Saddle pulmonary embolism as a fatal complication of Cushing syndrome: a call for standardized anticoagulation regimen in hypercortisolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Saddle pulmonary embolism as a fatal complication of Cushing syndrome: a call for standardized anticoagulation regimen in hypercortisolism
Cushing syndrome (CS) is associated with a 18‑fold higher risk of venous thromboembolism (VTE).1 Although the issue of hypercoagulability in CS is getting more and more attention, a consensus regarding the timing and dosing of thromboprophylaxis in hypercortisolism is currently lacking.2
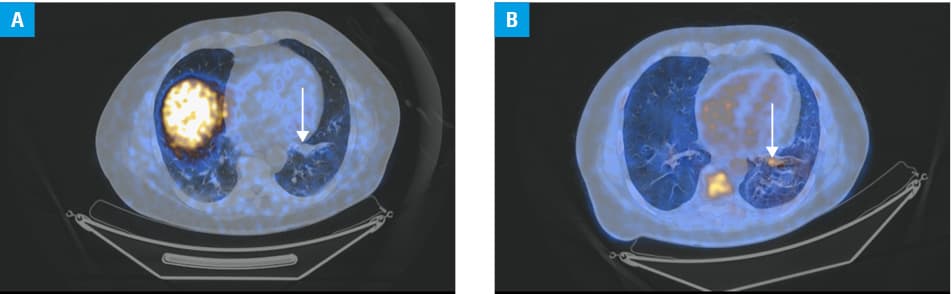
We present a case of a 51‑year‑old man with type 2 diabetes mellitus, hypertension, and liver steatosis who was admitted to the Emergency Department due to confusion and fatigue. Laboratory test results demonstrated severe hypokalemia (up to 1.7 mmol/l; reference range [RR], 3.5–5.10 mmol/l), which was refractory to treatment. Thromboprophylaxis (40 mg enoxaparin subcutaneously once daily) and a liver protection agent were introduced. Hormone test results showed an increased morning serum cortisol level (88.6 µg/dl; RR, 6.24–18 µg/dl); however, there were no classic physical signs of CS. The patient was transferred to the Department of Endocrinology. Biochemical workup revealed affected circadian cortisol rhythm with an elevated level of midnight cortisol (7 AM, 28.7 µg/dl; 5 PM, 24.3 µg/dl; 12 AM, 15 µg/dl), elevated level of adrenocorticotropic hormone (138.2 pg/ml; RR, 6–56 pg/ml), and an unsuppressed cortisol level in the 8‑mg dexamethasone suppression test (20.1 µg/dl), indicating ectopic CS. Due to psychosis, treatment with risperidone was introduced. Metyrapone (initial dose, 500 mg/day; final dose, 2500 mg/day) was also implemented, leading to biochemical and clinical improvement. Abdominal ultrasound confirmed liver steatosis, while a chest computed tomography (CT) scan showed a contrast‑enhanced nodule sized 17 mm × 14 mm in the lateral basal segment of the left lung. Neither gallium‑68 (Figure 1A) nor fluorine‑18 fluorodeoxyglucose positron emission tomography / CT (Figure 1B) showed typical pathological accumulation of the tracer indicating a high expression of somatostatin receptors. On the 21st day of hospitalization the patient’s condition suddenly deteriorated, leading to cardiac arrest with pulseless electrical activity. Despite cardiopulmonary resuscitation, the patient died. The postmortem examination revealed saddle pulmonary embolism and a multifocal neuroendocrine tumor grade 1, corresponding with the location of uncharacteristic tracer enhancement in the imaging studies.
This case describes a fatal thrombotic complication in a patient with CS on thromboprophylaxis. The current expert opinion suggests that either preventive or therapeutic dosage of heparin should be considered in patients with ectopic CS.3 Future studies should clarify the ways to decide which one is appropriate, for example, by means of assessing the utility of routine CT pulmonary angiography in this subpopulation of CS patients. Of note, the thrombotic event did not manifest during the severe hypercortisolemia but in the cortisol nadir, following metyrapone implementation. This is in line with a previous report showing that the risk of a VTE event in CS is the highest within 2 months from transsphenoidal surgery or adrenalectomy.4 Since cortisol exerts an anti‑inflammatory effect, its sudden drop might increase the proportion of proinflammatory factors, rendering a thrombotic event more probable.1
The presented case underlines the importance of extending our knowledge about hypercoagulability in hypercortisolism and proposing clear recommendations in this regard.
- Wagner J, Langlois F, Ting Lim DS, et al. Hypercoagulability and risk of venous thromboembolic events in endogenous Cushing’s syndrome: a systematic meta‑analysis. Front Endocrinol (Lausanne). 2019; 9: 805. | Crossref
- van Haalen FM, Kaya M, Pelsma ICM, et al. Current clinical practice for thromboprophylaxis management in patients with Cushing’s syndrome across reference centers of the European Reference Network on Rare Endocrine Conditions (Endo‑ERN). Orphanet J Rare Dis. 2022; 17: 178.
- Young J, Haissaguerre M, Viera‑Pinto O, et al. Cushing’s syndrome due to ectopic ACTH secretion: an expert operational opinion. Eur J Endocrinol. 2020; 182: R29‑R58. | Crossref
- Suarez MG, Stack M, Hinojosa‑Amaya JM, et al. Hypercoagulability in Cushing syndrome, prevalence of thrombotic events: a large, single‑center, retrospective study. J Endocr Soc. 2019; 4: bvz033. | Crossref
ARTICLE INFORMATION