Catastrophic antiphospholipid syndrome presenting initially as severe abdominal pain



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Catastrophic antiphospholipid syndrome presenting initially as severe abdominal pain
A 52‑year‑old man, who complained of severe abdominal pain for 1 day, was admitted to our hospital. The patient was previously healthy. He experienced persistent colic pain in the left side and near the umbilical area. Physical examination revealed left periumbilical tenderness. He was diagnosed with acute kidney injury, pulmonary embolism, and abdominal pain of unknown origin, thus he was treated with analgesic and anticoagulant drugs. On the following day, he developed high fever and oliguria. Supplementary material, Table S1 shows the results of his laboratory workup. Based on the arterial blood gas analysis results, the patient presented with type 1 respiratory failure. The antibody levels of anti‑cardiolipin and anti-β2 glycoprotein were markedly enhanced. However, the levels of a spectrum of antinuclear antibodies and tumor markers were normal. A vascular ultrasound of both lower limbs revealed bilateral deep vein thrombosis and right popliteal artery occlusion.
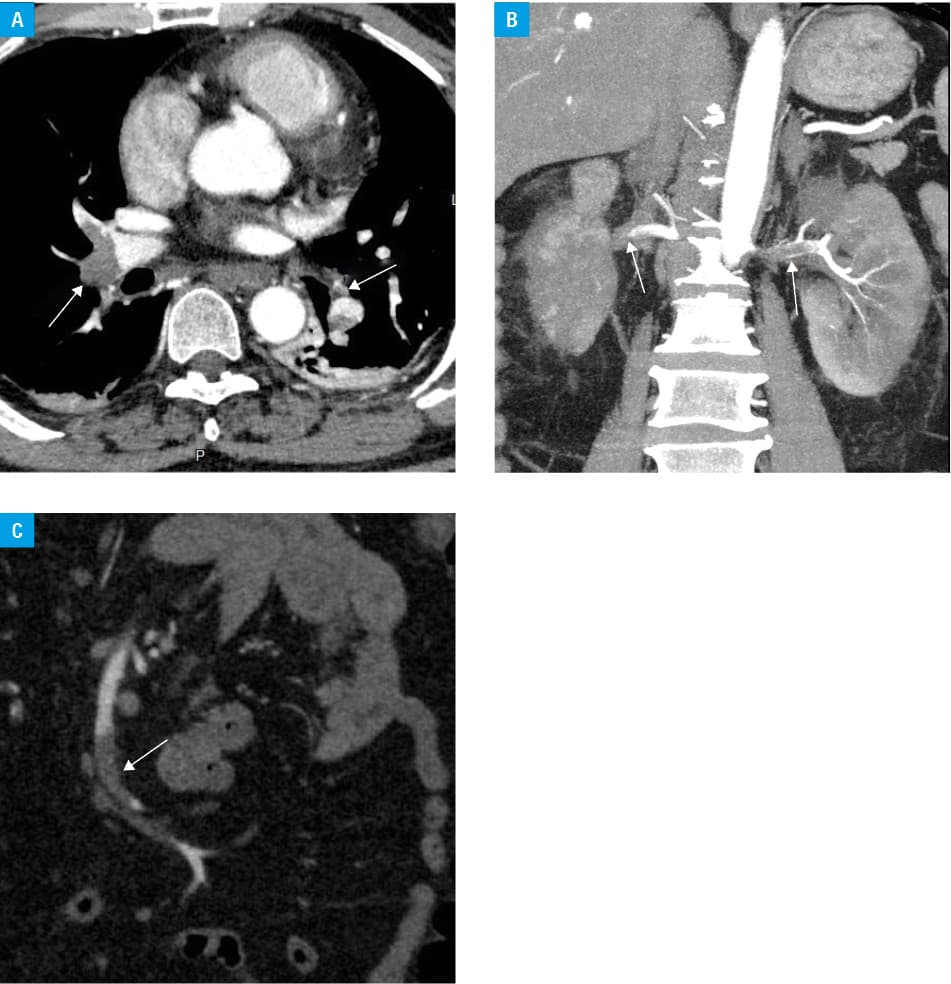
Emergency contrast‑enhanced computed tomography of the aorta showed filling defects in the bilateral pulmonary arteries (Figure 1A), renal arteries (Figure 1B), and superior mesenteric artery branches (Figure 1C). Hence, thrombosis of multiple sites was considered. Subsequently, based on the results of emergency rheumatologic and immunologic examinations, the patient was diagnosed with catastrophic antiphospholipid syndrome (CAPS). He received continuous renal replacement therapy for oliguria. After several consultations and recommendations, he received a hypodermic injection of low‑molecular‑weight heparin sodium daily and an intravenous methylprednisolone pulse of 1 g daily for 3 days. The patient also underwent plasma exchange on alternate days. He received a broad‑spectrum antibiotic for the treatment of systemic inflammatory responses. After 2 weeks, his condition improved significantly. Two months later, the levels of anti‑cardiolipin and anti-β2 glycoprotein antibodies were significantly lower than before but remained higher than normal. Moreover, his renal function did not recover, and he still presented with oliguria and needed to receive regular hemodialysis.
Antiphospholipid syndrome (APS) is an autoimmune systemic disorder that may be associated with an increased risk of thrombosis and the presence of antiphospholipid antibodies.1 CAPS is a lethal systemic disease occurring in approximately 1% of patients with APS.2 Patients with CAPS present with the following: 1) clinical signs of multiple (3 or more) organ failure progressing within an extremely short period, 2) histopathologic evidence of multiple small vessel occlusions, 3) presence of antiphospholipid antibodies, often represented as high titers in laboratory examinations, and 4) clinical symptoms occurring simultaneously or within the course of 1 week. In our case, the patient met 3 of the above CAPS criteria. Although no biopsy of histopathologic specimen was performed due to the patient’s critical condition, he was diagnosed with CAPS based on the results of the clinical examination. The pathogenesis of CAPS remains largely unclear. It is believed that CAPS is mainly characterized by microvascular thrombosis, which can develop into thrombotic storm and result in rapidly progressing inflammation involving multiple organs.2 Therefore, CAPS should be considered in the differential diagnosis of thrombotic microangiopathy.
The current treatment guidelines recommend antithrombotic and pulse therapy with glucocorticoids as the primary regimen.2 Plasma exchange or intravenous immunoglobulin therapy should be considered in patients with critical illnesses.3 Biological agents, such as rituximab and eculizumab, may be effective in patients with refractory or recurrent CAPS.4
In our case, the patient was promptly diagnosed with CAPS. He then received continuous renal replacement therapy and anticoagulation, antibiotics, and methylprednisolone pulse treatment, and underwent plasma exchange. His condition improved significantly. Most patients with CAPS die of multiorgan failure.4 Unless diagnosed early on, neglected CAPS can lead to disastrous effects. CAPS has a high mortality risk. Therefore, early diagnosis and timely treatment are necessary to achieve good outcomes. However, due to the condition’s rarity, it is extremely difficult for physicians to identify appropriate treatment strategies for CAPS by standard prospective randomized and control research.4 Although our patient required long‑term hemodialysis, he survived CAPS.
In conclusion, patients with CAPS may initially present with severe abdominal pain. CAPS is a rare variant of APS that occurs in less than 1% of patients with APS, with a mortality rate of up to 50%.5 CAPS has a high mortality rate even though intensive and comprehensive treatments are available. Therefore, it should be diagnosed immediately, and the treatment must be timely.
- Sammaritano LR. Antiphospholipid syndrome. Best Pract Res Clin Rheumatol. 2020; 34: 101463. | Crossref
- Cervera R, Rodríguez‑Pintó I, Espinosa G. The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: a comprehensive review. J Autoimmun. 2018; 92: 1‑11. | Crossref
- Rodríguez‑Pintó I, Lozano M, Cid J, et al. Plasma exchange in catastrophic antiphospholipid syndrome. Presse Med. 2019; 48: 347‑353. | Crossref
- Espinosa G, Rodríguez‑Pintó I, Cervera R. Catastrophic antiphospholipid syndrome: an update. Panminerva Med. 2017; 59: 254‑268. | Crossref
- Unlu O, Erkan D. Catastrophic antiphospholipid syndrome: candidate therapies for a potentially lethal disease. Annu Rev Med. 2017; 68: 287‑296. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION