Oxidized phospholipids associated with lipoprotein(a) contribute to hypofibrinolysis in severe aortic stenosis

 CC BY 4.0
CC BY 4.0
Oxidized phospholipids associated with lipoprotein(a) contribute to hypofibrinolysis in severe aortic stenosis
Introduction
Aortic stenosis (AS) is the most prevalent cause of acquired valvular heart disease in the aging population with no available pharmacotherapy to reduce or inhibit the disease progression. Within the stenotic aortic valves, a prominent accumulation of lipoproteins has been observed, being an essential component of AS development.1 Lipoprotein(a) (Lp[a]) is a major carrier of phospholipids and their oxidized forms (OxPLs), which shows both proatherogenic and prothrombotic properties.2 Data indicated that OxPLs are co‑expressed with Lp(a) within the stenotic leaflets and promote valvular calcification.1,3 A genome‑wide association study4 revealed that LPA rs10455872 polymorphism was significantly associated with a 2‑fold increased risk of aortic leaflet calcification. Kamstrup et al5 demonstrated that OxPL levels were associated with increased risk of AS (odds ratio [OR] of 2.0 (1.3–3.1) for 91st to 95th percentile levels). Recently, Siudut et al6 reported that in AS Lp(a) and oxidized low‑density lipoprotein contribute to hypofibrinolysis reflected by prolonged clot lysis time (CLT), and hypofibrinolysis has been shown to be associated with AS severity.7 It is tempting to speculate that OxPL associated with Lp(a) contribute to hypofibrinolysis and thus AS severity.
The aim of this study was to evaluate whether in patients with severe AS elevated serum concentrations of OxPL are associated with increased Lp(a) level, impaired fibrinolysis, and AS severity.
Patients and methods
Between October 2018 and November 2020, we recruited 70 patients with symptomatic severe AS. Fifty patients had Lp(a) concentration equal to or above 50 mg/dl and 20 had a Lp(a) level below 50 mg/dl, with a threshold for Lp(a) being equal to or above 50 mg/dl according to a recent European Atherosclerosis Society consensus statement.8 All AS patients underwent first‑time elective surgical aortic valve replacement at the Department of Cardiovascular Surgery and Transplantology at the John Paul II Hospital, Kraków, Poland. Data on medical history, current treatment, and demographics were collected using a standardized questionnaire. Severe AS was defined as mean transvalvular pressure gradient (PGmean) equal to or above 40 mm Hg, peak transvalvular velocity (Vmax) equal to or above 4.0 m/s, and aortic valve area (AVA) equal to or below 1 cm2 on transthoracic echocardiography. Arterial hypertension and hypercholesterolemia were diagnosed as previously described.6,9
The exclusion criteria for AS patients included atherosclerotic vascular disease requiring revascularization, acute infection including infective endocarditis, rheumatic AS, diabetes mellitus, advanced chronic kidney disease, need for concomitant valvular surgery (eg, mitral valve repair), percutaneous coronary intervention, recent (<3 months) acute coronary syndrome or cerebrovascular episode, diagnosed malignancy, and pregnancy. The valvular anatomy was confirmed intraoperatively by a cardiac surgeon, and patients with bicuspid valve and root / ascending aortic dilatation requiring intervention were excluded from the study. The diagnosis of atherosclerosis was based on angiographically documented coronary artery stenosis greater than 20% of the diameter and such patients were excluded from the study to avoid any influence of nonobstructive atherosclerosis.10
The ethics committee approved the study (8/KBL/OIL/2019 and 53/KBL/OIL/2022) and all participants provided their written informed consent in accordance with the Declaration of Helsinki.
Fasting venous blood was drawn between 7:00 and 9:00 am before the aortic valve replacement. Routine laboratory assays were used to assess glucose, creatinine, lipid profile, C‑reactive protein and fibrinogen. Lp(a) was evaluated using immunoturbidimetry (Roche Diagnostics, Mannheim, Germany). Plasminogen and α2-antiplasmin activity in plasma samples were measured by chromogenic assays (Siemens Healthcare, Marburg, Germany).
Aortic valves were collected during open heart surgery, embedded in Cryomatrix (Thermo Scientific, Kalamazoo, Michigan, United States), and sectioned into 4.5 μm slices with a Leica CM1520 cryostat. Immunostaining was performed on 30 valves from the patients with serum Lp(a) level equal to or above 50 mg/dl and 20 valves from the patients with Lp(a) level below 50 mg/dl, as described previously.11 The primary antibody was used against OxPL (E06; Avanti Polar Lipids, Alabaster, Alabama, United States). The secondary goat antibody conjugated with AlexaFluor 488 (Abcam, Cambridge, United Kingdom; 1:1000) was applied in the dark. Olympus BX43 microscope (Tokyo, Japan) was used to visualize and analyze the images. The percentage of immunopositive areas was calculated as previously,11 and 15 serial step sections were analyzed per each valve by 2 independent observers.
The levels of human tissue plasminogen activator (tPA), plasminogen activator inhibitor type 1 (PAI‑1) antigen, and thrombin activatable fibrinolysis inhibitor (TAFI) (all Hyphen Biomed, Neuville‑sur‑Oise, France), along with OxPL (Cell Biolabs, San Diego, California, United States) concentrations were assayed quantitatively in plasma or serum samples12 using the enzyme‑linked immunosorbent assay in accordance with the manufacturers’ instructions.
CLT in plasma samples was measured as described previously.13 Briefly, citrated plasma was mixed with thrombin (0.5 U/ml, Merck, Darmstadt, Germany), exogenous tPA (18 ng/ml, Boehringer Ingelheim, Germany), phospholipids (15 µM, Rossix, Mölndal, Sweden), and calcium ions. CLT was assessed turbidimetrically. The interassay coefficient of variation was below 6%.
Statistical analysis
All statistics were performed using the STATISTICA software (Version 13.3, TIBCO Software, Palo Alto, California, United States), and models were performed using R 4.1.1 package (The R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were presented as numbers and percentages, while continuous variables were expressed as mean and SD or median and interquartile range (IQR). Categorical variables were analyzed by the Pearson χ2 test or the 2‑tailed Fisher exact test. Normality was analyzed by the Shapiro–Wilk test. Differences between the groups were compared using the t test or the Mann–Whitney test, as appropriate. Associations between the variables were calculated using squared Pearson (r) or Spearman (R) correlation coefficients, as appropriate. The univariable linear regression models were performed to identify associations between CLT and laboratory, echocardiographic, and demographic variables. The variables that were associated with the prolonged CLT with a significance level below 0.2 in the univariable models or were clinically important were selected, and the multivariable linear model was fitted using stepwise regression with minimization of the Akaike information criterion, and adjusted for body mass index (BMI) with CLT as a dependent variable. The final model was validated using bootstrap resampling and examination of the residuals. Variance inflation factors were used to assess the multicollinearity. A P value below 0.05 was considered significant.
Results
The AS patients with Lp(a) level equal to or above 50 mg/dl did not differ from individuals with Lp(a) level below 50 mg/dl with regard to demographic and risk factors, used medications, or laboratory parameters (Supplementary material, Table 1). The AS patients with Lp(a) level equal to or above 50 mg/dl had by 10% higher Vmax (P <0.001), 13% higher PGmean (P = 0.04), 15% higher PGmax (P < 0.001), and 11% lower AVA (P = 0.003) than the patients with Lp(a) level below 50 mg/dl (Supplementary material, Table 1).
Valvular expression of OxPL was detected within all studied stenotic valves (Figure 1A and 1B), at the aortic side of the leaflets, and presented a condensed pattern of fluorescence. However, the patients with serum Lp(a) level equal to or above 50 mg/dl had enhanced valvular OxPL expression (21.4% [3.0] vs 16.6% [2.1] immunopositive area, P <0.001) and by 35% higher serum OxPL concentration (P = 0.03) than those with Lp(a) level below 50 mg/dl. Valvular amounts of OxPL were associated with serum OxPL concentration (R = 0.55, P = 0.002) and with Lp(a) concentration (R = 0.84, P <0.001). Moreover, the patients with Lp(a) level equal to or above 50 mg/dl were characterized by 11% longer CLT (P <0.001), 38% higher plasma PAI‑1 (P = 0.003), and 12% higher TAFI levels (P = 0.007) than those with Lp(a) level below 50 mg/dl (Supplementary material, Table 1). We did not observe any differences in plasma levels of tPA or plasminogen and α2-antiplasmin activity between the investigated groups (Supplementary material, Table 1). Interestingly, solely in the AS patients with Lp(a) level equal to or above 50 mg/dl, serum OxPL concentrations correlated with CLT, plasma levels of PAI‑1, and TAFI (Figure 1C–1E), but not with tPA, plasminogen, or α2-antiplasmin activity. Serum OxPL concentrations were also strongly associated with Vmax (R = 0.7, P <0.001), PGmean (R = 0.62, P <0.001), and weakly with AVA (R = –0.32, P = 0.02). As expected, serum Lp(a) levels positively correlated with CLT, PAI‑1 concentration, and AS severity reflected by Vmax and PGmean (data not shown).
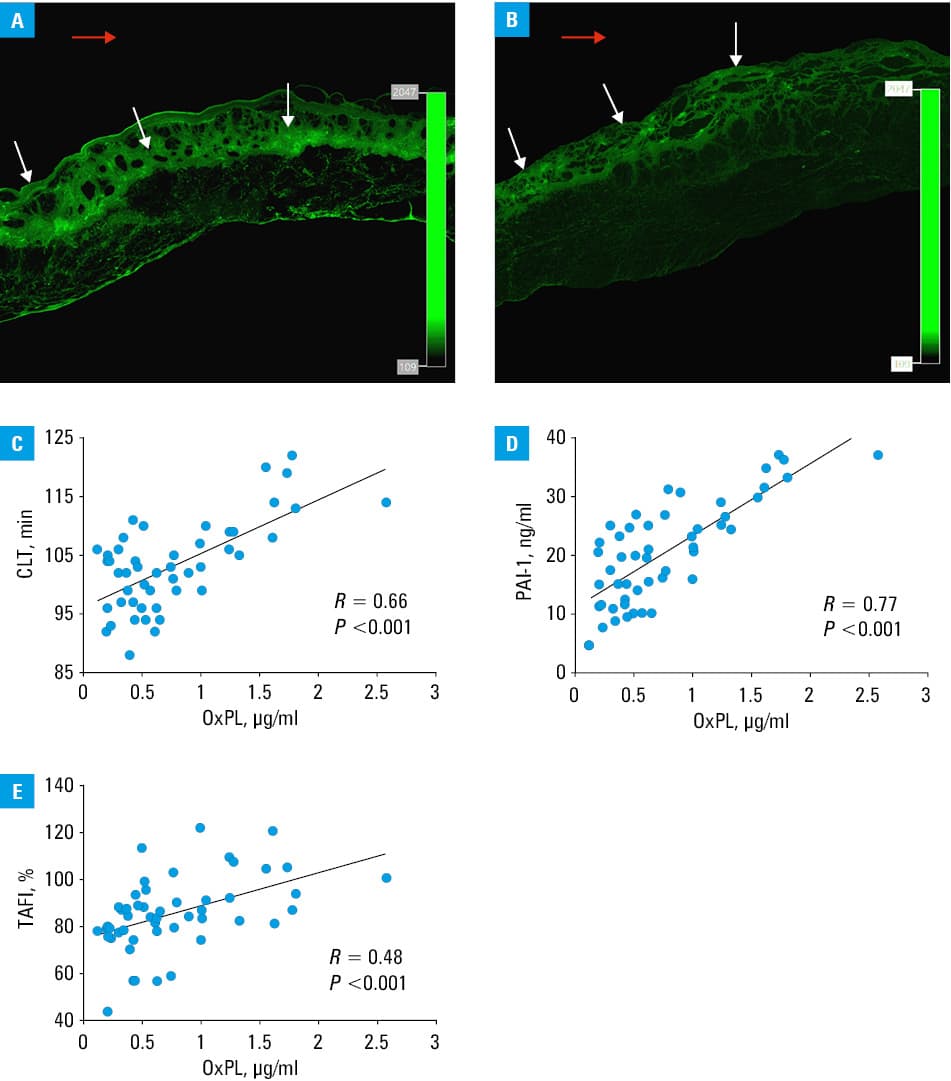
Abbreviations: AS, aortic stenosis; CLT, clot lysis time; Lp(a), lipoprotein(a); OxPLs, oxidized phospholipids; PAI‑1, plasminogen activator inhibitor 1; TAFI, thrombin activatable fibrinolysis inhibitor
The univariable linear regression analysis showed that OxPL, Lp(a), PAI‑1, TAFI, disease severity, and age, but not plasminogen activity were associated with CLT in the AS patients with Lp(a) level equal to or above 50 mg/dl (Supplementary material, Table 2). The multiple linear regression analysis adjusted for BMI showed that higher OxPL levels predicted prolonged CLT in severe AS patients with Lp(a) level equal to or above 50 mg/dl (Supplementary material, Table 2).
Discussion
This study is the first to show that in patients with severe AS and Lp(a) level equal to or above 50 mg/dl OxPLs are associated with impaired fibrinolysis and a have stronger impact on CLT than Lp(a). We also observed enhanced valvular OxPL expression in the patients with increased serum Lp(a) concentrations.
Lp(a) is the major plasma pool of OxPL and, as shown by Leibundgut et al,14 the second plasma pool of OxPLs is circulating with plasminogen, which in physiological conditions facilitates fibrinolysis by conversion of plasminogen to plasmin. However, at increased Lp(a) levels, OxPLs impair fibrinolysis by inhibiting tPA‑mediated plasminogen activation and inhibition of plasminogen binding to fibrin.14
The present study extended the observations of Siudut et al,6 and showed a stronger association of OxPL with hypofibrinolysis in AS patients than with Lp(a). In addition, given that in AS patients hypofibrinolysis is linked to the disease severity,6,7 our observation that OxPL level correlates with AS severity seems justified.
Moreover, we showed that valvular OxPL expression was related to both serum OxPL and Lp(a) concentrations, which may suggest that OxPL‑lowering therapies could be of importance in retardation of AS progression.
The study limitations should be acknowledged. The number of enrolled patients was limited, especially those with Lp(a) level below 50 mg/dl. However, the study was adequately powered and it represents typical patients with symptomatic severe AS in clinical practice. Moreover, the levels of OxPL and markers of fibrinolysis were measured once at enrolment, thus they may not reveal some associations. Our results cannot be directly extrapolated to individuals with mild or moderate AS.
In conclusion, our study showed that in patients with severe AS increased OxPL levels were associated with prolonged CLT and the disease severity. Larger studies are needed to confirm the observed associations.
- Yu B, Hafiane A, Thanassoulis G, et al. Lipoprotein(a) induces human aortic valve interstitial cell calcification. JACC Basic Transl Sci. 2017; 2: 358‑371. | Crossref
- Anuurad E, Boffa MB, Koschinsky ML, Berglund L. Lipoprotein(a): a unique risk factor for cardiovascular disease. Clin Lab Med. 2006; 26: 751‑772. | Crossref
- Yeang C, Wilkinson MJ, Tsimikas S. Lipoprotein(a) and oxidized phospholipids in calcific aortic valve stenosis. Curr Opin Cardiol. 2016; 31: 440‑450. | Crossref
- Thanassoulis G, Campbell CY, Owens DS, et al; CHARGE Extracoronary Calcium Working Group. Genetic associations with valvular calcification and aortic stenosis. N Engl J Med. 2013; 368: 503‑512.
- Kamstrup PR, Hung MY, Witztum JL, et al. Oxidized phospholipids and risk of calcific aortic valve disease: the Copenhagen general population study. Arterioscler Thromb Vasc Biol. 2017; 37: 1570‑1578. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION