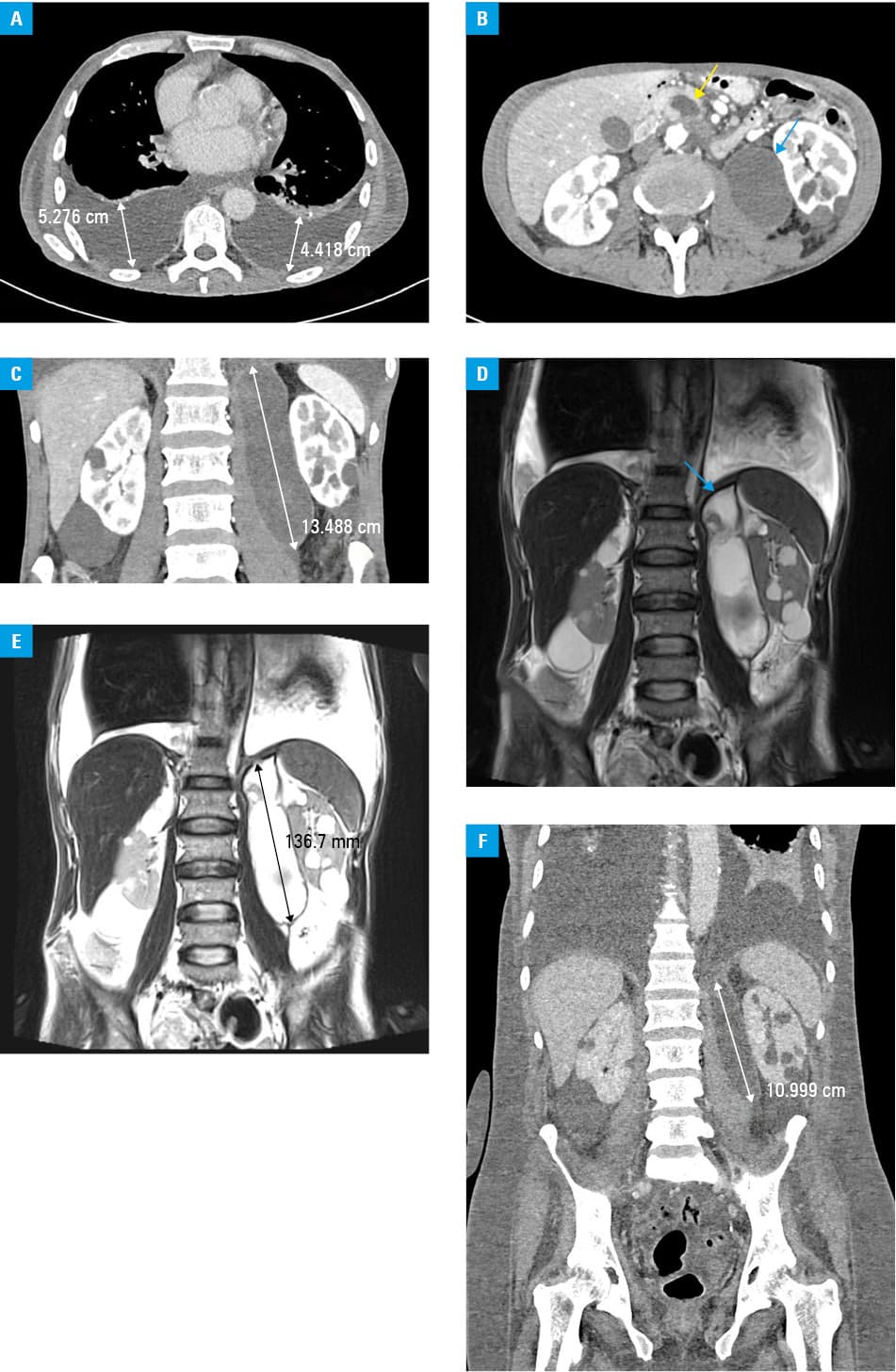
A 51‑year‑old man was admitted to the hospital with a 5‑month history of weakness, severe weight loss, minor abdominal pain, and dyspnea. He also had anorexia without nausea, vomiting, diarrhea, gastrointestinal bleeding, or fever. His medical history included hypertension, hyperlipidemia, and chronic pancreatitis. Moreover, he had a history of smoking (20 pack‑years) and excessive alcohol consumption. Physical examination revealed cachexia, shortness of breath, diminished respiratory sounds bilaterally, tachycardia, and no abdominal abnormalities. Computed tomography showed massive pleural effusion (Figure 1A), pancreaticopleural fistula (PPF) originating from the head of the pancreas, as well as multiple pancreatic pseudocysts (Figure 1B and 1C), the largest of which was situated in front of the left psoas muscle (55 mm × 38 mm × 200 mm). These findings were confirmed on magnetic resonance cholangiopancreatography (Figure 1D and 1E). There was no mass lesion or enlarged lymph nodes that would suggest pancreatic cancer. Laboratory workup revealed high activity of serum amylase (406 U/l; reference range [RR], 28–100 U/l), high concentrations of creatinine (2.24 mg/dl; RR, 0.67–1.17 mg/dl) and C‑reactive protein (90 mg/l; RR <5 mg/l), as well as a low serum calcium level (1.08 mmol/l; RR, 1.1–1.4 mmol/l). Thoracentesis was performed, which involved the removal of a large amount of dark brown, exudative, amylase- and lactate dehydrogenase (LDH)-rich fluid (amylase, 13 727 U/l; LDH, 1163 U/l; normal pleural fluid amylase activity is less than the upper limit of normal serum amylase [100 U/l] and has a ratio of pleural fluid amylase to serum amylase <1.0, normal pleural fluid LDH activity is above two‑thirds the upper limit of normal serum LDH [<250 U/l]). After the thoracentesis the patient’s clinical status improved significantly. He subsequently underwent percutaneous drainage of the largest pseudocyst without complications (Figure 1F). Due to further excessive pleural effusion, surgery was required. The patient underwent pancreatic duct anastomosis with an intestinal loop procedure (the Partington‑Rochelle procedure). On the control thoracentesis, the amylase activity decreased to 32.1 U/l. The patient was readmitted to our department 16 days after the surgical procedure with no signs of excessive fluid accumulation. He was then discharged home and remained well at the 7‑month follow‑up, with significant weight gain.
Pleural effusion can occur secondary to PPF, which is a rare complication of chronic pancreatitis. PPF is diagnosed in only 0.4% of patients with pancreatitis.1,2 Chronic pancreatitis secondary to alcohol abuse is the most common cause of PPF in adults, but it can also be associated with iatrogenic injury or trauma, among other causes.3 Clinical presentation of PPF may include pleural effusion, which causes respiratory symptoms, such as shortness of breath and cough. Physicians must be aware of the clinical features of PPF, as abdominal pain and other manifestations of pancreatitis may be minimal or absent. The Partington‑Rochelle procedure may be an appropriate therapeutic option in selected cases where clinical and / or endoscopic management is unsuccessful or unfeasible.4 Early and correct diagnosis and sufficient management can prevent long‑term morbidity and mortality.
- Sut M, Gray R, Ramachandran M, Diamond T, Pancreaticopleural fistula: a rare complication of ERCP‑induced pancreatitis. Ulster Med J. 2009; 78: 185‑186.
- Fulcher AS, Capps GW, Turner MA, Thoracopancreatic fistula: clinical and imaging findings. J Comput Assist Tomogr. 1999; 23: 181‑187. | Crossref
- Wypych K, Serafin Z, Gałązka P, Pancreaticopleural fistulas of different origin: report of two cases and a review of literature. Pol J Radiol. 2011; 76: 56‑60.
- Olakowski M, Mieczkowska‑Palacz H, Olakowska E, Lampe P. Surgical management of pancreaticopleural fistulas. Acta Chir Belg. 2009; 109: 735‑740. | Crossref
ARTICLE INFORMATION