Multiple myeloma (MM) remains the third most common hematologic malignancy. Its global incidence average is 1.78 cases per 100 000, but in some regions (ie, northern Europe) it is almost twice as high (3.82/100 000).1,2 Solitary plasmacytoma accounts for less than 5% of plasma cell dyscrasias. Half of plasmacytomas are located within the bones and the remaining half in other organs. The incidence of extramedullary plasmacytoma is estimated at 0.063 per 100 000 in women and 0.78 per 100 000 in men, and the disease may have a highly unexpected and unpredictable clinical course.3,4 Testicular plasmacytoma is a very rare entity, with up to 70 cases reported to date; it accounts for about 0.03% to 0.1% of all testicular malignancies, either primary or metastatic.5 To the best of our knowledge, such a case has not yet been reported in Poland. Since most previous reports described unilateral testicular involvement, the case described herein is even more unique.
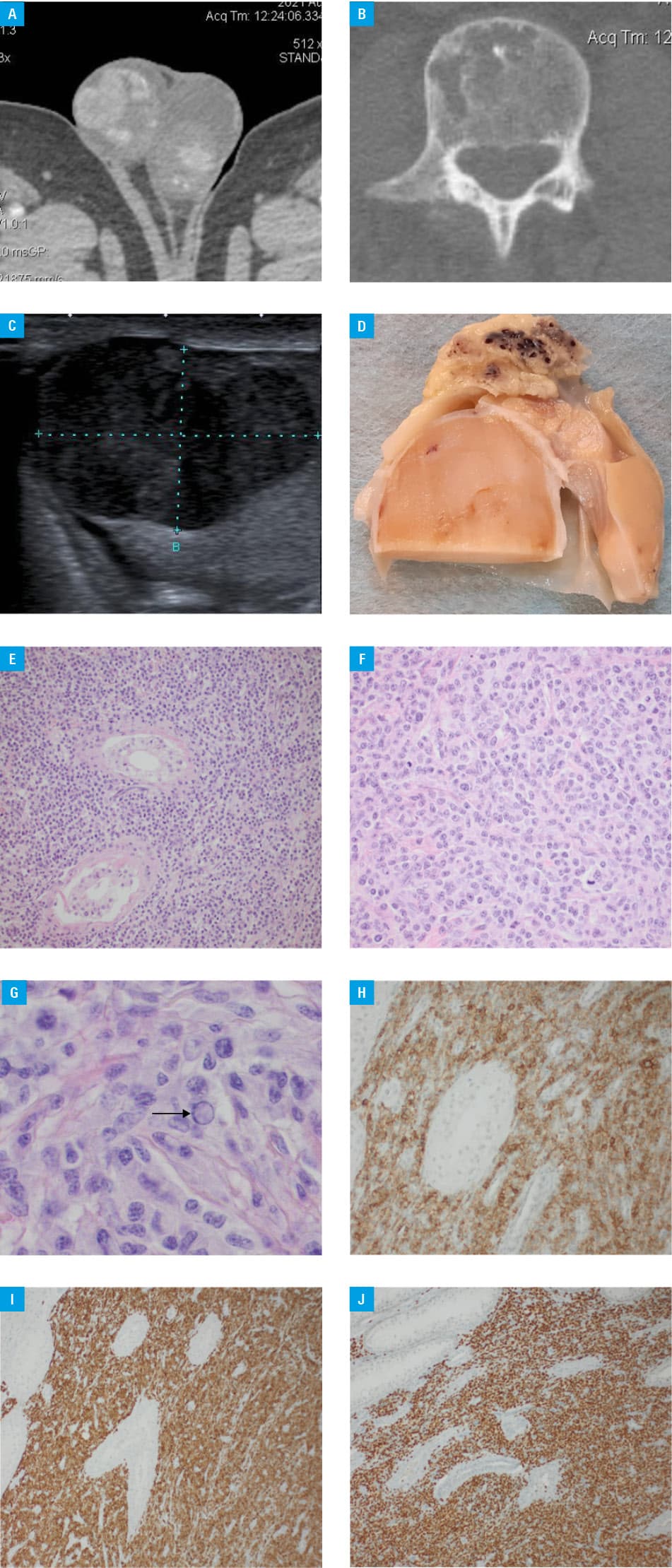
A patient aged 69 years was referred to the emergency department by his general practitioner due to apparent deep vein thrombosis (DVT). He also experienced recurrent epistaxis for the last few days. The laboratory test findings on admission were as follows: hemoglobin 9.9 g/dl (reference range [RR], 12.8–16.8 g/dl), white blood cell count 8310/μl (RR, 4000–10 500/μl), platelets 58 000/μl (RR, 150 000–450 000/μl), serum creatinine 1.8 mg/dl (RR, 0.7–1.2 mg/dl), serum albumin 28.7 g/l (RR, 35–50 g/l). Urinalysis revealed proteinuria 1.6 g/l (RR, <0.15 g/l) and microhematuria (RBC, 1600/μl; RR, <5/μl). The patient had no history of any chronic disease. Upon physical examination no remarkable abnormalities were found except for paleness, symmetric edema of lower legs, and tumorous appearance and enlargement of both testes. Ultrasound examination of lower legs excluded DVT. The autoantibody panel (antinuclear antibodies, anti‑dsDNA, antineutrophil cytoplasmic antibodies, antiphospholipid antibodies) was negative, complement components C3 and C4 were decreased (47.4 mg/dl; RR, 90–180 mg/dl and 3.1 mg/dl; RR, 10–40 mg/dl, respectively), and β2‑macroglobulin was elevated (5.37 mg/; RR, <3.0 mg/l). In addition, monoclonal immunoglobulin M (11.4 g/l) was found in serum. Κ and λ light chains were elevated (65.1 mg/l; RR, 3.3–19.4 mg/dl and 103.4 mg/l; RR, 5.71–26.3 mg/l, respectively), but the κ/λ ratio remained within the normal range. Since the laboratory test results were suggestive of monoclonal gammopathy and platelet count progressively decreased, the patient was consulted by a hematologist and a bone marrow (BM) biopsy was performed. The BM appeared hypoplastic, with signs of dyserythropoesis, but normal granulopoiesis and megakaryocytes, and plasma cells accounting for 3% to 4% of all cells. Computed tomography (GE Revolution Evo, Chicago, Illinois, United States) was also performed and revealed osteolytic lesions in the shaft of the right humerus and lumbar vertebrae. It also revealed irregular focal lesions enhanced after contrast infusion, suggestive of tumor or metastases in both testes (Figure 1A and 1B). A radiologist suggested testicular ultrasound to confirm these findings. The ultrasound (Toshiba Aplio 400, Tokyo, Japan) revealed multiple hypoechogenic focal lesions indicative of tumor or metastases (Figure 1C), pelvic and abdominal ultrasound was otherwise unremarkable. The patient was referred to a urologist who, based on the results of imaging and physical examination, decided to perform bilateral orchiectomy. A representative gross specimen of the testis is displayed in Figure 1D. Upon microscopic assessment, infiltration with polymorphic cells was found. Some were mature plasma cells with Dutcher bodies and spindle‑shaped plasma cells, whereas other were less mature, characterized by distinct nucleoli, mitotic Figures, and scant cytoplasm. The diagnosis was challenging, since immunohistochemistry staining for CD138 antigen (specific for plasma cells and MM cells) was negative. First, we excluded malignancies of germinal origin, cancer metastases, melanoma, and lymphoma. The cells were positive for the following antigens: CD38, MUM1, CD79a, CD43, bcl2, and weakly positive for leukocyte common antigen. Κ and λ light chain positivity was also identified in some cells. The cells were negative for CD20, PAX5, CD56, CD117, cyclin D1, CD3, and C‑MYC (Figure 1E–1J; see Supplementary material, Table S1 for the list of abbreviations). Lack of CD138 positivity with expression of κ and, less abundantly, λ light chains in the cells forming the tumor was considered unexpected, but the remaining histologic features together with the clinical / laboratory data indicating monoclonal gammopathy led us to a diagnosis of bilateral testicular plasmacytoma.
The patient started initial systemic treatment with dexamethasone and cyclophosphamide, with a plan to commence proteasome inhibitor in the near future. However, due to a series of severe infectious complications (including COVID‑19), pronounced anemia, development of bilateral hydronephrosis requiring double‑J ureteral stents, and low percentage of plasma cells in BM biopsy, any further systemic treatment was postponed. Renal function deteriorated gradually and the patient needed renal replacement therapy. At the time of submission of this report (12 months following the initial referral) the patient is doing well, remains on maintenance hemodialysis and has no signs of gammopathy progression.
The presented case is not a true “solitary” plasmacytoma and we think that a diagnosis of MM should be established in our patient. Even though the BM involvement criterion of MM was not fulfilled, the presence of solitary extramedullary tumor together with osteolytic lesions and renal failure allow for establishing such a diagnosis (according to the 4th edition of the World Health Organization diagnostic criteria of MM, published in 2016).
Three strategies are recommended in solitary plasmacytomas and they include radiation, surgery, and systemic therapy, but due to a limited number of cases and paucity of data none of them is evidence‑based (although radiation is considered the best option, depending on the tumor location).2 The treatment of testicular plasmacytoma is even less standardized but according to most reports orchiectomy is the treatment of choice.5
- Huang J, Chai Chan S, Lok V, et al. The epidemiological landscape of multiple myeloma: a global cancer registry estimate of disease burden, risk factors, and temporal trends. Lancet Haematol. 2022; 9: e670‑e677. | Crossref
- Charliński G, Tyczyńska A, Małecki B, et al. Risk factors and causes of early mortality in patients with newly diagnosed multiple myeloma in a “real‑world” study: experiences of the Polish Myeloma Group. Pol Arch Intern Med. 2021; 131: 527‑534. | Crossref
- Pham A, Mahindra A. Solitary plasmacytoma: a review of diagnosis and management. Curr Hematol Malig Rep. 2019; 14: 63‑69. | Crossref
- Hałka J, Spaleniak S, Michalak M, et al. Solitary multiple myeloma as a very rare cause of hypophosphatemia, micturition, and defecation disorders. Pol Arch Intern Med. 2022; 132: 16259. | Crossref
- Vusqa UT, Asawa P, Fazal S, Samhouri Y. Testicular plasmacytoma masking as epididymo‑orchitis in a known multiple myeloma patient. Cancer Diagn Progn. 2022; 2: 549‑552. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION