A 31‑year‑old non‑smoker with no history of previous abdominal surgery and no family history of genitourinary malignancies underwent an ultrasound screening. The pelvic ultrasound examination unexpectedly revealed a 22 mm × 20 mm hypoechoic lesion closely adhering to the left side of the urinary bladder wall (Figure 1A). Due to the ambiguous ultrasound image, additional diagnostic tests were performed (the differential diagnosis included bladder diverticulum, ureterocele, and tumor). Diagnostic cystoscopy showed a normal bladder mucosa with a visible mass protruding into the bladder lumen (Figure 1B). Due to the unclear view of the lesion, a transvesical biopsy was abandoned. A urine cytological examination was negative for any pathologic findings. Subsequently, contrast‑enhanced pelvic magnetic resonance imaging (MRI) was performed. It visualized an uncharacteristic solid tumor in the minor pelvis, which distorted the lateral wall of the bladder (Figure 1C and 1D). Late contrast enhancement pointed to fibrous tissue within the lesion (an image atypical of bladder tumors and enlarged lymph nodes). Based on the results of MRI and cystoscopy and the absence of a definitive diagnosis, the patient underwent surgical removal of the lesion. Extraperitoneal laparoscopic resection of the tumor was performed (Figure 1E), using a double‑J catheter placed in the left ureter prior to the surgery for identification purposes (the lesion was located about 15 mm distally to the end of the left ureter). Intraoperatively, the solid mass adjacent to the bladder wall was dissected and removed completely (Figure 1F). During gentle preparation, the muscular layer of the bladder wall was visualized. The bladder was tested for water tightness (integrity testing) by instilling 300 ml of saline through a Foley catheter, and as no leakage was found, the bladder repair was unnecessary. The histopathologic evaluation of frozen sections was consistent with bladder leiomyoma (Figure 1G and 1H).
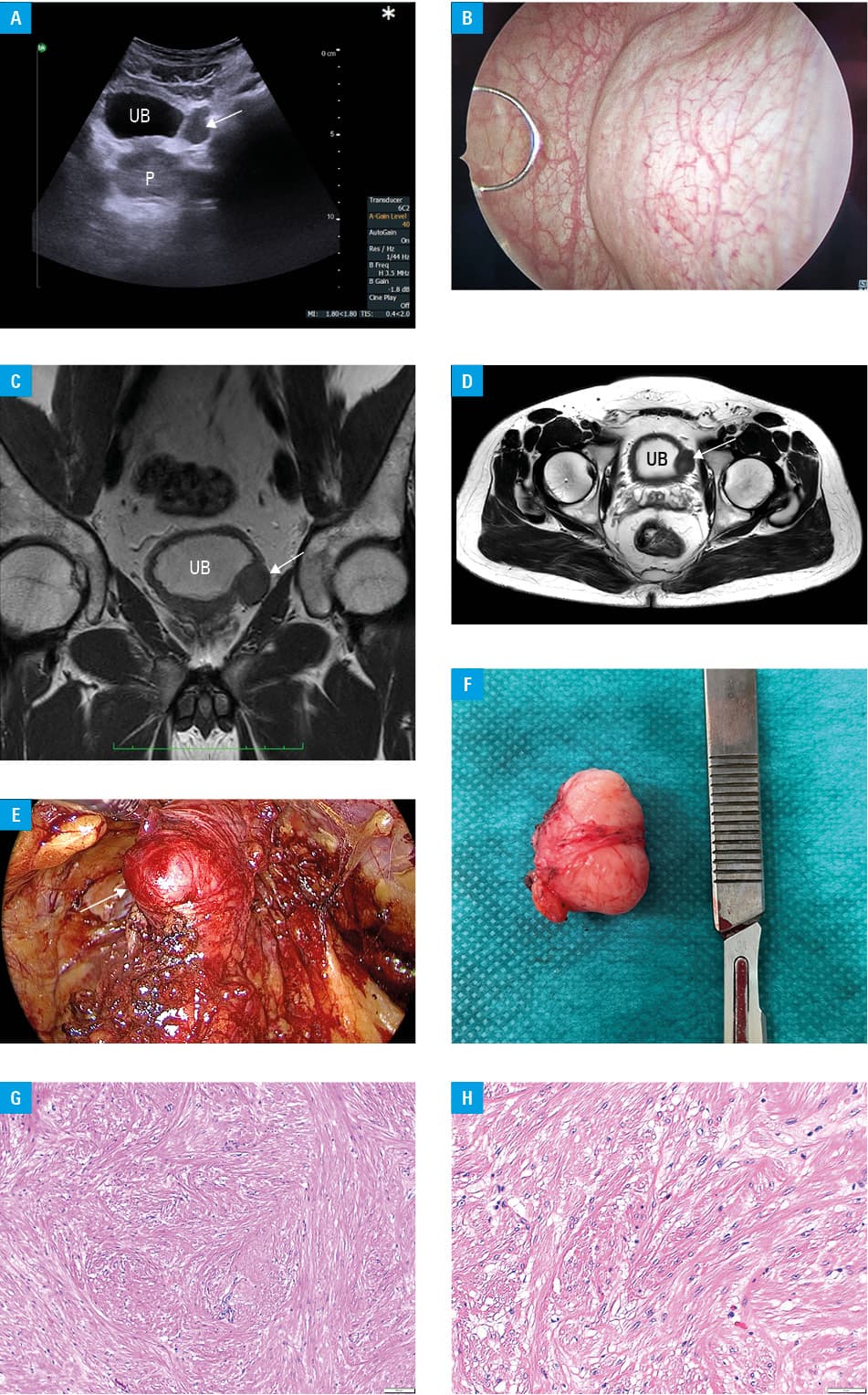
Abbreviations: P, prostate gland; UB, urinary bladder
Urinary bladder leiomyoma is a rare mesenchymal neoplasm representing less than 0.5% of all bladder tumors.1 The average age of presentation has been reported to be over 40 years, with a higher frequency in women. Leiomyomas can present in 3 locations: endovesical, which is the most common one and accounts for 63% to 66% of cases, extravesical found in 11% to 30% of cases, and intramural diagnosed in 3% to 6% of cases.2 MRI evaluations are highly specific for detecting the mesenchymal component of these tumors. Leiomyomas on MRI show low intensity in both T1- and T2‑weighted sequences with a smooth periphery, mimicking a uterine leiomyoma. The endovesical form can cause irritative or obstructive symptoms and gross hematuria, resulting in a relatively early diagnosis.3 Extravesical tumors are usually asymptomatic, similarly to the case presented in this report. Treatment is determined primarily based on the size and anatomical location of the tumors. There are no reports of bladder leiomyomas undergoing malignant transformation. Nevertheless, bladder leiomyomas often mimic malignant tumors and surgical resection with a diagnostic histopathologic examination of the removed tumor is preferred.4 Small endovesical tumors can be treated with transurethral resection of the bladder tumor. However, unfavorable location and difficulty in identifying the tumor may require laparoscopic or robotic resection or even partial cystectomy.5
- Yoshioka T, Kawakita M, Kameoka H. Cystoscope‑assisted laparoscopic enucleation of a large progressive bladder leiomyoma. J Endourol Case Rep. 2019; 5: 120‑123. | Crossref
- Goluboff ET, O’Toole K, Sawczuk IS. Leiomyoma of bladder: report of case and review of literature. Urology. 1994; 43: 238‑241. | Crossref
- Nazih K, Ghazi S. Bladder leiomyoma: presentation, evaluation and treatment. Arab J Urol. 2013; 11: 54‑61. | Crossref
- Park JW, Jeong BC, Seo SI, et al. Leiomyoma of the urinary bladder: a series of nine cases and review of the literature. Urology. 2010; 76: 1425‑1429. | Crossref
- Lyons TL, Lee T, Winer WK. Laparoscopic removal of a bladder leiomyoma. J Am Assoc Gynecol Laparosc. 1998; 5: 423‑426. | Crossref
ARTICLE INFORMATION