Hemoglobin level as a predictor of major adverse cardiac events during a long-term follow-up in patients with coronary artery disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Hemoglobin level as a predictor of major adverse cardiac events during a long-term follow-up in patients with coronary artery disease
Introduction
Anemia is a common and often underestimated clinical problem in patients with coronary artery disease (CAD), one that can exacerbate angina symptoms due to insufficient blood oxygenation and impaired oxygen supply to the myocardial muscle. In the ARIC (Atherosclerosis Risk in Communities) study,1 which included individuals aged 45 to 64 years from the general population, anemia was found to be an independent cardiovascular risk factor. Anemia was also identified as an independent predictor of cardiovascular events during a short‑term follow‑up (30 days) in patients who had developed acute coronary syndrome (ACS).2 Another parameter, red cell distribution width (RDW; evaluated as RDW coefficient of variation [RDW‑CV]), is a quantitative measure of anisocytosis, reflecting average erythrocyte dispersion. We have previously shown that RDW‑CV is a predictor of death and myocardial infarction (MI) during secondary CAD prevention.3 Also, Tonelli et al4 demonstrated that increasing anisocytosis was associated with major adverse cardiac events (MACEs) in patients with a history of MI.4 However, the published analyses did not include coronary plaque composition, even though the fibrofatty plaque and necrotic core components (together referred to as noncalcified plaque [NCP]) had been linked to the plaque vulnerability, which may be associated with subsequent ACS.5 The present study was intended to investigate the roles of hemoglobin level, RDW‑CV, and plaque composition (including NCP) in MACE prediction among patients with newly diagnosed significant CAD based on computed tomography coronary angiography (CTCA) during a long‑term follow‑up.
Patients and methods
Study population
This was a prospective, single‑center study that included 300 consecutive patients with newly diagnosed CAD based on CTCA. A flowchart and the inclusion / exclusion criteria for the study have been published elsewhere.6 All patients provided their informed consent and the study received Ethics Committee approval (1681). The patients were managed according to the current European Society of Cardiology guidelines, and participation in the study did not influence treatment recommendations.
Laboratory tests
All the patients underwent laboratory investigations (the Central Laboratory in the National Institute of Cardiology) directly after CTCA, including a complete blood count (reference range [RR] for hemoglobin, 11.2–15.7 g/dl in women and 13.7–17.5 g/dl in men), iron (RR, 33–193 µg/dl), vitamin B12 (RR, 197–771 pg/ml), folic acid (RR, 4.6–18.7 ng/ml), creatinine (RR, 0.5–0.9 mg/dl in women and 0.7–1.2 mg/dl in men), high‑sensitivity C‑reactive protein (hsCRP; RR <0.5 mg/dl), and a complete lipid profile evaluation. Anisocytosis was considered to be present when RDW‑CV values were above the upper limit of normal (11.7%–14.4% for women and 11.6%–14.4% for men).
Follow‑up and study outcomes
Medical history data were obtained via interviews with the patients and from the medical documentation. The follow‑up data were collected during outpatient visits or using a standardized telephone questionnaire. They were gathered regularly at the first and second year after CTCA. An additional follow‑up checkup was performed for all the patients in January 2022.
The primary study outcome was the occurrence of MACEs. This outcome was a composite of death, nonfatal MI, and revascularization due to CAD progression, as confirmed via invasive angiography.7 Of the enrolled patients, 18 underwent elective coronary artery bypass grafting, and 65 underwent elective percutaneous coronary interventions as a result of index angiography after CTCA. The remaining patients were managed conservatively based on their clinical status and the functional ischemia test results. These procedures were not counted as events.
Computed tomography coronary angiography analysis
CTCA analyses were performed in our core laboratory by an experienced reader (at least 10 years of experience with CTCA) blinded to the clinical and laboratory data. A QAngioCT analysis (Medis Medical Imaging Systems, Leiden, the Netherlands) was performed by a blinded, professionally trained reader.
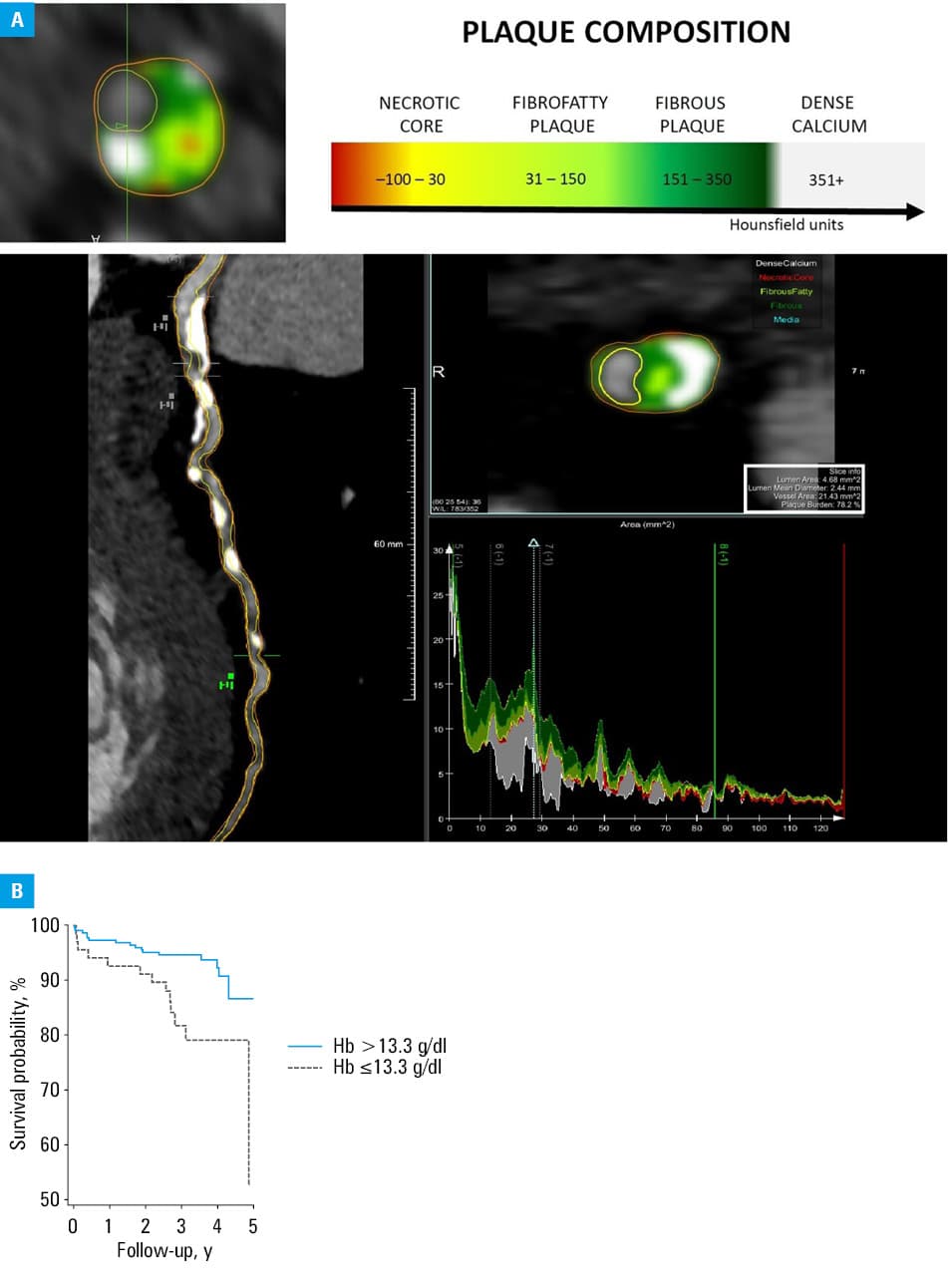
Coronary stenosis was categorized as minimal (<25%), mild (25%–49%), moderate (50%–69%), or severe (70%–100%). In the study population, the composition of atherosclerotic plaques was evaluated. The atheroma composition was determined based on tissue attenuation ranges (in Hounsfield units) for the following plaque components: dense calcium, fibrous plaque, fibrofatty plaque, and necrotic core (Figure 1A).8,9 The sum of the values for the fibrofatty plaque and necrotic core was calculated and referred to as NCP.10 Atheroma components were expressed as percentages (normalized to the vessel volume).
Statistical analysis
The study size calculation results were published before along with the study protocol.6 Continuous data with normal distribution are presented as means (SD). Non‑normally distributed variables are presented as medians with interquartile ranges (IQRs). Categorical variables are presented as frequencies and percentages. Differences between the study groups were determined using the t test (normal distribution) or the Mann–Whitney test (non‑normal distribution, independent variables). Differences between the qualitative variables were determined using the χ2 test or the Fisher exact test.
The predictive value of each variable was evaluated using the Cox proportional hazards model. The independent effects of the variables on the primary outcome were calculated using the Cox multivariable proportional hazards regression analysis. The cutoff value for hemoglobin was calculated using receiver operating characteristic curve (ROC) analysis (DeLong et al11). Kaplan–Meier curves were plotted for the primary study outcome. A P value below 0.05 was considered significant. All analyses were performed using MedCalc software (version 20.011, Ostend, Belgium).
Results
The study included 300 patients (191 men, mean [SD] age, 66 [8] years). Baseline characteristics of the study group are provided in Supplementary material, Table S1. The median total calcium score per patient was 565.2 (IQR, 220.4–988.8). The median dose length product for CTCA was 431.8 mGy × cm (IQR, 346.6–576.2).
The differences in hemoglobin, iron, folic acid, vitamin B12, creatinine, hsCRP, and lipid levels according to sex categories are presented in Supplementary material, Table S2.
Overall, 34 patients (11.3%) had the hemoglobin level under the lower limit of normal. Five individuals had the iron level lower than the RR, and in 4 patients it was above the RR. A total of 56 patients had folic acid deficiency, and 15 had folic acid overload. With respect to vitamin B12, deficiency was found in 18 individuals, and overload in 13. Among the patients with the hemoglobin level under the RR, the most common state was normocytosis, which was observed in 19 patients. Macrocytosis was detected in 14 individuals, and microcytosis in 1. Normochromia was found in 25 patients, hyperchromia in 7, and hypochromia in 2.
A total of 2184 coronary plaques were found on CTCA, of which 1201 (55%) were calcified, 584 (27%) were noncalcified, and 397 (18%) were mixed. Of all the analyzed plaques, 864 caused minimal stenosis, 613 caused mild stenosis, 500 caused moderate stenosis, and 207 caused severe stenosis.
Analysis was performed after a median follow‑up of 3.2 years (IQR, 2.6–4.0). During the follow‑up, the primary outcome was observed in 29 patients, including 19 deaths, 4 nonfatal MIs, and 7 revascularizations due to the progression of CAD, as confirmed by invasive angiography. A single patient experienced 2 events, which were nonfatal MI and, subsequently, death, with only the first event being included in the analysis.
In a univariable regression analysis, the following factors were identified as MACE predictors: hemoglobin level (hazard ratio [HR], 0.69; 95% CI, 0.53–0.88; P = 0.003), percentage of NCP (HR, 0.96; 95% CI, 0.93–1.00; P = 0.03), percentage of the fibrous plaque component (HR, 0.94; 95% CI, 0.90–0.99; P = 0.01), and percentage of the dense calcium plaque component (HR, 1.03; 95% CI, 1.01–1.05; P = 0.01). Sex, age, and CAD risk factors were not identified as MACE predictors (P >0.05 for all). In a multivariable regression analysis, hemoglobin level was an independent MACE predictor (HR, 0.73; 95% CI, 0.54–0.97; P = 0.03), regardless of anisocytosis and the composition of coronary plaques. Complete results of the multivariable analysis are presented in Supplementary material, Table S3. According to the ROC analysis, the cutoff value for hemoglobin was equal to or below 13.3 mg/dl (area under the curve = 0.625; P =0.04). The Kaplan–Meier analysis showed that the patients with the hemoglobin level equal to or below 13.3 mg/dl had a significantly worse outcome than those with the hemoglobin level above the cutoff value (P = 0.002) (Figure 1B).
Discussion
Our study showed that lower hemoglobin levels were an independent predictor of MACEs in the patients with a newly diagnosed significant CAD, regardless of the coronary plaque composition. The fibrofatty plaque and necrotic core, together referred to as NCP, are more likely to evolve into culprit MI lesions than other plaque components, and should be considered high‑risk.12 Higher levels of the fibrofatty plaque were previously revealed to be a MACE predictor in a study investigating 265 diabetic patients, who experienced 63 events, specifically 16 deaths, 3 MIs, 8 unstable anginas, and 36 late nonurgent revascularizations.13 However, in that study, hemoglobin level was not included in the multivariable analysis. Lipid‑lowering treatment could reduce the predictive importance of the fibrofatty plaque component for MACE occurrence during the follow‑up due to the inhibition of coronary plaque progression and, in some cases, potential plaque regression.10
More research is needed to confirm the role of low hemoglobin level and anemia in CAD patients, and to investigate the possible influence of anemia treatment on a patient’s prognosis. In a recent meta‑analysis of 44 studies with 230 795 participants,14 anemia was present in 16% of the patients undergoing PCI, which is in agreement with the results of our study. It seems that anemia is more prevalent in the patients with CAD than in the general population—in the ARIC study,1 9% of adults had anemia. A meta‑analysis by Kwok et al14 showed an elevated risk of MACE with anemia as compared with the no anemia–pooled risk ratio (risk ratio, 2.39; 95% CI, 2.02–2.83; P <0.001 and risk ratio, 1.51; 95% CI, 1.34–1.71; P <0.001, respectively). In another analysis,15 the model including anemia, CAD, kidney dysfunction, and diabetes yielded the best accuracy for predicting the 12‑month rate of composite all‑cause death in patients with heart failure. The results of our study indicate the need to pay attention to the level of hemoglobin and the presence of anemia in the comprehensive management of patients with CAD, regardless of the coronary plaque composition.
The limitations of our study include a single‑center design and the lack of analysis of other blood parameters, that is, total iron binding capacity, ferritin, or transferrin.
In conclusion, a decreased hemoglobin level occurred in about 11.3% of our study patients with newly diagnosed significant CAD diagnosed using CTCA. Hemoglobin level was an independent MACE predictor in the investigated population, regardless of anisocytosis and the composition of coronary atherosclerotic plaques.
- Sarnak MJ, Tighiouart H, Manjunath G, et al. Anemia as a risk factor for cardiovascular disease in the Atherosclerosis Risk in Communities (ARIC) study. J Am Coll Cardiol. 2002; 40: 27‑33. | Crossref
- Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111: 2042‑2049. | Crossref
- Oleksiak A, Kruk M, Lenarczyk E, et al. Biomarkers for risk stratification in secondary cardiovascular prevention. A role of red blood cell distribution width and calcium score. Atherosclerosis. 2016; 246: 57‑62. | Crossref
- Tonelli M, Sacks F, Arnold M, et al. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation. 2008; 117: 163‑168. | Crossref
- Maurovich‑Horvat P, Ferencik M, Voros S, et al. Comprehensive plaque assessment by coronary CT angiography. Nat Rev Cardiol. 2014; 11: 390‑402. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION