of treatment with oral clonazepam. She was prescribed biphasic insulin to be taken twice daily and was referred to a higher‑level treatment center for better management of chorea.
DS is a rare neurological manifestation of poorly controlled hyperglycemia seen in elderly diabetic women, predominantly those without ketosis. It usually presents as hemichorea. Unilateral arm and leg involvement is a common presentation but both sides of the body, as well as the trunk and face, can be involved. The symptoms usually develop suddenly at the peak of nonketotic hyperglycemia. Rarely, chorea can be the first presentation of uncontrolled diabetes. On the other hand, chorea may present a few weeks after an episode of uneventful hyperglycemia has been resolved or treated—a scenario that is sometimes called delayed‑onset DS.1 Hyperintensity in the striatum (particularly in the putamen and / or caudate nucleus) on T1‑weighted imaging is the most consistent MRI finding in DS. MRI is the modality of choice to assess this condition, as it is more sensitive than CT. Hyperintensity on T1‑weighted imaging is hypothesized to be due to increased protein hydration within gemistocytes. According to the literature, other imaging findings are variable but generally include a hypointense lesion on the T2‑weighted / fluid‑attenuated inversion recovery MRI sequence, increased susceptibility on susceptibility‑weighted imaging, high diffusion signal on diffusion‑weighted imaging, and hyperdensity in the striatum on brain CT; however, a CT scan can miss the diagnosis, as was the case in the present case study. Also, the other findings do not present with the same frequency as T1‑weighted hyperintensity and tend to vary. Lesions detected on imaging gradually resolve after correction of hyperglycemia but they tend to do so more slowly than the clinical abnormalities.2,3 DS is a poorly understood condition, probably occurring due to hyperviscosity secondary to hyperglycemia, leading to regional blood–brain barrier disruption and metabolic damage, augmented sensitivity of dopaminergic receptors in postmenopausal women (explaining the female predominance), and decreased GABA availability in the striatum secondary to the nonketotic state.2 It has been hypothesized that in nonketotic hyperglycemia, brain metabolism shifts to the alternative anaerobic pathway in the Krebs cycle, which leads to a rapid depletion of GABA. This results in disinhibition of the subthalamus and basal ganglia, finally causing chorea. However, in ketotic states, usually seen in type 1 diabetes, GABA can be resynthesized using acetoacetate produced in the liver to prevent its reduction. Therefore, DS is rarely seen in diabetes with ketoacidosis.4 Symptoms of chorea may improve within hours of achieving euglycemia but they can also persist for days to months, even after correction of the glucose level.1 Of note, hypoglycemia is to be avoided as it may slow down recovery or even worsen the symptoms of chorea, as shown previously.5 Earlier studies indicated benefits conferred by antichorea drugs, such as haloperidol.3 In our case, we suspect that GABA stores were severely depleted, and therefore a GABA receptor agonist (clonazepam) did not prove to be very helpful. Finally, it is also important to get acquainted with mimickers presenting with a unilateral hyperintense lesion on T1‑weighted MRI or unilateral hyperdensity on a CT scan.
- Osborn AG, Hedlund GL, Salzman KL. Osborn’s Brain: Imaging, Pathology, and Anatomy, Second edition. Philadelphia, PA: Elsevier; 2018.
- Radiopaedia.org. Gaillard F, Sharma R, Foster T. Non‑ketotic hyperglycemic hemichorea. https://radiopaedia.org/articles/21924. Accessed June 19, 2022. | Crossref
- Homaida M, Kanodia AK, Young N, et al. Diabetic striatopathy: a rare condition and diagnostic dilemma. BMJ Case Rep. 2021; 14: e240141. | Crossref
- Chua CB, Sun CK, Hsu CW, et al. “Diabetic striatopathy”: clinical presentations, controversy, pathogenesis, treatments, and outcomes. Sci Rep. 2020; 10: 1594. | Crossref
- Rupp J, Gillespie A. A case of diabetic hemichorea hemiballismus exacerbated by hypoglycemia. AACE Clin Case Rep. 2021; 7: 327‑329. | Crossref
ARTICLE INFORMATION