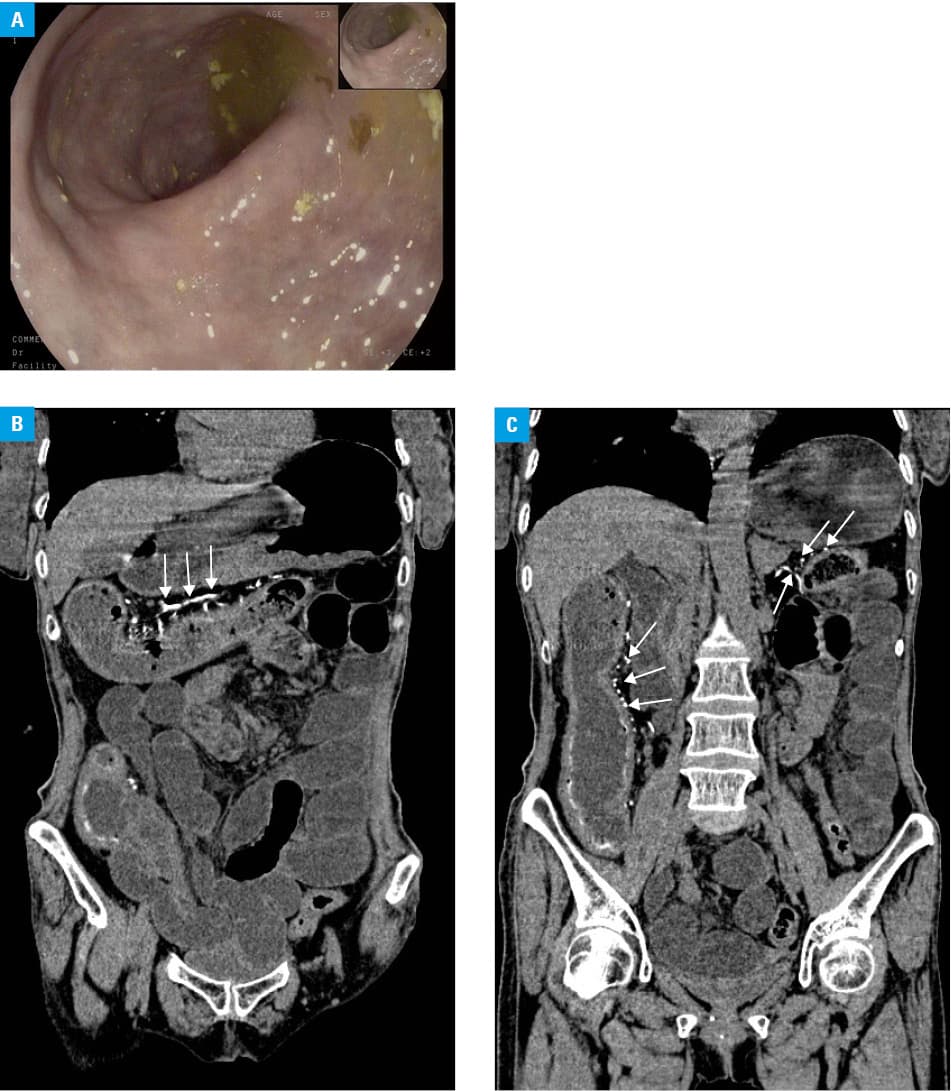
A 65‑year‑old woman presented to our hospital with complaints of recurrent dull aching pain in the right lower abdomen for 1 month. The patient had no fever, nausea or vomiting, diarrhea or melena, and experienced weight loss of nearly 8 kg in 6 months. Apart from these, she had recurrent abdominal distension and constipation. Physical examination revealed an abdominal bulge with mild tenderness in the right lower abdomen, but the cause of pain was not obvious. The patient did not have a history of chronic liver disease, alcohol abuse, or any other relevant medical history that could cause portal hypertension. It is worth noting that she had a 10‑year history of taking a Chinese medicine of unknown composition due to thyroid nodules. No laboratory abnormalities were found apart from increased C‑reactive protein level (96 mg/l; reference range, <6 mg/l). Enteroscopy revealed that the entire colon mucous membrane was purple (Figure 1A). Pathologic examination demonstrated acute and chronic inflammation with proliferation of fibrotic tissue in the intestinal mucosa. A computed tomography (CT) scan of the abdomen and pelvis presented diffuse colon wall thickening and intestinal obstruction (intestinal distension with massive effusion), with extensive calcification of the mesenteric vessels (Figure 1B and 1C). A diagnosis of phlebosclerotic colitis (PC) was established. The patient was treated with levofloxacin and low‑molecular‑weight heparin. At the same time, papaverine was administered to improve microcirculation. The symptoms resolved following 1 week of treatment. The patient was stable during a 1‑year follow‑up.
PC is a rare condition characterized by extensive calcification of the mesenteric veins and thickened colon wall.1-4 PC is more common in women, and the possible etiology was attributed to certain toxins uptake (eg, Chinese herbal medicine containing geniposide), resulting in vascular damage to the intestinal wall that causes vessel wall fibrosis and calcification.1-3 In a considerable subset of patients, PC presents with atypical clinical symptoms (eg, acute or chronic abdominal pain), and laboratory workup usually indicates general inflammatory responses or no abnormalities. The mucosal appearance at endoscopy is bluish violet, and mucosal swelling with submucosal varices could also be observed.4 Notably, these endoscopic features are easily misdiagnosed as inflammatory bowel disease. Thickening of the colonic wall with extensive calcifications of the mesenteric vein on CT directly confirm the diagnosis.5 Patients with mild symptoms can be managed conservatively, including dilation of blood vessels, anti‑infective treatment, and nutritional support. If the patients develop signs of bowel ischemia or necrosis, resection is recommended.
- Chang YY, Lin HH, Lin CC. Phlebosclerotic colitis presenting as intestinal obstruction. Clin Gastroenterol Hepatol. 2014; 12: e81‑e82. | Crossref
- Chang KM. New histologic findings in idiopathic mesenteric phlebosclerosis: clues to its pathogenesis and etiology—probably ingested toxic agent‑related. J Chin Med Assoc. 2007; 70: 227‑235. | Crossref
- Hiramatsu K, Sakata H, Horita Y, et al. Mesenteric phlebosclerosis associated with long‑term oral intake of geniposide, an ingredient of herbal medicine. Aliment Pharmacol Ther. 2012; 36: 575‑586. | Crossref
- Shibata H, Nishikawa J, Sakaida I. Dark purple‑colored colon: sign of idiopathic mesenteric phlebosclerosis. Dig Endosc. 2014; 26: 604‑605. | Crossref
- Li YL, Cheung KK. Thread like calcifications in mesenteric phlebosclerosis. Abdom Radiol (NY). 2018; 43: 1504‑1505. | Crossref
ARTICLE INFORMATION