Applicability of shear wave elastography for lacrimal gland evaluation in primary Sjögren syndrome
Key words: diagnostic imaging, eye dryness, lacrimal glands, primary Sjögren syndrome, shear wave elastography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Applicability of shear wave elastography for lacrimal gland evaluation in primary Sjögren syndrome
Introduction: Primary Sjögren syndrome (pSS) is a systemic autoimmune disease that mainly affects the salivary and lacrimal glands, leading to their progressive destruction.
Objectives: The primary aim of this study was to verify whether shear wave elastography (SWE) of the lacrimal glands can be used to differentiate patients with pSS from healthy controls. The secondary aim was to assess whether there are any associations between SWE values, results of other ocular tests included in pSS diagnosis (the Schirmer test, ocular staining score [OSS]), and subjective symptoms of eye dryness.
Patients and methods: The study included 45 patients with pSS (41 women, 4 men) and 108 healthy controls (104 women, 4 men). All pSS patients met the 2016 American College of Rheumatology / European League Against Rheumatism pSS classification criteria. The participants underwent bilateral SWE of the lacrimal glands with the results expressed in kilopascals (kPa). The Schirmer test was performed in all patients, and OSS was calculated only in the pSS group.
Results: The patients with pSS had significantly higher SWE values for the lacrimal glands than the controls. No significant differences in SWE results were observed between the groups of pSS patients with or without eye dryness confirmed by the Schirmer test and OSS, or the pSS patients with or without subjective symptoms of eye dryness. The optimal cutoff point for the diagnosis of pSS for the mean result of left and right lacrimal gland elastography was 7.2 kPa (sensitivity, 88.9%; specificity, 88%). Lacrimal gland SWE values may be a good classifier for the diagnosis of pSS, with an area under the receiver operating characteristic curve of 89.8 (95% CI, 81.5–98.1).
Conclusions: SWE of the lacrimal glands is a noninvasive, quantitative method that seems to be a reliable additional examination tool to support the diagnosis of pSS. Its role among the functional tests has not yet been well defined. To confirm the usefulness of SWE for pSS diagnosis, a standardized and widely accepted study protocol should be defined first.
What's new?
The present study is the first to assess whether shear wave elastography (SWE) of the lacrimal glands can be used to support the diagnosis of primary Sjögren syndrome (pSS). The disease not only manifests as “sicca syndrome,” characterized by ocular and oral dryness, but also includes a variety of extraglandular manifestations. As a result, appropriate diagnosis of pSS still poses a challenge. The current classification criteria for pSS include only functional tests (the Schirmer test and the ocular staining score or the van Bijsterfeld score) for eye assessment. Among the imaging modalities there is still no simple, noninvasive, and quantitative method that would support the diagnosis of pSS. Based on the results of our study, SWE of the lacrimal glands is a reliable additional examination tool that can contribute to the diagnosis of pSS.
Introduction
Primary Sjögren syndrome (pSS) is a systemic, autoimmune connective tissue disease characterized by lymphocytic infiltration of the salivary and lacrimal glands, as well as other types of exocrine gland involvement. The disease manifests as sicca syndrome or sicca complex, with oral and ocular dryness as the principal symptoms; however, there is also a variety of extraglandular manifestations that can potentially affect numerous organs, such as the lungs, kidneys, and the nervous system.1
The disease mainly affects women, with the average female‑to‑male ratio of 9:1, and it is one of the most common rheumatic disorders.2 The incidence and prevalence of pSS vary widely around the world. The highest incidence was reported in studies from Europe and Asia. The prevalence is estimated at 43 per 100 000 people.2 Although the pSS phenotype may vary as a function of geolocation and ethnicity, objective findings of salivary and / or lacrimal gland destruction were observed in most patients.
Until recently, a wide variety of imaging methods have been used to assess the salivary glands in pSS, including ultrasonography, sialography, magnetic resonance (MR) sialography, scintigraphy, magnetic resonance imaging (MRI), and elastography.3 On the other hand, in the case of the lacrimal glands, the assessment is performed mainly by means of functional tests rather than imaging methods. The current classification criteria for pSS published in 2016 by the American College of Rheumatology and European League Against Rheumatism (ACR/EULAR)4 include the Schirmer test and the ocular staining score (OSS) or the van Bijsterveld score. The Schirmer test is primarily used to diagnose dry eye syndrome, and it determines whether the eye produces enough tears.5 The OSS uses lissamine green dye to assess the conjunctiva and fluorescein to assess the cornea. It is easily applied in clinical practice and gives equal numerical weight to corneal and conjunctival changes.6 Both of these tests are routinely used to evaluate the lacrimal glands in pSS, in contrast to imaging techniques.
Choosing an appropriate imaging method for the diagnosis poses a challenge not only in pSS, but also in other rheumatic diseases. Large vessel vasculitis7,8 and gout9 are examples of conditions for which new imaging modalities are being developed to facilitate early diagnosis and follow‑up of the disease activity.
Appropriate assessment of eye involvement in pSS is important not only due to classification criteria but also because of the fact that dry eye disease affects most patients with pSS and there is a weak correlation between its symptoms and signs. Xerophthalmia significantly impairs the quality of life of pSS patients and its management is often difficult and unsatisfactory.10
Assessment of structural changes in the lacrimal glands in the course of the disease can pose a great challenge, potentially due to their small size and anatomy. Situated in the lacrimal fossa in the upper lateral region of each orbit, the lacrimal glands are structures composed of small lobules intermixed with connective tissue septations and lacking a capsule.11 They normally measure approximately 20 mm × 12 mm × 5 mm and are not often subjected to imaging examinations.
Shear wave elastography (SWE) is a rapidly evolving imaging technique that enables quantification of mechanical and elastic tissue properties.12 It provides additional information related to tissue characteristics by evaluating tissue elasticity, which may contribute to the diagnosis of many disorders, including rheumatic diseases. In the field of rheumatology, this technique has been used for example to assess muscles in idiopathic inflammatory myopathies,13 to evaluate the liver, pancreas, spleen, and kidneys in patients with familial Mediterranean fever,14 to measure skin strain in systemic sclerosis,15 or to assess the salivary glands in the course of pSS,16 as well as to identify parotid lymphoma in patients with pSS.17
This study aimed to verify whether SWE of the lacrimal glands can be used to differentiate pSS patients from healthy controls. Moreover, we checked if there are any associations between the SWE values, the results of the Schirmer test and OSS, and subjective eye dryness in the patients with pSS.
Patients and methods
Participants
The study was conducted between October 2018 and November 2019. The participants were divided into 2 groups: the pSS group (n = 45) and the control group (n = 108). The pSS group included patients with a diagnosis of pSS who met the 2016 ACR/EULAR pSS classification criteria, diagnosed at the Early Arthritis Clinic in Warsaw, Poland. All pSS patients treated at the Clinic were considered for participation in the study and those meeting the pSS criteria were chosen based on their medical history. The control group comprised 108 healthy volunteers free of clinical features of pSS, with no sicca symptoms and negative Schirmer test results (>10 mm of moisture on the filter paper in 5 minutes). Additionally, the control group did not use artificial tears for the duration of the study.
The exclusion criteria encompassed past head radiotherapy, surgeries affecting the lacrimal glands, orbital pseudotumor, sarcoidosis, hepatitis C, HIV infection, lymphoma of the lacrimal glands or other proliferation processes within them, use of cholinolytics, antidepressants, or other drugs potentially affecting the eye test results, and presence of any other pathology within the lacrimal glands.
Study protocol
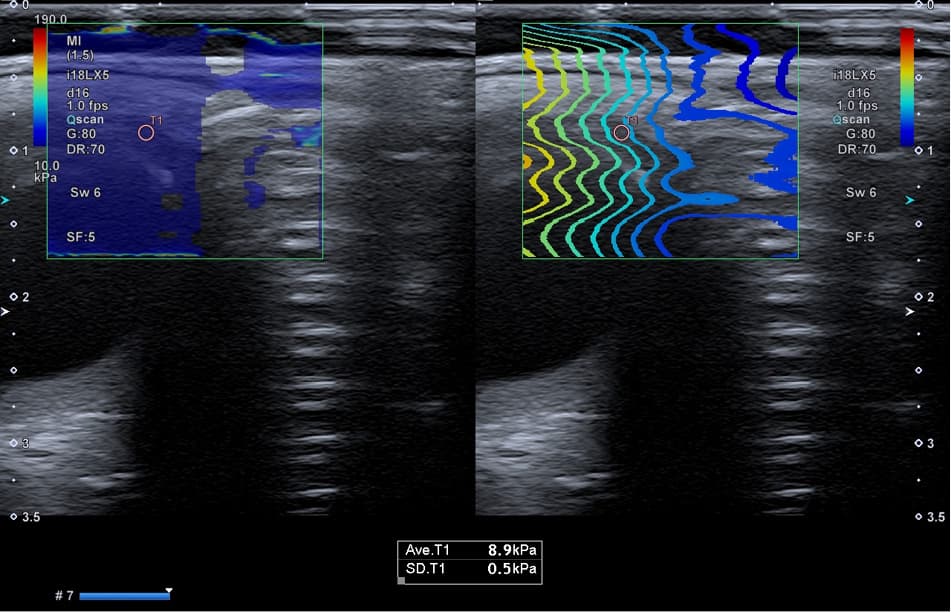
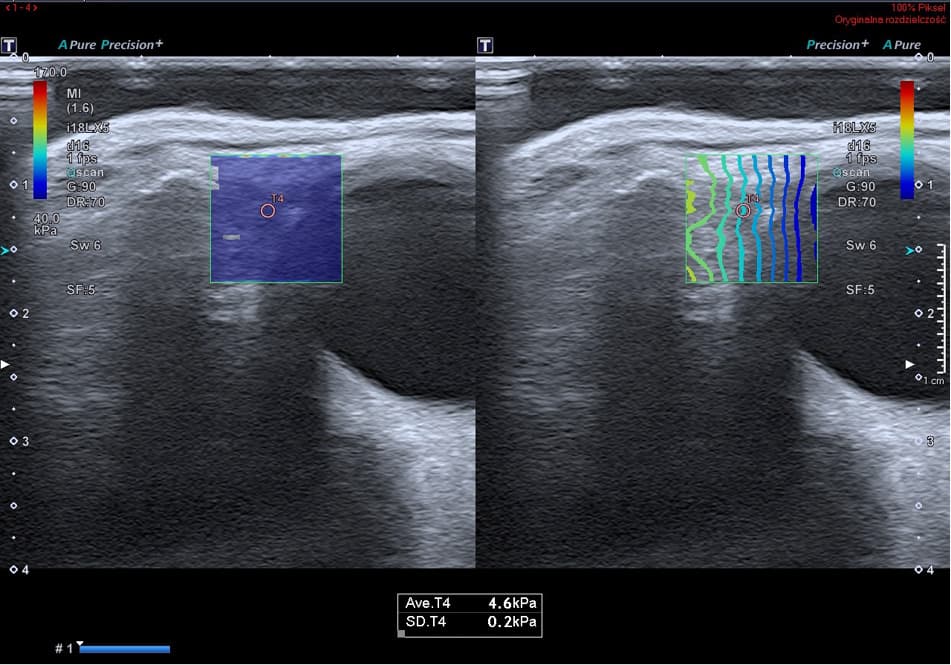
All patients included in the study underwent bilateral SWE assessment of the lacrimal glands. All SWE measurements were performed in the morning. None of the patients used any topical agents before the examination. Each region was examined separately, with the patient placed in a supine position. Sonographic scans were carried out with a Toshiba iAplio 900 ultrasonograph (Canon Medical Systems, Nasushiobara, Japan) using a 5–18 MHz transducer. During the examination, the face of the patient was covered with a hydrogel pad and a thick layer of gel. The transducer was placed perpendicularly to the skin and no pressure was applied on the examined tissues. The measurements were performed within a region of interest (ROI) 0.1 × 0.1 cm in size, located in the middle of the lacrimal gland. All SWE measurements were performed by 2 radiologists with 5 years of experience in SWE imaging. At least 5 single measurements were taken for each gland, and the average Young modulus was calculated. The SWE values within the ROI were measured in kilopascals (kPa). An example of a typical SWE scan of the lacrimal glands in the pSS group is presented in Figure 1, and an SWE scan of a healthy participant is shown in Figure 2.
Clinical data of the pSS patients were collected from the Early Arthritis Clinic database.
Statistical analysis
Statistical analysis of the data was performed using the R statistical software, version 3.6.3 (R Core Team, 2017, Vienna, Austria). A P value below 0.05 was considered significant in all analyses. All the performed tests were 2‑sided. The studied groups were characterized in terms of anthropometric and demographic parameters using descriptive statistics. The Shapiro–Wilk test was used to assess the normality of distribution of continuous variables. Mean with SD was reported for the normally distributed continuous data, and median with interquartile range was reported for the nonnormally distributed variables. Categorical variables were presented as the number and percentage of occurrences. Differences between the 2 groups were evaluated using a 2‑sided independent‑samples t test for the normally distributed continuous variables or the Mann–Whitney test otherwise, whereas the χ2 test was used for the categorical variables. Receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive capabilities of lacrimal gland elastography results as a marker of pSS. Cutoff points were calculated with the closest‑to‑the‑corner method (ie, the point closest to the 100% sensitivity and 100% specificity was chosen). Characteristics of selected predictors were presented as the area under the ROC curve (AUC) with 95% CI, and the cutoff value with sensitivity and specificity. To assess the relationship between selected predictive factors and odds for the diagnosis of pSS, univariable logistic regression models were built. Odds ratios (OR) with corresponding 95% CIs and P values derived from the Wald test were reported. To assess the effect of selected parameters on elastography results, univariable linear models were applied; linear relationship coefficients with 95% CIs and the Wald test P values were presented.
Bioethical standards
This was a prospective study whose protocol was approved by the Bioethics Committee of the National Geriatrics, Rheumatology and Rehabilitation Institute (KBT‑7/3/2018). Written informed consent was sought from all pSS patients and healthy controls. All the procedures were conducted in accordance with the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, October 2013).
Results
Baseline characteristics of the study population are presented in Table 1. The patients with pSS and the controls did not differ in terms of demographic data.
Variable | pSS group (n = 45) | Control group (n = 108) | P value | |||
Data are shown as number (percentage) of patients unless indicated otherwise.
a Assessed in 26 patients
b Assessed in 44 patients
c Assessed in 41 patients
Abbreviations: anti‑SSA, anti–Sjögren syndrome–related antigen A, IQR, interquartile range; pSS, primary Sjögren syndrome | ||||||
Age, y, median (IQR; range) | 50 (39–62; 25–80) | 51 (45.8–56.2; 40–67) | 0.65 | |||
Sex | Women | 41 (91.1) | 104 (96.3) | 0.24 | ||
Men | 4 (8.9) | 4 (3.7) | ||||
Eye dryness | Yes | 26 (59.1) | 0 | – | ||
No | 18 (40.9) | 108 (100) | ||||
No data | 1 | 0 | ||||
Duration of xerophthalmiaa, y, median (IQR) | 4.50 (3.00–6.75) | – | – | |||
Schirmer test result ≤5 mm/5 minb | Left eye | 13 (29.5) | – | – | ||
Right eye | 13 (29.5) | |||||
At least in 1 eye | 15 (34.1) | |||||
Sicca score ≥5 pointsc | Left eye | 15 (36) | – | – | ||
Right eye | 15 (36.6) | |||||
At least in 1 eye | 16 (39) | |||||
Antinuclear antibodies presence | Yes | 45 (100) | – | – | ||
No | 0 | |||||
Anti‑SSA/Ro positivity | Yes | 43 (95.5) | – | – | ||
No | 2 (4.4) | |||||
Diabetes mellitus | Yes | 2 (4.4) | – | – | ||
No | 43 (4.4) | |||||
Smoking | Yes | 6 (14) | – | – | ||
No | 37 (86) | |||||
No data | 2 | |||||
Atopy | Yes | 0 | – | – | ||
No | 45 (100) | |||||
Thyroid disease | Yes | 12 (26.7) | – | – | ||
No | 33 (73.3) | |||||
pSS treatment | Hydroxychloroquine | 39 (86.7) | – | – | ||
Glucocorticosteroids | 26 (57.8) | |||||
Azathioprine | 7 (15.6) | |||||
Methotrexate | 6 (13.3) | |||||
No treatment | 0 | |||||
The pSS group included 45 patients, 41 women and 4 men, with a median age of 50 years (range, 25–80 years). The control group included 108 participants, 104 women and 4 men, with a median age of 51 (range, 40–67 years).
All pSS patients were treated with disease‑modifying antirheumatic drugs and / or glucocorticosteroids (GCs). No biological therapies were used. None of the patients used saliva substitutes, topical nonsteroidal anti‑inflammatory drugs, topical GCs, topical cyclosporine A, serum tear drops, or oral muscarinic agonists (pilocarpine or cevimeline).
The results of the lacrimal gland SWE measured in kPa were significantly different in the pSS group than in the control group (Table 2). Higher elastography results were associated with an increased probability of a pSS diagnosis, with an OR of 1.95 (95% CI, 1.493–3.001) per a 1‑unit increase in the mean SWE result for both lacrimal glands.
Location | SWE values, kPa | P value | |
pSS group (n = 45) | Control group (n = 108) | ||
Data are shown as median (interquartile range).
Abbreviations: kPa, kilopascals; SWE, shear wave elastography; others, see Table 1 | |||
Right lacrimal gland | 15.6 (7.7–21.0) | 6.45 (6.10–6.90) | <0.001 |
Left lacrimal gland | 16.0 (7.7–23.0) | 6.45 (5.90–7.00) | <0.001 |
Mean SWE values for left and right lacrimal glands | 16.30 (7.65–22.00) | 6.40 (6.00–6.86) | <0.001 |
There were no differences in elastography results related to age. In the linear regression model estimating the sex‑specific effects in the studied groups, the effect of sex (male vs female) was –1.806 (95% CI, –4.732 to 1.121; P = 0.23).
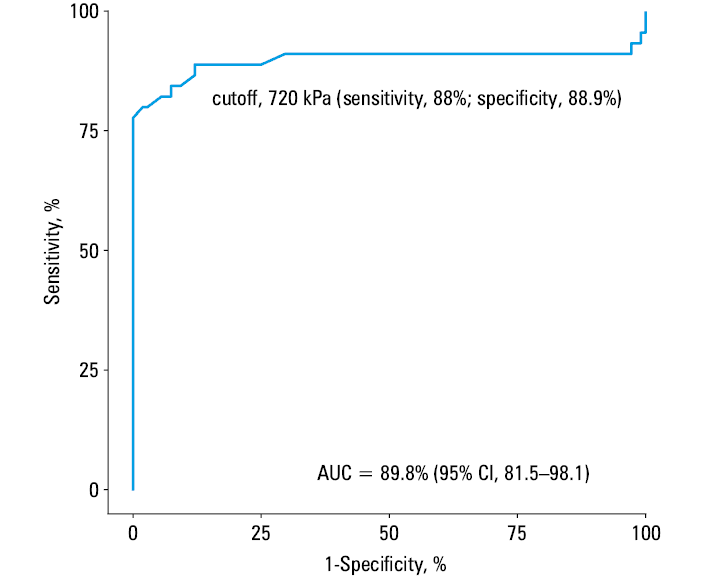
The results of lacrimal gland SWE seem to be a good classifier for the diagnosis of pSS, with an AUC of 89.8 (95% CI, 81.5–98.1) for the mean result of left and right lacrimal gland elastography. Based on the results of the ROC analysis, the optimal cutoff point for the diagnosis of pSS for the average result of lacrimal gland elastography was 7.2 kPa (sensitivity, 88.9%; specificity, 88%). A ROC curve for SWE measurements of the lacrimal glands as a predictor of a pSS diagnosis is shown in Figure 3.
No significant differences in the elastography values were observed between the subgroups of pSS patients with or without eye dryness confirmed by the Schirmer test and OSS result. Additionally, there were no significant differences in SWE values between the pSS patients with or without subjective eye dryness. However, the size of the subgroups in the abovementioned comparisons was small, hence the power of the tests was low. Table 3 presents the results of lacrimal gland SWE in the pSS patients divided according to the Schirmer test and OSS results, and the presence of subjective eye dryness.
Variable, kPa | Schirmer test <5 mm/5 min in at least 1 eye (n = 15) | Normal Schirmer test result (n = 29) | P value |
SWE of the right lacrimal gland | 12 (7.5–18.5) | 16 (7.8–22) | 0.28 |
SWE of the left lacrimal gland | 16 (7.75–19.5) | 17 (7.7–25) | 0.29 |
Mean SWE values for left and right lacrimal glands | 14 (7.65–18.75) | 16.3 (7.65–23.50) | 0.36 |
OSS ≥5 in at least one eye (n = 16) | Normal OSS (n = 25) | P value | |
SWE of the right lacrimal gland | 9.9 (7.5–18) | 16 (11–22) | 0.08 |
SWE of the left lacrimal gland | 12 (7.45–17.5) | 18 (11–24) | 0.07 |
Mean SWE values for left and right lacrimal glands | 10.78 (7.51–17.46) | 18.5 (11.5–22.5) | 0.07 |
OSS ≥5 in at least one eye OR Schirmer test <5 mm/5 min in at least 1 eye (n = 18) | Normal OSS AND normal Schirmer test result (n = 22) | P value | |
Mean SWE values for left and right lacrimal glands | 10.78 (7.34–17.49) | 17.25 (11.5–24) | 0.09 |
Subjective eye dryness (n = 26) | No subjective eye dryness (n = 18) | P value | |
SWE of the right lacrimal gland | 14.5 (7.7–20.75) | 17 (8.45–22) | 0.29 |
SWE of the left lacrimal gland | 14 (7.73–20.5) | 20.5 (8.78–24.25) | 0.19 |
Mean SWE values for left and right lacrimal glands | 13.75 (7.65–21.38) | 19.25 (8.61–23.12) | 0.22 |
Discussion
SWE of the lacrimal glands is a novel and still unexplored diagnostic tool. Until now, there have been only 2 studies focusing on SWE of the lacrimal glands, conducted by Bădărînză et al18 and Cerit et al.19 The former one18 was designed to evaluate the lacrimal glands in healthy individuals and in patients with diabetes mellitus and / or obesity, with or without sialosis. The main finding of the study was the lack of differences in the elastic modulus between the groups. However, the groups analyzed by Bădărînză et al18 were more heterogeneous than the population of our study.
The main purpose of the study by Cerit et al19 was to determine a reference data set for stiffness value of a normal lacrimal gland using SWE. Mean normal SWE value for the lacrimal gland in the healthy population included in this study was estimated to be 6.17 (2.94) kPa. There were no significant differences related to sex (P >0.05), whereas age exhibited a weak correlation with the stiffness value.
Although the abovementioned studies included different groups of patients, it is worth comparing them with our report in terms of the equipment used, study protocol, and SWE results in healthy controls. The main difference is that the SWE values in the control group in our study (6.4 kPa) and in the analysis by Cerit et al19 (6.17 kPa) were lower than those reported by Bădărînză et al18 (9.47 kPa). It may be related to the fact that different ultrasonography devices were used in each study (Toshiba iAplio 900 vs LOGIQ S819 [GE Healthcare Systems, Waukesha, Wisconsin, United States] vs Supersonic Imagine AixplorerUltimate18 [Aix‑en‑Provence, France]). There was also a difference in ROI (our study, 1‑mm ROI; Cerit et al,192‑mm ROI; Bădărînză et al,18 2‑mm diameter Q‑box). Therefore, a standardized test protocol for SWE of the lacrimal glands should be developed to enable larger‑scale studies regardless of the type of the study group.
The lacrimal glands are very rarely examined using other imaging tools, and no widely used objective method of their assessment has been established. Therefore, there is a need to develop or identify an acceptable imaging technique for clinical and research purposes.
Attempts to use ultrasonography to evaluate the lacrimal glands in the course of Sjögren syndrome have been scarce, encompassing 4 studies published so far: 2 prospective studies20,21 and 2 case reports.22,23 Giovagnorio et al20 were the first to perform lacrimal gland ultrasonography in 15 patients with pSS and 15 healthy controls. They based their approach on the observation that superficial location of the lacrimal glands facilitates their evaluation with high‑resolution sonography. In this study, atrophic and normal‑size glands in the pSS patients were difficult or impossible to detect, while detectable glands correlated with lacrimal impairment. Meanwhile, in a study by De Lucia et al,21 glandular parenchyma inhomogeneity and fibrous gland appearance were the features that differentiated pSS patients from healthy controls. The authors evaluated 57 healthy individuals and 17 pSS patients with a good‑to‑excellent intra- and inter‑rater reliability.
Several attempts were also made to define MR features of the lacrimal glands in patients with pSS.24,25 The results of the first MR study in patients with Sjögren syndrome were published in 1998. Izumi et al24 showed that a change in the size associated with accelerated fat deposition may be the characteristic MR feature of the lacrimal glands affected by Sjögren syndrome. Although the results were encouraging, there were not many subsequent attempts to confirm them. Likewise, there have not been many studies using computed tomography (CT), 68Ga‑PSMA‑11 positron emission tomography / CT,26,27 or confocal microscopy examination of the lacrimal glands in patients with pSS.28,29 This raises the question of why imaging methods, which are more and more common in modern medicine, are not used for lacrimal gland assessment in pSS.
The need for facilitating the pSS diagnosis and ruling out differential diagnoses has increased in the last years, as ocular dryness may be related to a variety of conditions that may require very different diagnostics, treatments, and follow‑up modalities.30 Although the standardized functional tests for eye assessment have many advantages, they also have certain limitations. The Schirmer test has good specificity for pSS (71%–73%), although its sensitivity is only 49% to 54%.31 It is, however, simple to perform at many health care facilities, not only in centers specialized in ophthalmology. In contrast, OSS is used mainly by ophthalmologists. This fact may be perceived as an advantage, as all patients with suspected pSS should be assessed for differential diagnoses and complications by an ophthalmologist. However, access to a professional ophthalmologist with experience in pSS treatment may be limited, especially in smaller medical centers. Moreover, the concordance with salivary gland biopsy results is higher for the Schirmer test than for OSS.32
One of the most intriguing aspects of dry eye is poor correlation between its symptoms and signs,33 which we also found in a large clinical cohort of SS patients.34 The diagnostic process is even more complicated, as the correlation between dry eye symptoms and the Schirmer test results is weak, and there is some controversy on its reproducibility, especially for the higher scores.35 However, as better markers of pSS have not been identified so far, it is necessary to rely on the current classification criteria.
It is likely that functional tests are used more often to assess the eye also because they are more accessible, standardized, and usually cheaper than the imaging tests. MRI and CT are the techniques most frequently used to differentiate between benign and malignant lesions, often when the lacrimal glands present with unilateral swelling. As there is an increased incidence of B‑cell lymphomas in pSS36 that may also occur in the lacrimal gland,37 MRI may prove superior to CT5 for examining such cases.
With regard to SWE, its application in pSS is difficult to assess so far. Our study showed that it is a noninvasive, simple, and cost‑effective quantitative modality with good sensitivity and specificity.
The last purpose of our research was to determine whether there are any relations between the SWE values and the results of the Schirmer test, OSS, and subjective eye dryness in pSS patients. We showed that in the patients with normal Schirmer test results, normal OSS, and no symptoms of eye dryness, the SWE values were higher than in the patients with the Schirmer test positive for pSS, pathologic ocular staining, and eye dryness; however, no significant associations were found. The lack of correlation may be due to the very small size of the groups (there were only 15 patients with a positive Schirmer test result and 16 patients with OSS ≥5). It is important to conduct studies involving more participants because we would rather expect higher SWE values in the patients with pathological results of functional eye tests, as in the case of salivary glands in pSS. In a study by Satış et al,38 labial biopsy was replaced with the parotid strain ratio measured during SWE, which indicated that the SWE result corresponds with salivary gland inflammation in the course of pSS. As mentioned above, a discrepancy between the symptoms and objective measures is characteristic of pSS in general.39 In pSS, subjective dryness poorly correlates with the amount of glandular secretion, which may explain the lack of association between xerophthalmia and the values of lacrimal gland SWE.
Limitations of the study
We are well aware of the potential limitations of this analysis. Firstly, the study group was relatively small; however, taking into account the novelty of the study, the group seems large enough to allow for initial conclusions. However, future studies should be performed in larger cohorts of patients. Secondly, our results cannot be compared with any published evidence because, to the best of our knowledge, none of the previous studies examined SWE of the lacrimal glands in pSS patients. That is why no standardized study protocol has been established so far. Thirdly, our control group consisted only of healthy individuals. It would also be beneficial to examine sicca syndrome patients without pSS and to compare them with pSS individuals. Additionally, the grey scale / Doppler ultrasonography of the lacrimal glands should be conducted in all participants to broaden the research spectrum. Finally, we only performed the Schirmer test in the controls, and it would be advantageous to extend the diagnostic procedures in the control group.
Regarding our final results, SWE of the lacrimal glands is a promising imaging method that could be used to evaluate patients with pSS.
Conclusions
SWE of the lacrimal glands is a noninvasive quantitative method that seems to be a reliable additional examination tool to support the diagnosis of pSS. It is a novel, simple, and cost‑effective modality for assessing the lacrimal glands. However, its role among the functional tests of the lacrimal glands has not yet been well defined. In the present study, this method was characterized with good sensitivity (88.9%) and specificity (88%). These results warrant future research, preferably also addressing the limitations of this study. As the potential of this method has been demonstrated, more extensive future studies on a larger number of patients are needed to establish reference SWE values for the lacrimal glands.
- Negrini S, Emmi G, Greco M, et al. Sjögren’s syndrome: a systemic autoimmune disease. Clin Exp Med. 2022; 22: 9‑25. | Crossref
- Qin B, Wang J, Yang Z, et al. Epidemiology of primary Sjögren’s syndrome: a systematic review and meta‑analysis. Ann Rheum Dis. 2015; 74: 1983‑1989. | Crossref
- Świecka M, Maślińska M, Paluch Ł, et. al. Imaging methods in primary Sjögren’s syndrome as potential tools of disease diagnostics and monitoring. Reumatologia. 2019; 57: 336‑342. | Crossref
- Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology / European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: a consensus and data‑driven methodology involving three international patient cohorts. Arthritis Rheumatol. 2017; 69: 35‑45.
- Bjordal O, Norheim KB, Rødahl E, et al. Primary Sjögren’s syndrome and the eye. Surv Ophthalmol. 2020; 65: 119‑132. | Crossref
ARTICLE INFORMATION