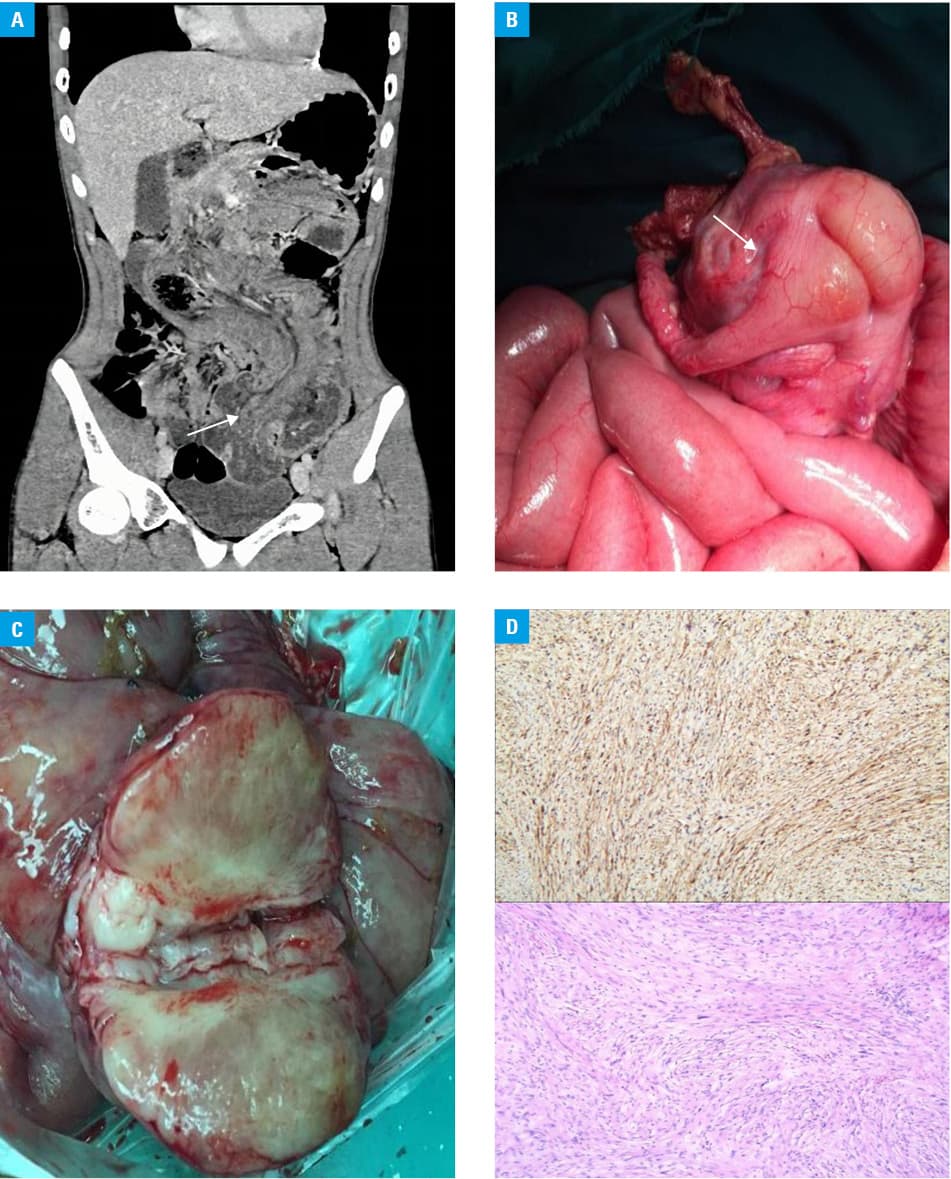
A previously healthy 16‑year‑old boy presented to the emergency department with hematochezia and a 16‑hour history of intense pain in the lower abdomen. He reported intermittent, mild episodes of pain over the previous 6 months. Physical examination revealed diffuse abdominal discomfort with a palpable abdominal mass in the left lower quadrant. The laboratory workup was unremarkable. Computed tomography (CT) showed a long intussusception (Figure 1A). Laparotomy demonstrated an intussusception extending to the sigmoid colon, and a mass was palpated in the area of the sigmoid colon. After reduction of the intussusception, a cecal mass was observed to be the lead point and it was intussuscepted into the sigmoid colon (Figure 1B). Subsequently, oncologic right hemicolectomy was performed, and the size of the mass was 5 cm × 4 cm × 3 cm (Figure 1C). The results of the histologic examination were consistent with a neurofibroma (Figure 1D). A thorough physical examination failed to reveal any clinical signs of neurofibromatosis. A diagnosis of an isolated intestinal neurofibroma was made. The patient remained in a good condition during the 5‑year follow‑up, and showed no systemic signs of neurofibromatosis.
Isolated intestinal neurofibromas are extremely rare, and only 16 cases have been reported in the English research literature to date. The age of diagnosis ranged from 26 to 70 years, and most of the patients were women. Although most cases were incidentally found in asymptomatic patients, the patients may present clinically with abdominal pain, a palpable mass, bloody diarrhea, or obstruction due to an intussusception or the external pressure exerted by the mass.1 Similarly, long‑tract ileocolic intussusception is rarely reported in the available literature. This is the first case report of a long‑tract ileocolic intussusception caused by an isolated intestinal neurofibroma. Abdominal CT is the most accurate diagnostic tool for intussusception but cannot accurately distinguish between benign, malignant, or idiopathic causes.2 The final diagnosis depends on the laparotomy findings and the postoperative pathologic examination. However, there is no consensus on the treatment guidelines for adult intussusception. Due to a high malignancy rate of the pathologic lead point, surgical resection is a suitable choice.3 In addition, the incidence of aggressive tumors developing from a solitary neurofibroma is still unknown. Three cases of malignant transformation from isolated neurofibromas without neurofibromatosis type 1 have been reported, and malignant transformation occurred many years after the initial diagnosis. Therefore, close and regular follow‑up of patients is important.4
In conclusion, isolated enteric neurofibroma‑associated long‑tract intussusception is rare. Abdominal CT is clinically important for the diagnosis, but the final diagnosis depends on postoperative pathologic examination, and regular postoperative follow‑up is mandatory.
- Ghoneim S, Sandhu S, Sandhu D. Isolated colonic neurofibroma, a rare tumor: a case report and review of literature. World J Clin Cases. 2020; 8: 1932‑1938. | Crossref
- Hong KD, Kim J, Ji W, Wexner SD. Adult intussusception: a systematic review and meta‑analysis. Tech Coloproctol. 2019; 23: 315‑324. | Crossref
- Chiu HT, Yen H, Weng YS, et al. Combined ileoileal and ileocolic intussusception secondary to inflammatory fibroid polyp in an adult: a case report. Medicina (Kaunas). 2022; 58: 310. | Crossref
- Adioui T, Tamzaourte M, Nejjari F, et al. Isolated neurofibroma of the sigmoid colon: a case report and review of the literature. J Gastrointest Cancer. 2018; 49: 195‑199. | Crossref
ARTICLE INFORMATION