Atherosclerotic renovascular disease and cardiovascular risk: new concepts
Key words: atherosclerotic renal artery stenosis, cardiovascular risk, ischemic nephropathy, renovascular hypertension



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atherosclerotic renovascular disease and cardiovascular risk: new concepts
Renal vascular hypertension (RVHT) is one of the most common secondary forms of hypertension. It is estimated that 1% to 5% of all cases of hypertension can be attributed to RVHT. RVHT is generally caused by progressive stenosis of the renal artery most often due to atherosclerosis, and less often caused by fibromuscular dysplasia. Atherosclerotic renal artery stenosis (ARAS) can lead to the development of resistant hypertension and can also cause progressive impairment of renal function. ARAS can also result in serious cardiac complications, such as flash pulmonary edema or congestive heart failure. Most patients with ARAS are characterized by the presence of left ventricular hypertrophy and diastolic dysfunction. The disease progression is associated with an increase in left ventricular mass index and cardiac dilatation. Atherosclerotic renovascular disease is recognized as a relevant risk factor for cardiovascular morbidity and mortality. Studies published so far documented ARAS as a predictor of higher cardiovascular risk and showed that mortality after incidental ARAS diagnosis is much higher than that observed in the general population. Proper recognition of the patients with ARAS who would benefit from interventional treatment is crucial, particularly for identification of patients with true resistant hypertension, flash pulmonary edema, and progressive impairment of renal function.
Introduction
Renal vascular hypertension (RVHT) is one of the most common secondary forms of hypertension. It is estimated that 1% to 5% of all cases of hypertension can be attributed to this condition. The prevalence may reach up to 6.8% in the older population (>65 years).1-3 RVHT is generally caused by progressive stenosis of the renal artery most often due to atherosclerosis, and less often due to fibromuscular dysplasia.4 The remaining rare or very rare causes, that is, consequences of other stenotic lesions, vascular malformations, or thrombotic complications may also be responsible for development of RVHT.5
Atherosclerotic renal artery stenosis (ARAS) accounts for approximately 90% to 95% percent of cases of renal artery stenosis (RAS) and is predominantly seen in the populations with other cardiovascular risk factors or atherosclerotic lesions in other vascular beds. The prevalence of ARAS increases with age, particularly in the patients with a history of smoking, hypertension, diabetes, peripheral artery disease, or coronary artery disease (CAD).6-8 ARAS is usually localized in the ostium and proximal third of the main renal artery, and sometimes the atherosclerotic plaque may extend into the renal artery. ARAS can affect one or both renal arteries, and at more advanced stages segmental and diffuse intrarenal atherosclerosis develops, predominantly in the patients with ischemic nephropathy.1-3 ARAS can lead to the occurrence of resistant hypertension and can progressively impair the renal function. ARAS can cause serious cardiac complications, such as flash pulmonary edema or congestive heart failure (HF).1-3
ARAS is a multifaceted disease due to the complex interplay between RAS, hypertension, and renal excretory dysfunction. The disease may present as isolated anatomical RAS or may be accompanied by renal insufficiency and / or hypertension.2 It should be considered that in a subset of patients with ARAS essential hypertension develops, and in those patients blood pressure levels are not augmented by the atherosclerotic lesion itself.2
Atherosclerotic renal artery stenosis and cardiovascular disease burden
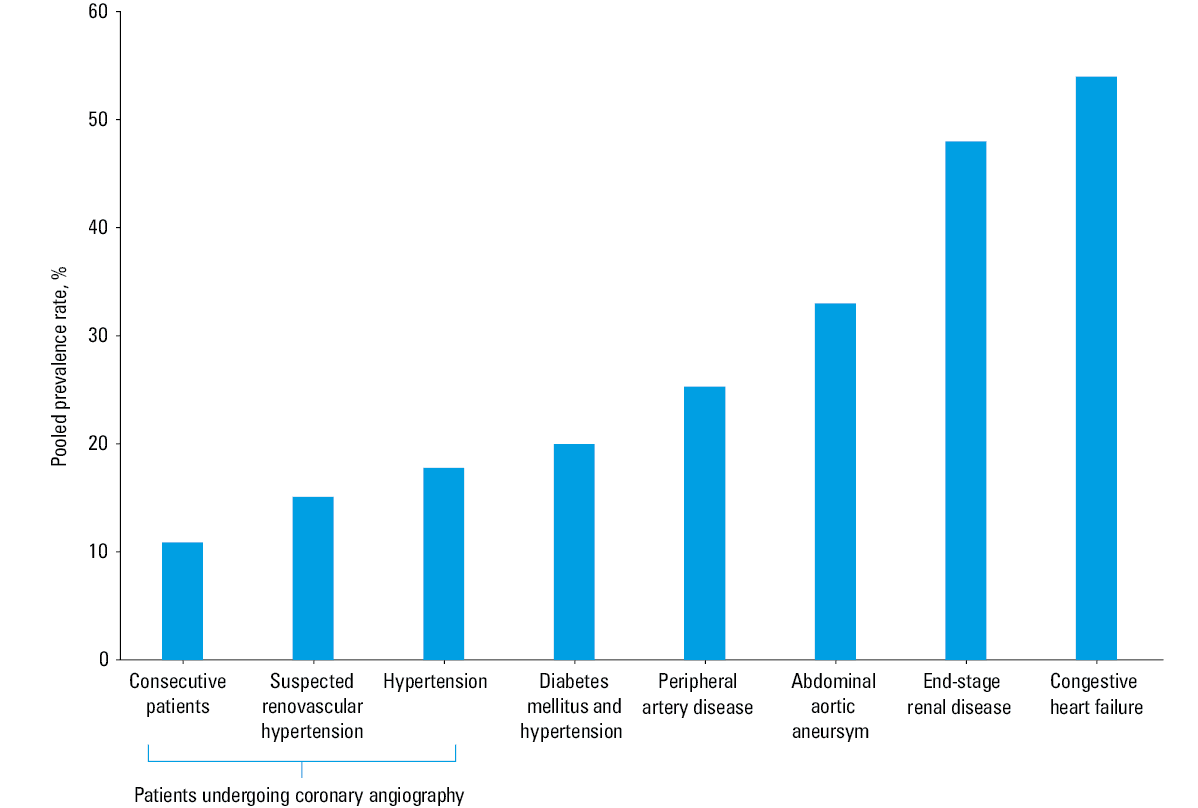
The prevalence of ARAS increases with age and also in patients with cardiovascular risk factors or atherosclerosis. ARAS prevalence ranges from 30% among patients with coronary artery disease to 50% in elderly patients or in those with atherosclerotic lesions in different vascular territories.1-3 Several reports have emphasized the common association of ARAS with documented CAD, and studies based on series of clinically selected groups indicated the prevalence of ARAS at 11% to 18%.1-3 In the studies of Weber‑Mzell et al9 and Harding et al11 performed in the cohorts of patients undergoing cardiac catheterization for suspected CAD, ARAS (defined as renal artery stenosis >50%) was found in 10.7% and 11% of patients, respectively. In the study by Rihal et al,12 which included 297 individuals who underwent coronary angiography, RAS of 50% or more was found in 9.2% of patients.
In a classic study of Buller et al,10 the prevalence and severity of RAS in patients undergoing cardiac catheterization was also established. To be included to the study, the patients had to exhibit at least 1 of the 4 predefined selection criteria, that is, severe hypertension, a history of acute pulmonary edema, unexplained renal dysfunction, or severe atherosclerosis. In this selected population, angiographic ARAS above 50% and above 70% were found in 14.3% and 7.3% of CAD patients, respectively.10
Subsequent studies investigated the relationship between the presence of ARAS and clinical characteristics of the patients. The paper by Dzielińska et al13 documented the presence of ARAS above 50% in 12% of patients who underwent cardiac catheterization for suspected CAD. The number of coronary arteries stenoses, carotid intima‑media thickness, body mass index, creatinine concentration, and the number of antihypertensive drugs were independently associated with the presence of ARAS in this work. Also, the number of coronary arteries with stenotic lesions and serum creatinine level predicted the presence of significant RAS.13
Independently from the ARAS and CAD association, data from other studies also showed high prevalence of ARAS in patients with end‑stage renal disease, peripheral artery disease, and congestive HF.2 In a systematic literature review, de Mast et al14 documented high ARAS prevalence in risk groups, especially in the patients with extrarenal atherosclerosis, HF, and end‑stage kidney disease (Figure 1).
In conclusion, it should be noted that ARAS is more frequent in the patients with high cardiovascular risk (eg, those with diabetes or impaired kidney function). The frequency of ARAS also correlates with the severity of atherosclerosis in other vascular beds.
Atherosclerotic renal artery stenosis as a progressive disease
ARAS is a progressive disease (Figure 2), particularly in the patients with other manifestations of atherosclerosis and / or type 2 diabetes.2 Data on ARAS progression are inconsistent, indicating high rates of progression of renovascular disease with annual occlusion rate of 5%. In another study in the group of patients with ARAS, progressive stenosis was reported in 51% of the renal arteries 5 years after ARAS diagnosis.15
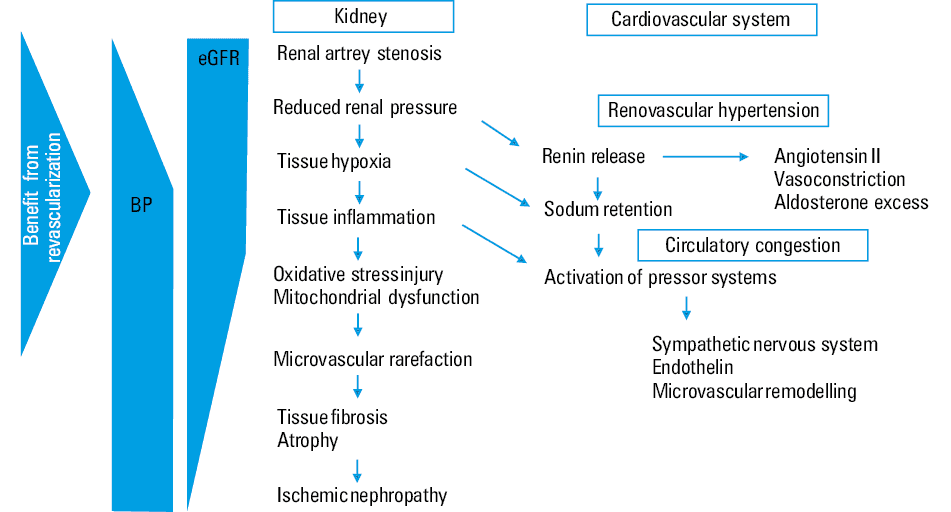
Abbreviations: BP, blood pressure; eGFR, estimated glomerular filtration rate
In contrast with all earlier retrospective studies, the Cardiovascular Health Study2 demonstrated in the 8‑year follow‑up that ARAS progressed in only 14% of kidneys with annualized rate of 1.3%. Progression to significant RAS was observed in only 4% of patients, and in none of the elderly participants a total occlusion was found.2 Also, in a cohort of 1189 patients who underwent cardiac catheterization, progression of ARAS was observed in 11.1% of the patients, and in only 0.3% it led to the renal artery occlusion, which may be explained by the routine statin therapy in these individuals.16
Under experimental conditions, statins have been shown to modify macro- and microvascular circulation of the kidneys and to limit fibrosis and inflammation.16 Also, clinical observations in patients with severe ARAS undergoing stent placement indicated significant benefits of renal protection during intensive lipid lowering, as compared with a conventional therapy.16
In summary, ARAS is a progressive disease, but contrary to the results of early studies showing a significant rate of its progression, recent studies documented delayed development and slower progression of atherosclerotic lesions in renal arteries.
Cardiac structural and functional abnormalities associated with atherosclerotic renal artery stenosis
Excessive amounts of angiotensin II in patients with RVHT exert deleterious effects on the heart. When untreated, ARAS causes not only more cardiac damage than essential hypertension, but is associated with greater morbidity and mortality.17 It has been reported that in the patients not receiving dialysis therapy, ARAS is associated with a 50% increase in mortality rate as compared with other causes of chronic kidney disease (CKD). In the patients on dialysis, the mortality rate for ARAS is over 3 times higher than in those with CKD from other causes.18
Most patients with ARAS are characterized by the presence of left ventricular hypertrophy and diastolic dysfunction. The disease progression is associated with an increase in left ventricular mass index (LVMI) and cardiac dilatation.2,15 The cross‑sectional echocardiographic study of Wright et al,19 which included 79 patients with ARAS and chronic kidney disease, documented that only 5.1% of the patients had no structural and functional cardiac abnormalities. The patients included in that study were characterized by higher prevalence of left ventricular hypertrophy (LVH) than the patients with other causes of CKD (control group) (78.5% vs 46%). Of note, LVH was more pronounced in the individuals with bilateral than unilateral ARAS.2,15,19
A meta‑analysis by Cuspidi et al,20 which included 726 patients (13 studies) with hypertension and ARAS (90%), showed that renal artery revascularization supplementing the antihypertensive therapy had a favorable effect on left ventricular (LV) structure, as documented by a decrease in LVMI and in the likelihood of LVH by 40%. The study of Khangura et al21 highlighted the difference in the pattern of LV geometry between ARAS patients with preserved or impaired renal function and individuals with primary hypertension. In the patients with ARAS and preserved renal function or in those with ARAS and renal dysfunction, concentric and eccentric LVH was more frequent than in the patients with primary hypertension.21
The study of Wright et al19 also showed that the patients with ARAS and CKD were characterized by higher prevalence of LV diastolic dysfunction (40.5% vs 12.0%) than individuals with other causes of CKD (control group).
The association between LV diastolic dysfunction and ARAS‑related CKD persisted after adjusting for age, sex, baseline BP levels and kidney function, diabetes mellitus, smoking status, and the use of statins.2,15 Also, Ghanami et al22 found that diastolic dysfunction was frequent (61.8%) in the patients with ARAS who underwent revascularization, and was associated with increased mortality during follow‑up.
The prevalence of ARAS in patients with congestive HF is high. In 1 study, including patients aged 70 years or older presenting with NYHA class II–III HF, ARAS was found in 34% of cases. In a systematic literature review by de Mast et al23 the pooled prevalence rate of ARAS was 54.1% in the patients with HF.
In 1988, Bloch et al24 described a series of 11 patients with hypertension with bilateral ARAS, who manifested recurrent episodes of pulmonary edema. In 77% of cases successful revascularization improved the clinical course and eliminated pulmonary edema.23
This unique clinical entity, also known as flash pulmonary edema (FPO) or the Pickering Syndrome, describes acute decompensated HF in patients with bilateral or unilateral ARAS triggered by defective natriuresis (with sodium and fluid retention) and increased LV end‑diastolic pressure as underlying pathophysiological mechanisms.
In summary, in ARAS, hemodynamic overload resulting from markedly elevated blood pressure (BP) and augmented activation of the systemic renin‑angiotensin‑aldosterone system impairs cardiac structure and function. Moreover, the patients with ARAS are characterized by more enhanced coronary atherosclerosis, as compared with hypertensive patients without ARAS, which may also result in alteration of cardiac structure and function.17
Atherosclerotic renal artery stenosis and cardiovascular outcomes
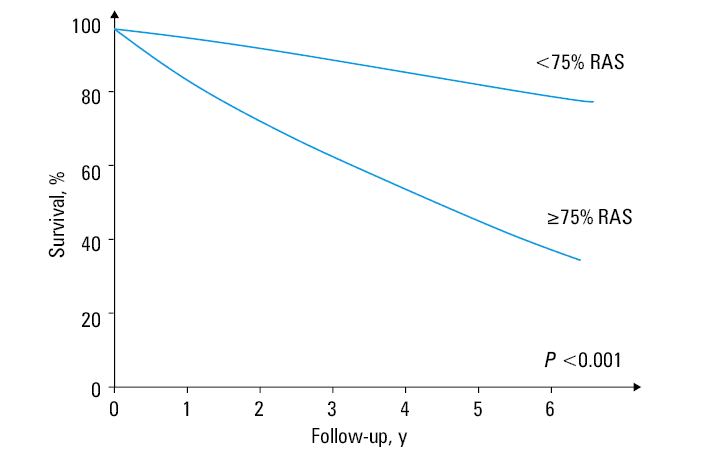
Several lines of evidence indicate that ARAS is a predictor of a poor cardiovascular prognosis and carries a high risk of morbidity and mortality. Cardiovascular complications of ARAS include stroke, myocardial infarction, and congestive HF.2,15 Conlon et al25 studied 3987 patients who underwent renal angiogram during diagnostic cardiac catheterization, and found that the individuals with incidentally discovered ARAS had a much worse prognosis than those with no renal narrowing (Figure 3). In addition, increasing severity of ARAS was associated with an incremental increase in mortality, that is, 4‑year survival of patients without RAS was 89%, while in people with 50% to 75%, 75% to 95% and over 95% ARAS, survival was 70%, 68%, and 48%, respectively. The hazard ratio for 4‑year mortality was 2.01 for the patients with a diagnosis of ARAS after adjustments for the degree of RAS, age, and associated comorbidities.25
Similar data linking ARAS to cardiovascular morbidity and mortality are available for other cardiovascular diseases.2,15 The prognostic impact of incidental ARAS on mortality was studied in a single clinical center (between 1997 and 2000) in 491 consecutive patients who underwent angiography for peripheral vascular disease. RAS higher than 50% was present in 26% of the patients, and mortality was 59% vs 28% in the non‑ARAS group.26 In the same study, ARAS was an independent predictor of mortality along with age, diabetes mellitus type 2, smoking, previous myocardial infarction, stroke, and a history of peripheral artery disease.
In summary, several studies published so far confirmed ARAS as a predictor of poor cardiovascular prognosis and demonstrated that both cardiovascular and renal morbidity and mortality after incidental ARAS diagnosis are much higher than in the general population.
Atherosclerotic renal artery stenosis, renal revascularization and cardiovascular outcomes
Results of several randomized controlled studies have questioned the value of routine revascularization for ARAS, since the latter was not associated with improved cardiovascular outcomes when compared with medical therapy alone.27 In the ASTRAL (Angioplasty and Stenting for Renal Artery Lesions) trial, comparing medical therapy with stenting for ARAS in randomly assigned 806 patients, there was no difference in the pre‑established outcomes of renal function decline, renal events, cardiovascular events, or death.27,28 Also, in the CORAL (Cardiovascular Outcomes in Renal Atherosclerotic Lesions) trial, which enrolled 931 patients with ARAS, there were no differences in primary outcomes including major cardiovascular events (myocardial infarction, stroke, hospitalization for HF, or cardiovascular death), kidney events, or a composite outcome.27,29
These negative results of the ASTRAL and CORAL studies led to the widespread opinion that renal artery intervention in patients with ARAS is not beneficial in the long‑term follow‑up. However, these data are conflicting with further observational studies demonstrating that successful restoration of blood flow may reverse complications of untreated ARAS, such as resistant hypertension or ischemic nephropathy.27,30-32
In a retrospective, uncontrolled single center study, interventional treatment in patients with ARAS and true resistant hypertension significantly lowered diastolic ambulatory BP and reduced the need for antihypertensive treatment without affecting renal function.33 Also, a prospective, longitudinal observational study at a single clinical center indicated that revascularization of ARAS in the patients with HF was associated with substantial reduction in all‑cause mortality and hospitalization rate.34-36
In summary, proper recognition of patients with ARAS (Figure 2) who may benefit from interventional treatment is crucial, particularly for identification of patients with true resistant hypertension, flash pulmonary edema, and progressive deterioration of kidney function.
- Herrmann SM, Textor SC. Current concepts in the treatment of renovascular hypertension. Am J Hypertens. 2018; 31: 139‑149. | Crossref
- Safian RD, Textor SC. Renal‑artery stenosis. N Engl J Med. 2001; 344: 431‑442. | Crossref
- Textor SC. Management of renovascular hypertension. Curr Opin Cardiol. 2020; 35: 627‑635. | Crossref
- Warchol‑Celinska E, Prejbisz A, Dobrowolski P, et al. Systematic and multidisciplinary evaluation of fibromuscular dysplasia patients reveals high prevalence of previously undetected fibromuscular dysplasia lesions and affects clinical decisions: the ARCADIA‑POL Study. Hypertension. 2020; 75: 1102‑1109. | Crossref
- Persu A, Canning C, Prejbisz A, et al. Beyond atherosclerosis and fibromuscular dysplasia: rare causes of renovascular hypertension. Hypertension. 2021; 78: 898‑911. | Crossref
ARTICLE INFORMATION