Diagnosis of splenic cavernous lymphangioma by computed tomography and multimodal magnetic resonance imaging: a comparative analysis of imaging and pathology



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Diagnosis of splenic cavernous lymphangioma by computed tomography and multimodal magnetic resonance imaging: a comparative analysis of imaging and pathology
A 59‑year‑old woman complained of dull pain in the upper abdomen for more than 10 days. A physical examination was unremarkable. Laboratory tests showed normal liver function, blood biochemistry, and α-fetoprotein, carcinoembryonic antigen, and carbohydrate associated antigen 19‑9 levels. A plain computed tomography (CT) scan revealed enlarged and lobulated spleen. Multiple visible cystic lesions of various size with multiple septations were observed, and a small calcified lesion was detected (Figure 1A). Magnetic resonance imaging (MRI) showed that the cystic lesions had low signal intensity on T1 weighted images (T1WI) (Figure 1B), and high signal intensity on fat‑suppressed T2 weighted images (Figure 1C). Some lesions had slightly higher signal intensity on T1WI, and there was no signal reduction on opposed‑phase T1WI, indicating protein deposition or hemorrhage in the cyst. On diffusion‑weighted imaging multi‑b value scans, the lesions changed from high signal intensity to low signal intensity, when the b‑value shifted from 40 to 1200 s/mm2, indicating that the content of the cyst was free water (Figure 1D and 1E). Fibrous septa with mild delayed enhancement were observed within the lesions on the enhanced scan, and solid component enhancement was not detected (Figure 1F).
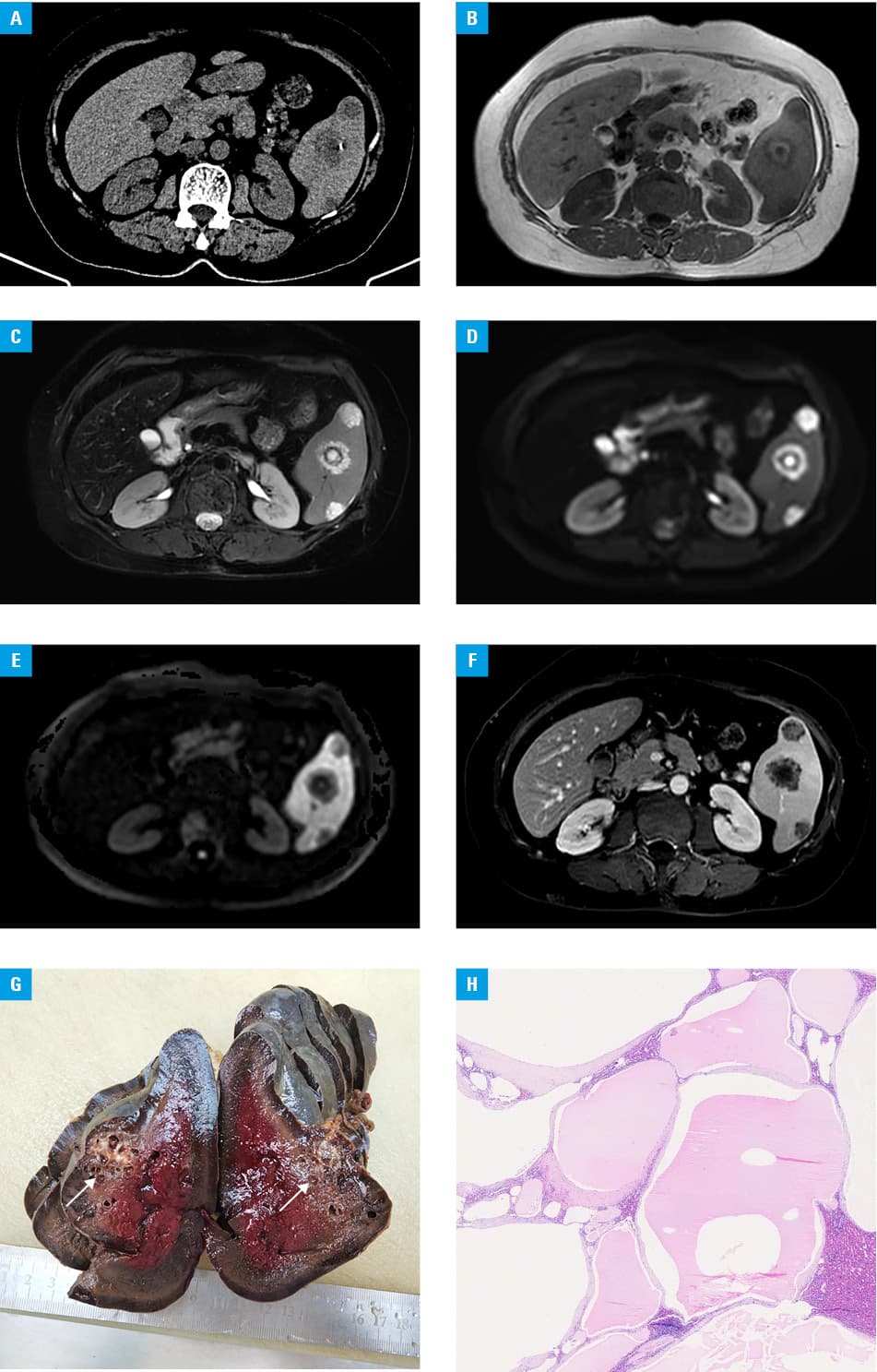
The patient underwent total splenectomy. The cut surface of the spleen tissue was grayish‑brown and spongy, and multilocular lesions adjacent to the splenic capsule were present. The largest lesion was about 3.8 cm in diameter, and grayish‑yellow jelly‑like substances were revealed within the lesions following their partial incision (Figure 1G). Multilocular lesions were filled with clear lymph, and more protein components had jelly‑like texture. The lymphatic vessels showed dilatations of variable size and uneven wall thickness. Some lymphatic vessels were separated by fibrous tissue or residual splenic tissue. The cyst was filled with clear lymph, and hemorrhage and calcification were observed in some lesions (Figure 1H). A diagnosis of cavernous lymphangioma was made.
Lymphangioma is a relatively rare, benign tumor, originating from the lymphatic system.1 Although it can occur in any part of the human body, the splenic localization is rare.2 Surgical resection is the best treatment, and therefore preoperative imaging evaluation is particularly important.3 However, there are only a few publications on preoperative multimodal MRI diagnosis and differential diagnosis of splenic cavernous lymphangioma.4 In the case described here, CT and multimodal MRI helped to accurately identify typical histopathologic features, as described above.5
- Efared B, Atsame‑Ebang G, Zabeirou A, et al. Isolated splenic lymphangioma presenting as a huge mass causing anemia and abdominal distension in an adult patient: a case report. J Med Case Rep. 2018; 12: 97. | Crossref
- Kim SY, Kwon HJ, Park HW, et al. Multiple cystic lymphangiomas of the spleen: radiologic and histopathologic findings. J Med Ultrason. 2015; 42: 409‑412. | Crossref
- Hussein Al‑Janabi M, Abodest R, Adnan Alshabab M, et al. Splenic cystic lymphangioma in adults: a rare case report from Syria. J Ann Med Surg. 2022; 80: 104152. | Crossref
- Perez A, Perez MEC, Yuga AC, Viray BAG. Splenic lymphangioma in adulthood: a case report. J Surg Case Rep. 2020; 67: 250‑253. | Crossref
- Ousmane T, Mamadou FP, Sitor SI, et al. Splenic lymphangioma. J Surg Case Rep. 2019; 62: 40‑42. | Crossref
ARTICLE INFORMATION