Atypical hemolytic-uremic syndrome due to scleroderma renal crisis treated with eculizumab



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atypical hemolytic-uremic syndrome due to scleroderma renal crisis treated with eculizumab
Systemic sclerosis (SSc) is a systemic disease with an insidious course and serious complications.1 The most dangerous manifestation of kidney involvement in SSc is scleroderma renal crisis (SRC), which is characterized by acute kidney injury (AKI) and a sudden increase in blood pressure, sometimes also accompanied by microangiopathic hemolysis.2 It has been suggested that SRC may lead to the activation of the complement system; therefore, it may be assumed that eculizumab can be a successful treatment of this condition.3
A 46‑year‑old man was hospitalized due to atypical chest pain. During the diagnostic evaluation, cardiac magnetic resonance imaging findings suggested acute myocarditis of a viral etiology (Figure 1A). Additional tests were performed due to eosinophilia, and the results of high‑resolution computed tomography (HRCT) of the chest raised suspicions of eosinophilic granulomatosis with polyangiitis (EGPA) (Figure 1B). Because of the increasing eosinophil count, further worsening of the renal function, and the overall poor clinical condition of the patient, a hematology consultation was scheduled, and it was decided to start a therapy with an oral steroid (prednisone 0.5 mg/kg). Due to the suspicion of progressive anemia and thrombocytopenia in the course of thrombotic microangiopathy (TMA), a therapy with freshly frozen plasma (FFP) and pulses of methylprednisolone was initiated. Since an increase in renal parameters and features of TMA were noted, plasmapheresis using FFP was performed, and after the second exchange the patient’s general condition deteriorated, showing overhydration, further worsening of the laboratory test results, and an increase in blood pressure.
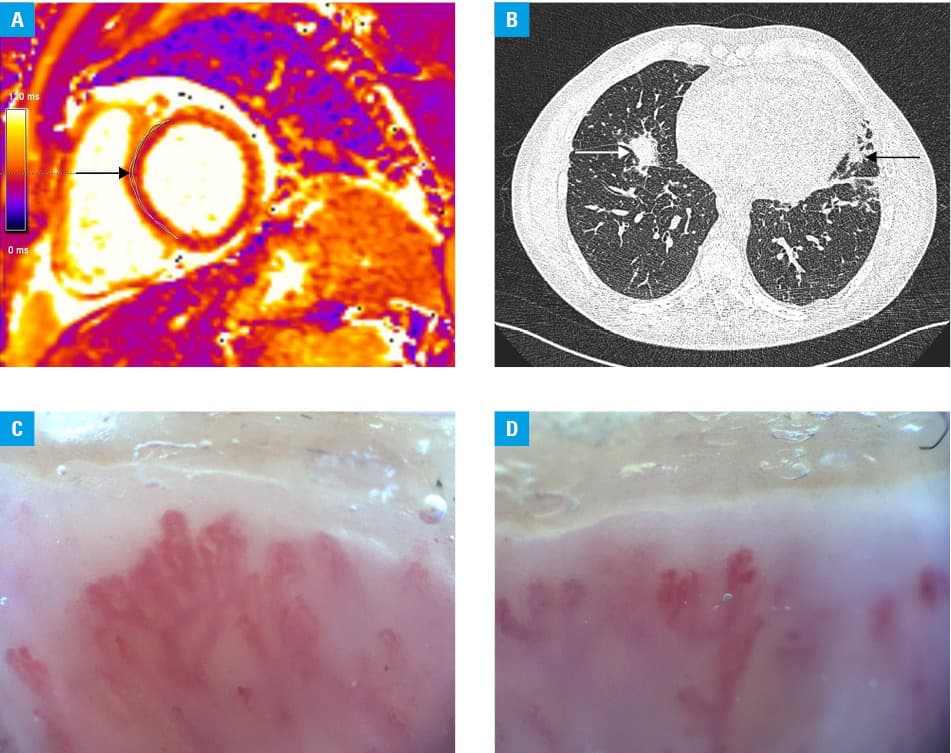
After capillaroscopy (Figure 1C and 1D), a rheumatological consultation, and the result of a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) assay (ADAMTS13 activity of 71%; reference range, 40%–130%; anti‑ADAMTS13 antibody level, 9 U/ml; reference range <12 U/ml), the overall clinical picture allowed for a diagnosis of limited SSc and a suspicion of atypical hemolytic uremic syndrome (aHUS) in the course of SRC. Based on that, the patient was referred for an aHUS treatment program with eculizumab. During the 3‑month treatment, significant improvements in the hemoglobin level and platelet count were observed, along with a reduction in the activity of lactate dehydrogenase. No side effects of the treatment were observed. The patient remains dependent on dialysis. In the genetic testing, variants of complement factor H (heterozygous variant rs2274700) and ADAMTS13 (homozygous variant rs2285489) were found, which may correspond with an increased risk of aHUS and a severe course of the disease.
The role of the complement system in SSc and SRC remains unclear. Corticosteroids were used in our patient, leading to a deterioration of the general condition. However, the signs of TMA were noted before the administration of prednisone. Nevertheless, the diagnosis of SSc was difficult due to the atypical course o the disease. The patient never noticed Raynaud syndrome, and the musculoskeletal symptoms were considered to be related to his past as a sportsman. Also, eosinophilia and HRCT imaging findings suggested the presence of EGPA. The usual treatment of TMA was unsuccessful, and the administration of eculizumab led to immediate improvement, with no side effects observed. Studies on the use of eculizumab in SRC have several limitations, such as the small number of patients, lack of a control group, and coexisting effects of other drugs which are also used due to the life‑threatening condition of the patients.4 Our patient is still dialysis‑dependent, and he will be placed on the transplantation waiting list.
In the cases of severe SRC complicated with TMA, eculizumab treatment can be life‑saving; however, further studies in this area are needed.
- Smoleńska Ż, Gogulska Z, Dorniak K, Zdrojewski Z. Successful treatment of systemic sclerosis coexisting with smoldering myeloma. Pol Arch Intern Med. 2021; 131: 16133. | Crossref
- Penn H, Howie AJ, Kingdon EJ, et al. Scleroderma renal crisis: patient characteristics and long‑term outcomes. QJM. 2007; 100: 485‑494. | Crossref
- Devresse A, Aydin S, Le Quintrec M, et al. Complement activation and effect of eculizumab in scleroderma renal crisis. Medicine (Baltimore). 2016; 95: e4459. | Crossref
- Gouin A, Ribes D, Colombat M, et al. Role of C5 inhibition in idiopathic inflammatory myopathies and scleroderma renal crisis‑induced thrombotic microangiopathies. Kidney Int Rep. 2021; 6: 1015‑1021. | Crossref
ARTICLE INFORMATION