Invasive aspergillosis mimicking cryptogenic organizing pneumonia in a patient with diffuse large B-cell lymphoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Invasive aspergillosis mimicking cryptogenic organizing pneumonia in a patient with diffuse large B-cell lymphoma
Invasive aspergillosis (IA) is an opportunistic mold infection defined as tissue invasion by the Aspergillus spp. hyphae.1 IA is increasingly recognized in immunocompromised hosts, and it leads to substantial mortality in this patient population.2 Major risk factors include treatment with intensive chemotherapy for hematologic malignancy, prolonged neutropenia, and solid organ or hematopoietic cell transplantation.1,3
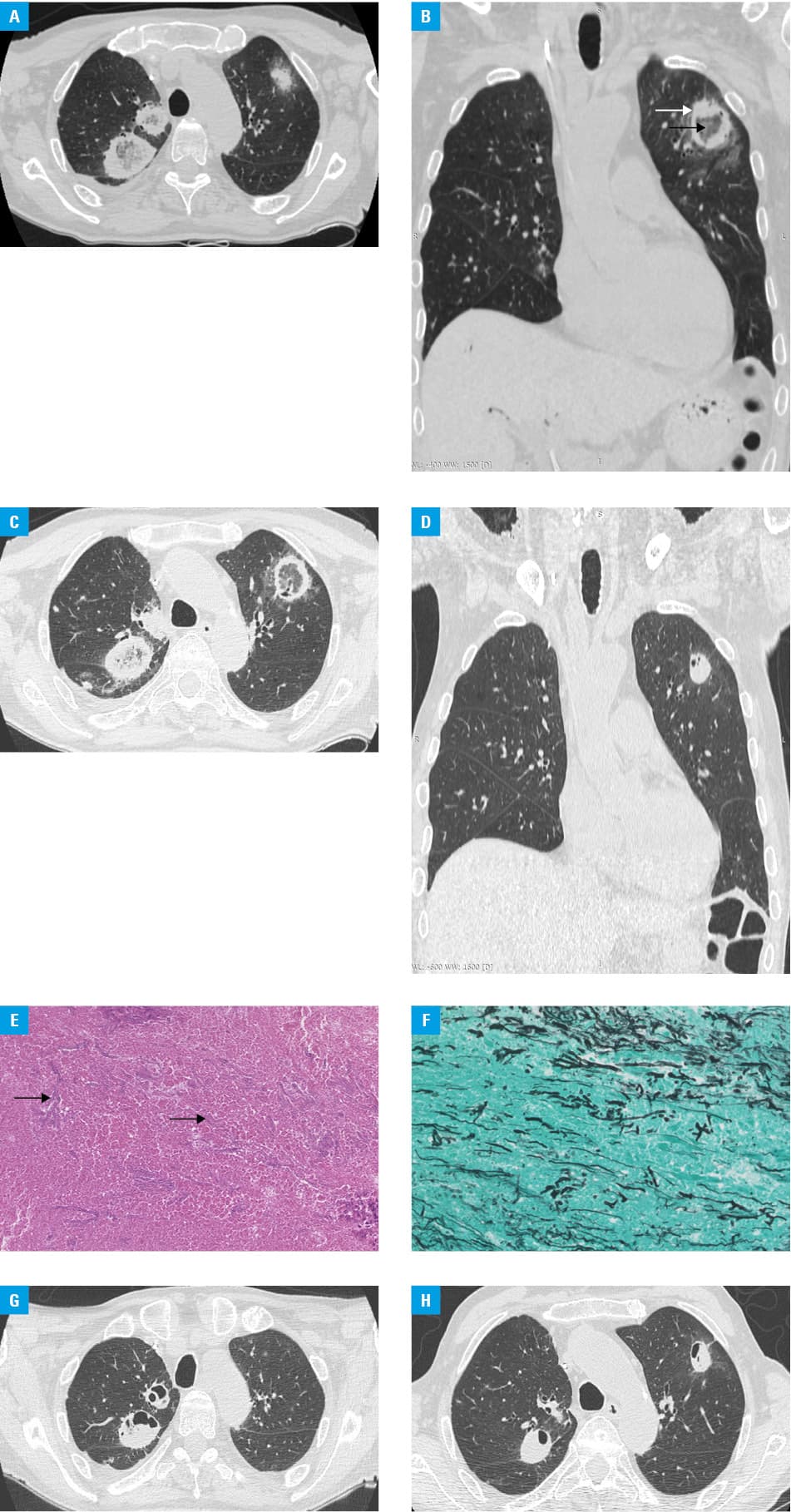
A 69‑year‑old man was referred to the department of hematology for the treatment of diffuse large B‑cell lymphoma (DLBCL). Several months before the admission, the patient had presented with severe abdominal pain, nausea, fatigue, and jaundice. Computed tomography (CT) revealed a retroperitoneal mass measuring 140 mm × 106 mm × 200 mm, with central necrosis. Histopathologic examination of the core biopsy specimen confirmed the diagnosis of DLBCL, not otherwise specified, activated B‑cell type. Positron emission tomography (PET)-CT revealed extensive lymph node involvement accompanied with bilateral ground‑glass opacities in the lungs. The patient underwent bronchoscopy with bronchoalveolar lavage, which yielded positive culture for ESBL‑producing Klebsiella pneumoniae and herpes simplex virus type 1. Despite the absence of clinical signs of infection, systemic therapy was postponed and anti‑infective treatment with meropenem and acyclovir was administered, resulting in the resolution of the sings of pneumonia on imaging studies. Standard systemic chemoimmunotherapy with the R‑CHOP regimen (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) was administered concurrently with intrathecal methotrexate. Following the second cycle of R‑CHOP, the PET‑CT scan showed progressive disease. Second‑line salvage treatment with alternating R‑IVAC (rituximab, ifosfamide, cytarabine, and etoposide) and R‑CODOX‑M (rituximab, cyclophosphamide, vincristine, doxorubicin, and methotrexate) regimens was initiated. The patient received a total of 2 cycles of R‑IVAC and 1 cycle of R‑CODOX‑M, which were complicated by severe pancytopenia with prolonged agranulocytosis. Over the next weeks, he presented with several episodes of fever with chills, while laboratory tests showed a marked elevation of the inflammatory parameters. Despite the broad‑spectrum antibiotic therapy, his general condition deteriorated. C‑reactive protein values were persistently elevated (up to 237 mg/l; reference range <10 mg/l); however, cultures and fungal antigen assays remained negative. A high‑resolution CT (HRCT) scan showed features suggestive of cryptogenic organizing pneumonia (COP): bilateral consolidations with a central ground‑glass density (Figure 1A–1D). However, based on a positive result of the serum galactomannan antigen test, the diagnosis of probable IA was established, prompting the treatment with voriconazole. Microscopic examination of the specimens obtained during bronchoscopy demonstrated Aspergillus spp. hyphae, thus confirming the IA diagnosis (Figure 1E and 1F). Despite intensive antifungal treatment with amphotericin B lipid complex, the evolution was marked by the appearance of pulmonary cavities and nodules on HRCT (Figure 1G and 1H). The patient’s clinical condition further deteriorated and 7 months after his initial presentation, he died of the primary refractory DLBCL and COVID‑19.
The high burden of infectious complications in immunocompromised patients makes the differential diagnosis of pulmonary infiltrates challenging. Clinical and radiological manifestations of IA are nonspecific and may be indistinguishable from other pulmonary conditions.1,3 In the described case, IA shared common radiological features with COP, underscoring the need to perform an accurate diagnostic evaluation. Given its potential for rapid dissemination and high death rate, early treatment may be lifesaving. Thus, all high‑risk patients presenting with persistent signs of infection should be screened for fungal infections.
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015; 70: 270‑277. | Crossref
- Lamberink H, Wagemakers A, Sigaloff KCE, et al. The impact of the updated EORTC/MSG criteria on the classification of hematological patients with suspected invasive pulmonary aspergillosis. Clin Microbiol Infect. 2022; 28: 1120‑1125. | Crossref
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020; 71: 1367‑1376.
ARTICLE INFORMATION