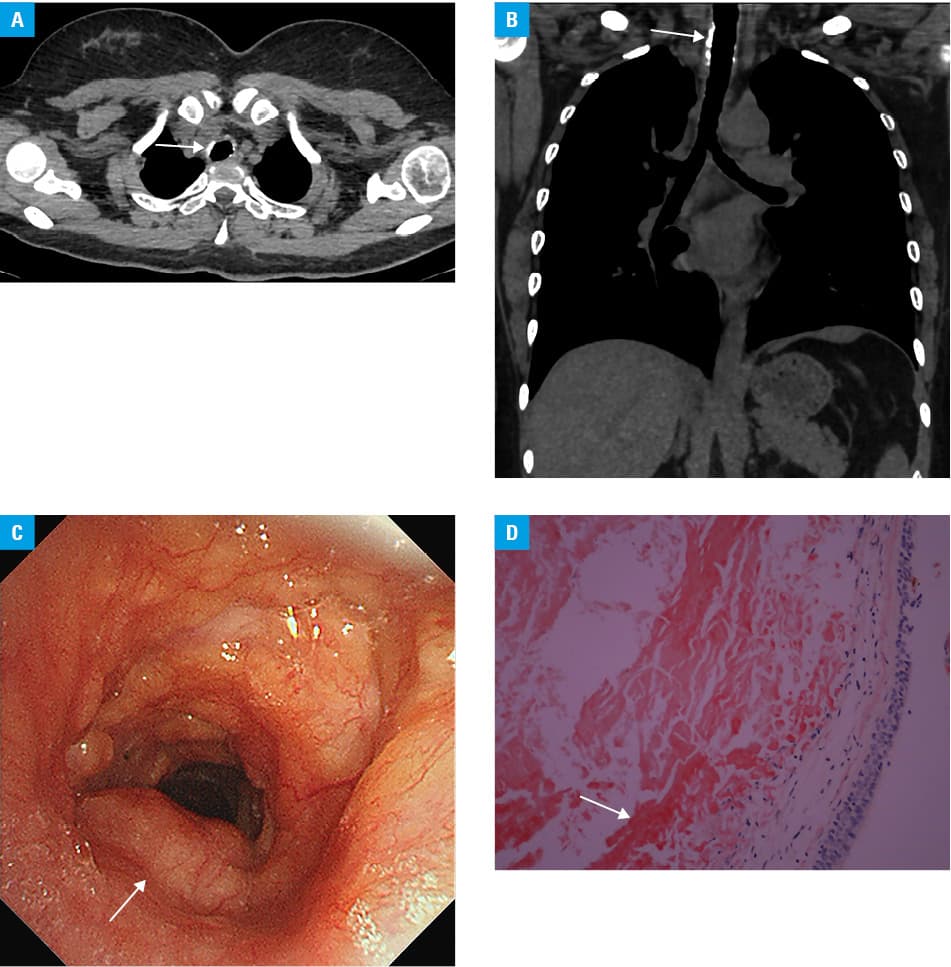
A 50‑year‑old woman presented with symptoms of progressive dyspnea for the past 2 years. Previously, she had been diagnosed with tracheal candidiasis at another hospital and had been treated with a daily dose of fluconazole for 6 months; however, the symptoms did not subside. Chest computed tomography (CT) performed at our center revealed thickening and calcification of the tracheal wall (Figure 1A and 1B). Bronchoscopy showed multiple yellowish nodular lesions on the tracheal wall, with a smooth surface and congestion (Figure 1C). Histopathological examination of a biopsy specimen demonstrated extensive subepithelial amorphous eosinophilic material, and staining with Congo red revealed characteristic amyloid deposits with an orange‑red appearance (Figure 1D). Bacterial or fungal growth was not detected in the bronchial specimen. Clinically, the patient did not exhibit any connective tissue symptoms, and the results of routine blood tests (C‑reactive protein, hemoglobin, leukocytes, creatinine, estimated glomerular filtration rate, aspartate aminotransferase, alanine aminotransferase, γ-glutamyl transferase, lactate dehydrogenase, calcium, albumin, N‑terminal pro–B‑type natriuretic peptide as well as immunoglobulins A, M, and G) were within the reference ranges. Analyses of serum and urine protein electrophoresis, cardiac magnetic resonance imaging, and abdominal ultrasound revealed no signs of systemic amyloidosis. Based on these findings, a diagnosis of primary tracheal amyloidosis was made. Most of the tracheal lesions were removed through bronchoscopy using argon and neodymium‑doped yttrium aluminum garnet lasers. The symptoms subsided within 5 days, and the patient remained in a stable condition at the 1‑year follow‑up.
Amyloidosis is characterized by the deposition and abnormal accumulation of protein in organs and tissues. It can be classified as systemic (affecting multiple organs) or localized (affecting a single organ). Most commonly, systemic amyloidosis affects the kidneys, spleen, liver, and heart.1 Typically, amyloidosis in the thoracic compartment involves the heart, but it can also affect the lung parenchyma, pleura, lymph nodes, and tracheobronchial tree.2 Primary tracheal amyloidosis is a clinically rare condition. The presence of calcifications of the tracheal wall associated with wall thickening on chest CT should suggest tracheal amyloidosis.3 Tracheobronchial tuberculosis, relapsing polychondritis, and osteochondroplastic arthritis can all be considered as differential diagnoses.2 Additional bronchoscopies and pathological examinations are recommended to confirm the diagnosis. In the tracheal tissue, the presence of yellow‑green double refraction in polarized light under a microscope or Congo red positive staining can confirm the disease.2
Tracheobronchial amyloidosis can be treated with bronchoscopic recanalization, pharmacotherapy, and external beam radiation therapy. Cryosurgery, dilatation and stenting, and laser resection are the 3 main options for bronchoscopy recanalization therapy.2 Generally, localized amyloidosis is associated with a good prognosis.
- Send T, Spiegel JL, Schade G, et al. Amyloidosis of the upper aerodigestive tract: management of a rare disease and review of the literature. Dysphagia. 2019; 34: 179‑191. | Crossref
- Sommer P, Kumar G, Lipchik RJ, et al. Tracheobronchial amyloidosis managed with multimodality therapies. Ther Adv Respir Dis. 2014; 8: 48‑52. | Crossref
- Czeyda‑Pommersheim F, Hwang M, Chen SS, et al. Amyloidosis: modern cross‑sectional imaging. Radiographics. 2015; 35: 1381‑1392. | Crossref
ARTICLE INFORMATION