Potential benefits of one-time gastroscopy in search for precancerous conditions
Key words: esophageal cancer, gastric cancer, gastroscopy, precancerous conditions, screening



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Potential benefits of one-time gastroscopy in search for precancerous conditions
Introduction: Precancerous conditions for esophageal (EA) and gastric adenocarcinoma (GA) are Barrett’s esophagus (BE) and atrophic gastritis (AG), respectively. Their surveillance is crucial for the detection of early lesions.
Objectives: The study aimed to assess whether one‑time esophagogastroduodenoscopy (EGD) in search for precancerous conditions would be effective in the population with low‑to‑moderate esophageal and gastric cancer risk.
Patients and methods: A total of 5984 individuals who underwent diagnostic EGD in 3 endoscopic centers, from March 2018 to October 2019, were analyzed to assess the age of occurrence of precancerous conditions and cancers. Age distribution of the patients with malignant gastric and esophageal tumors registered in the national cancer registry from 2014 to 2017 was analyzed.
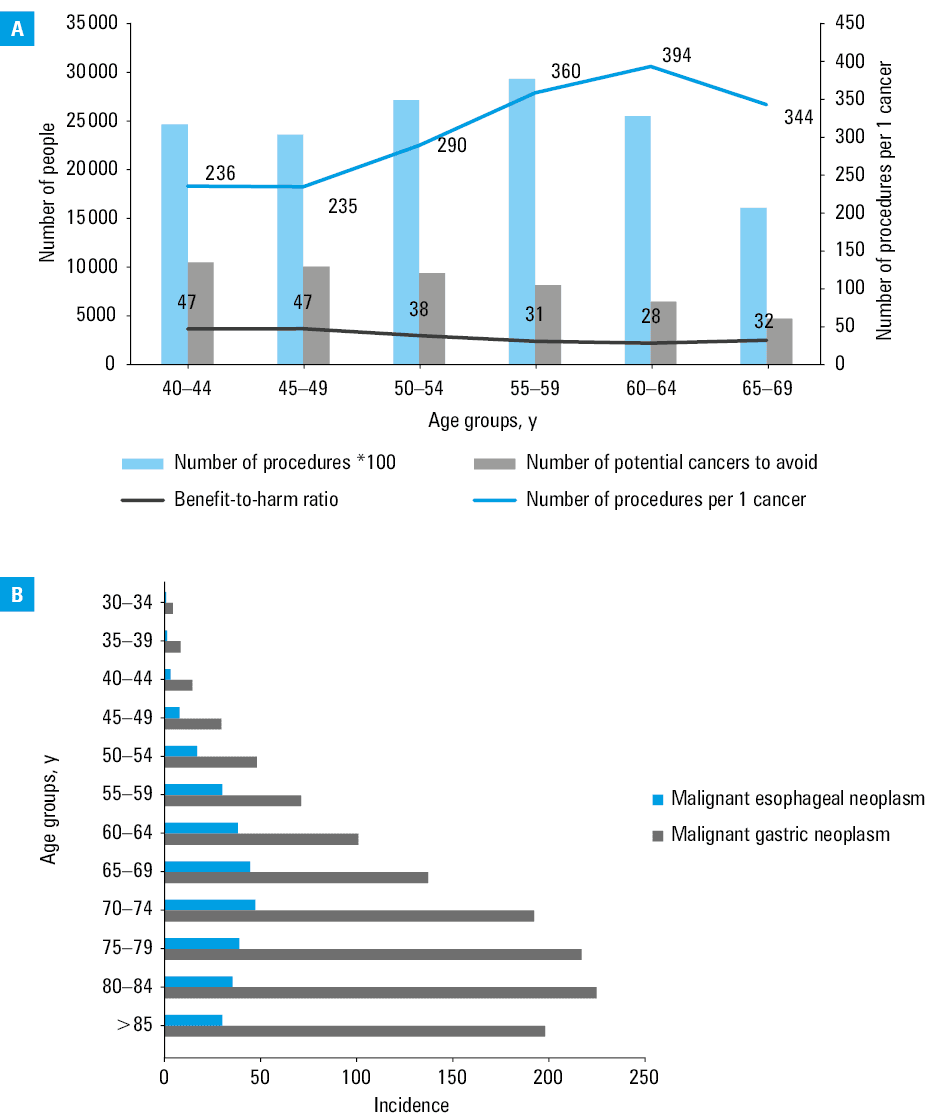
Results: In comparison with individuals below 40 years old, the risk of EA and GA diagnosis increased at the age of 60 to 64 years (odds ratio [OR], 12.1; 95% CI, 1.5–98.6), gastric and esophageal dysplasia at the age of 55 to 59 years (OR, 3.6; 95% CI, 1.3–9.7), and BE and AG at the age of 40 to 44 years (OR, 1.6; 95% CI, 1.04–2.4). The number of procedures per 1 cancer that could be potentially avoided was 236, 235, 290, 360, 394, and 344 for the age groups of 40–44 years, 45–49 years, 50–54 years, 55–59 years, 60–64 years, and 65–69 years, respectively. The assessed potential benefit‑to‑harm ratio was 47, 38, 31, 28, and 32 for the age groups of 40–49 years, 50–54 years, 55–59 years, 60–64 years, and 65–69 years, respectively.
Conclusions: One‑time EGD in search for precancerous conditions could be potentially applicable in individuals between 40 and 69 years of age.
What's new?
Screening gastroscopy is a useful tool in the areas of high cancer risk, but its usefulness has not been proven in the low- to moderate‑risk areas. The detection and treatment of early neoplasia is based on surveillance of esophageal and gastric precancerous conditions. One‑time gastroscopy at the age between 40 and 69 years could be a potentially effective method for searching for esophageal and gastric precancerous conditions.
Introduction
Upper gastrointestinal cancers are a frequent cause of cancer‑related deaths worldwide.1 In these diseases, the prognosis of survival generally remains poor, and it is closely related to the stage of the cancer.2 Esophagogastroduodenoscopy (EGD) is an essential examination for diagnosing and screening for upper gastrointestinal cancer, with the estimated adverse event rate as low as 0.009%.3 It has been proven that screening for gastric cancer is not only beneficial to the individual but also cost‑effective in high- and intermediate‑risk populations.4-7 It has been shown that endoscopic screening leads to a reduction in gastric cancer‑related deaths.7 Gastric cancer screening programs were implemented in South Korea and Japan.5-7 They offer population‑based screening starts at the age of 40 and 50, respectively. The most frequent type of gastric cancer is intestinal‑type gastric adenocarcinoma (GA), which develops in a multistep process called the “Correa cascade” from chronic inflammation (atrophic gastritis [AG] and intestinal metaplasia [IM]) through low‑grade and high‑grade dysplasia to cancer.8 Identification of high‑risk groups with extensive atrophy and IM is crucial in the surveillance strategy of non‑cardia GA.9 Similarly to GA, esophageal adenocarcinoma (EA), occurring within Barrett’s metaplastic mucosa, develops in a multistep process, and requires endoscopic surveillance and treatment of dysplasia to prevent cancer development.10 For both EA and GA, the opportunities for successful screening widened along with the improvement of endoscopic treatment of dysplasia. Several screening options have been worked out based on the detection of gastric and esophageal precancerous conditions.5,6,11,12 The aim of our study was to determine if the implementation of single‑time EGD to detect high‑risk conditions (AG, Barrett’s esophagus [BE]) might be beneficial in areas of moderate gastric cancer prevalence and low esophageal cancer prevalence areas.
Patients and methods
Databases
We used 2 databases to analyze patients with upper gastrointestinal neoplasms. The first database comprised retrospective data of the patients who underwent diagnostic EGD in 3 endoscopic centers: 1) an endoscopy unit of a tertiary university hospital, 2) an outpatient endoscopy clinic, or 3) an endoscopy unit of a district hospital. The examinations were performed from March 2018 to October 2019 by 32 operators who completed the endoscopic training (gastroenterology, general surgery, and internal medicine specialists). The patient personal data (age, sex) and endoscopic data, such as esophageal, gastric, and duodenal lesions or tumors and endoscopically suspected esophageal metaplasia were collected. Histopathologic reports provided information on the histologic type of the lesions and tumors, confirmed BE, AG, gastric IM, and dysplasia.
The patients were categorized into 4 groups based on the endoscopic and histopathologic findings. The control group consisted of the individuals who were not diagnosed with cancerous or precancerous conditions. Group 1 consisted of individuals diagnosed with precancerous conditions without dysplasia (BE, AG, IM). BE was diagnosed according to the European Society of Gastrointestinal Endoscopy criteria.9 Group 2 consisted of patients diagnosed with esophageal or gastric dysplasia, and group 3 included patients diagnosed with EA and non‑cardia GA. Given the feasibility of monitoring such precancerous conditions as BE and AG, we selected individuals with EA and non‑cardia intestinal‑type GA as target tumors that could be avoided. The patients with nonepithelial tumors, such as lymphomas, neuroendocrine tumors, and stromal tumors were not included in the assessment.
The second database was the national cancer registry (Krajowy Rejestr Nowotworów [KRN]), covering the years 2014 to 2017. Data extraction was based on the ICD‑10 code, sex, and age range, divided into 5‑year intervals. To evaluate morbidity, we compared the KRN data with national statistics for the general population (Statistics Poland, https://bdl.stat.gov.pl/bdl/dane/podgrup/temat).
As histopathologic records in the KRN could be biased by inaccurate or insufficient data entry, we extrapolated the data regarding histopathologic types of gastric and esophageal malignant neoplasms from a retrospective cohort. In the retrospective cohort, the number of cancers that developed from BE (EA) and AG (non‑cardia GA) was compared with the number of other types of malignant esophageal neoplasms (ICD code C15) and malignant gastric neoplasms (ICD code C16) to stratify the ratio of the listed neoplasms. Then, this number was assessed as the percentage value of tumors coded as C15 and C16 in the KRN database.
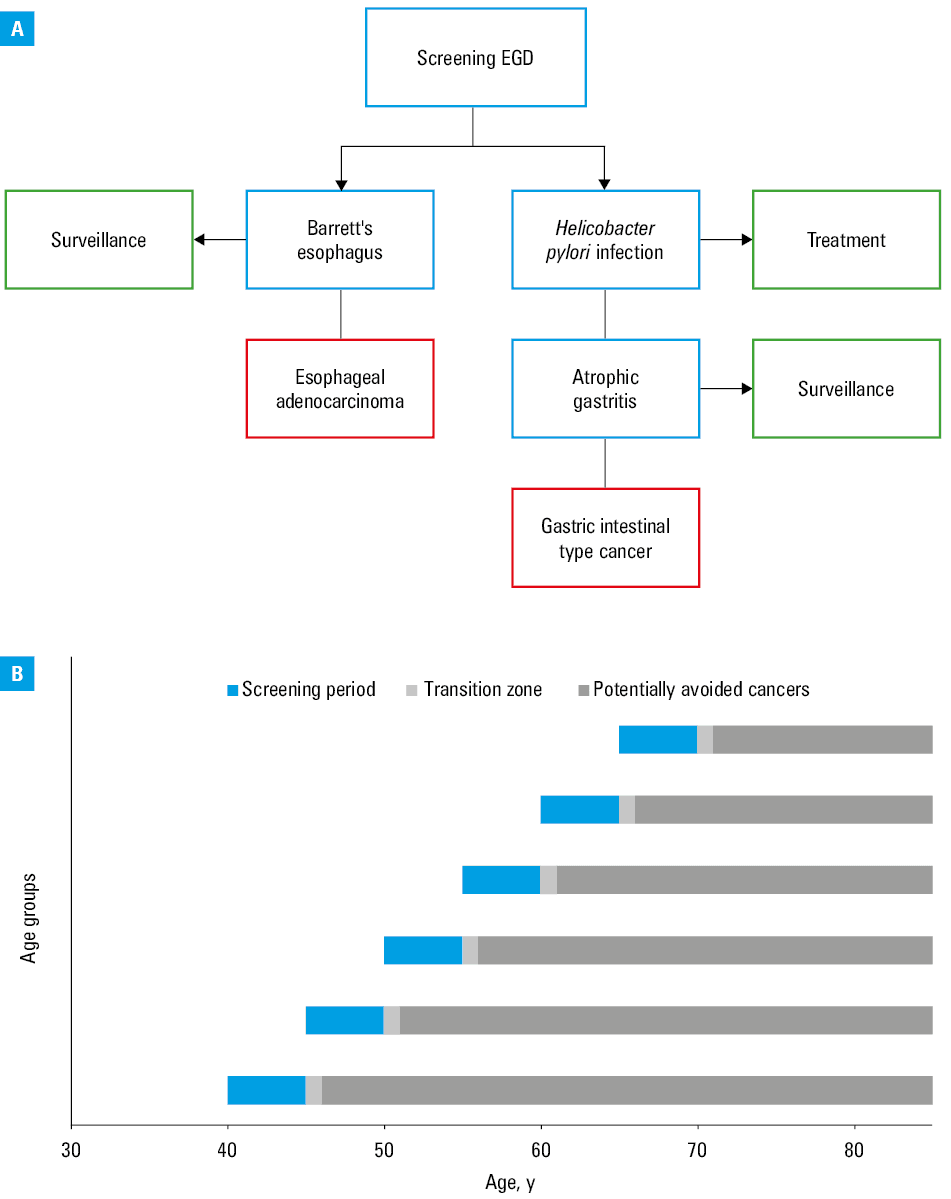
To select the optimal time frame, we analyzed the 2012 cohort of adults and divided them into 5‑year intervals starting at the age of 40 years. To avoid cases of initially symptomatic tumors and delayed diagnosis due to the first false‑negative histopathologic examination results, the first year (2013) was treated as a “transition” zone and was not analyzed. For the purpose of our study, we assumed that finding a precancerous condition (BE, AG) and its inclusion in our surveillance would be beneficial for the patient. The potential benefit‑to‑harm ratio of detecting the precancerous conditions was calculated as proportion of number of procedures per 1 avoided cancer and risk of complications related to EGD.3 The assumed additional benefit would be eradication of Helicobacter pylori, if present. The screening assumptions are summarized in Figure 1. The study was approved by the local ethics commission (PCN/022/KB/41/21), and obtaining the informed consent was waived. The study was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
The age of the patients was presented as mean (SD), while categorical values were presented as numbers and frequencies. Differences between independent groups were assessed by the χ2 test for categorical measures. The differences between quantitative variables were assessed by the Kruskal–Wallis test with the Dunn post hoc test for multiple comparisons. Simple logistic regression was performed to estimate the association between the outcomes (precancerous conditions, dysplasia, and cancers) and age categories. The odds ratios (OR) were presented with 95% CIs. A P value below 0.05 was considered significant throughout the analysis. All analyses were performed using SAS statistical package, version 9.4 (SAS Institute Inc., Cary, North Carolina, United States).
Results
Study group characteristics
A total of 5984 individuals who underwent diagnostic EGD were included in the study. The mean (SD)age of the whole study group was 56.1 (16.2) years, and 3265 participants (56.2%) were women. BE was diagnosed in 131 and AG in 707 cases (2.2% and 11.8%, respectively). Of the 26 identified cases of esophageal dysplasia (0.4%), 24 were dysplasia in BE (21 low‑grade dysplasia, 1 high‑grade dysplasia, and 2 cases of indefinite for dysplasia) and 2 cases were squamous intraepithelial high‑grade dysplasia. Of the 102 cases (1.7%), gastric dysplasia was identified as a macroscopic lesion in 14 cases. Esophageal tumors were found on 22 EGDs (0.4%), including 5 adenocarcinomas, 14 squamous cell carcinomas, 2 neuroendocrine tumors, and 1 stromal tumor. The most frequent histologic type of gastric tumor (0.7%) was adenocarcinoma (26 cases of which 23 were non‑cardia); the other types were 10 poorly cohesive / signet‑ring cell or mixed type carcinomas, 4 neuroendocrine tumors, 3 lymphomas, and 1 lung cancer metastasis.
Analysis of patient subgroups
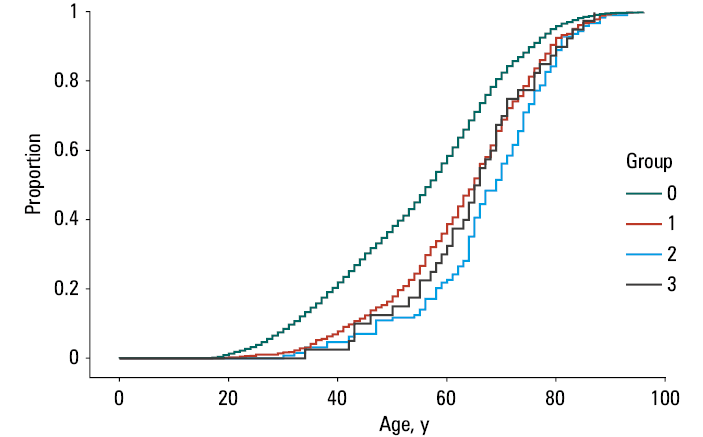
Women were found to be more prevalent in the control group than in the groups 1, 2, and 3 than men (85.2% vs 81.8% in the control group, respectively; P = 0.001). The characteristics of the groups are shown in Table 1. The mean age was significantly lower in the controls than in the patients with diagnosed precancerous conditions, dysplasia, and cancers, and in those diagnosed with precancerous conditions than those with diagnosed dysplasia. The age distribution in individual groups is presented in Figure 2. There was no relationship between the histologic type of esophageal or gastric cancers and the age of the patients (esophageal squamous cell carcinoma vs EA, non‑cardia GA vs other gastric cancers, both P = 0.12, and combined EA with non‑cardia GA compared with the other cancer types, P = 0.2).
Diagnosis | |||||||
Variable | Control (Group 0) | Precancerous conditions
(Group 1) | Dysplasia
(Group 2) | Cancers
(Group 3) | |||
Comparison of age in the group 0 (control) with the groups 1, 2, and 3, P <0.001; comparison of the groups 1 and 2, P = 0.004; the other comparisons P >0.05 | |||||||
Barrett’s esophagus | Atrophic gastritis | Esophageal dysplasia | Gastric dysplasia | Esophageal adenocarcinoma | Gastric
adenocarcinoma | ||
Patients, n | 5112 | 131 | 707 | 26 | 102 | 5 | 23 |
Age, y, mean (SD) | 54.9 (16.6) | 56.8 (14.4) | 64.1 (13.5) | 65.9 (10.2) | 67.5 (13.2) | 53.6 (13.4) | 67.5 (9.5) |
Women, n (%) | 2909 (56.9) | 46 (35.1) | 401 (56.7) | 9 (34.6) | 43 (52) | 0 | 7 (30.4) |
Age as a risk factor for cancerous and precancerous conditions
The univariable regression analysis was performed to assess the potential age thresholds for increased risk of precancerous conditions, dysplasia, and cancers (see Table 2). In comparison with patients under 40 years of age, an increased risk of detection of precancerous conditions (group 1) began at the age of 40 years, and of dysplasia (group 2), and cancer (group 3) at 55 and 60 years of age, respectively.
Age group, y | Precancerous conditions
(Group 1) | Dysplasia
(Group 2) | Cancers
(Group 3) | ||||||
OR | 95% CI | P value | OR | 95% CI | P value | OR | 95% CI | P value | |
Abbreviations: OR, odds ratio | |||||||||
<40 | Reference | Reference | Reference | ||||||
40–44 | 1.6 | 1.04–2.4 | 0.03 | 1.3 | 0.3–5.3 | 0.70 | 7.9 | 0.8–75.7 | 0.07 |
45–49 | 1.97 | 1.3–2.9 | <0.001 | 2.8 | 0.9–8.7 | 0.07 | 5.6 | 0.5–61.5 | 0.16 |
50–54 | 2.8 | 1.99–4.0 | <0.001 | 1.2 | 0.3–4.98 | 0.76 | 7.4 | 0.8–71.7 | 0.08 |
55–59 | 3.0 | 2.2–4.2 | <0.001 | 3.6 | 1.3–9.7 | <0.001 | 7.8 | 0.9–69.8 | 0.06 |
60–64 | 2.95 | 2.1–4.1 | <0.001 | 6.6 | 2.7–16.4 | <0.001 | 12.1 | 1.5–98.6 | 0.01 |
65–69 | 4.2 | 3.1–5.8 | <0.001 | 6.5 | 2.6–16.2 | <0.001 | 15.6 | 1.9–124.7 | 0.009 |
70–74 | 4.8 | 3.4–6.7 | <0.001 | 11.0 | 4.4–27.4 | <0.001 | 9.0 | 0.9–87.1 | 0.05 |
75–79 | 5.3 | 3.7–7.4 | <0.001 | 12.1 | 4.8–30.4 | <0.001 | 18.2 | 2.1–156.0 | 0.008 |
80–84 | 4.6 | 2.9–7.2 | <0.001 | 12.4 | 4.3–35.4 | <0.001 | 24.8 | 2.6–240.4 | 0.005 |
>84 | 6.5 | 3.9–10.9 | <0.001 | 13.6 | 4.0–45.7 | <0.001 | 16.3 | 1.01–263.7 | 0.04 |
Cancer registry database: an analysis of potential screening efficiency and age intervals
In the KRN database, 23 864 esophageal and gastric malignant neoplasms were found. Mean incidence of esophageal and gastric malignant neoplasms during the analyzed period in different age groups is presented in Figure 3. Of these, 10 480 were identified as potentially avoidable by screening implementation (EA or non‑cardia GA at the age of 45 years or higher). Six age intervals from 40 to 69 years were analyzed. The lowest number of procedures per 1 potentially avoidable cancer was 236 and 235 for the 40–44 years and 45–50 years age groups, respectively (see Figure 3).
Discussion
The idea of performing screening EGD to search for precancerous conditions or early cancers of the upper gastrointestinal tract has been discussed for some time. The available data originate mainly from the countries with high prevalence of such cancers, such as Japan and South Korea, where organized screening programs have been implemented.5 The impact of screening on the reduction of gastric cancer mortality has been shown in South Korea in patients with a wide age range of 40 to 74 years.7 In the countries with lower prevalence of gastric cancer, where screening could not be as effective, the idea of combining screening gastroscopy with screening colonoscopy has emerged.12,13 However, this approach was not found to be cost‑effective in the United States.12 Recently, a large cohort study from China has shown promising results of one‑time endoscopic screening in reducing esophageal and gastric cancer incidence and mortality.14 In that study, the number of screening EGDs needed to prevent a cancer diagnosis in a single patient was 98.14 In 2 studies, one‑time screening EGD was investigated.12,14 As most of the studies were performed in the countries with high prevalence of cancer, the results cannot be directly translated to the countries where cancer incidence is lower, such as Poland. In our study, we assumed that one‑time EGD could work as “mass triage” to identify individuals at a risk of esophageal or gastric cancer who have been diagnosed with BE or AG, respectively. Ideally, screening focused on the identification of dysplasia that would lead to an endoscopic treatment to prevent cancer development would be desirable. Unfortunately, our study showed that it might be impossible to select an age range for patients with elevated risk of dysplasia without significant risk of advanced cancer. However, the age at which the risk of detecting precancerous conditions (AG and BE) increased was lower than that for dysplasia and cancer diagnosis. Detecting precancerous conditions in younger patients than those with cancers is supported by a large retrospective study on IM and gastric cancer.15 Therefore, we suppose that performing one‑time EGD at the age when the risk of AG and BE starts to rise could lead to the selection of candidates for the endoscopic surveillance without a significant risk of finding an advanced tumor on screening EGD. We assumed that the potential screening period would end at the age of 69 based on cancer diagnosis risk which then becomes substantial. Both BE and AG are well‑recognized precancerous conditions. The annual risk of cancer development in BE is estimated at 0.61%, and in AG at around 0.25%.16,17 It is also worth mentioning that the increased risk of BE and AG diagnosis at the age of at least 40 years justifies the endoscopic diagnosis of symptomatic patients above that age limit. The proposed age threshold is coherent with sustained high sensitivity of diagnosis of advanced stages of AG or gastric dysplasia based on a biopsy at the age of at least 45 years or 40 years and endoscopic diagnosis of gastritis.18
H. pylori is the type 1 oncogene in the pathogenesis of gastric cancer (GC).19 GC unrelated to H. pylori is estimated to account for less than 1% of all GCs.20 Eradication therapy not only reduces the risk of developing AG and IM and decreases AG and IM severity, but it also shows a preventive potential in GC.21,22 Therefore, a secondary goal of potential screening would be a highly sensitive and specific diagnosis of H. pylori infection and providing eradication therapy to the infected patients.23
A potential obstacle to EGD as the mass screening could be the patient willingness to undergo this examination. We estimated the potential benefit‑to‑harm ratio by comparing the number of procedures needed to prevent 1 cancer by detecting a precancerous condition and the risk of complications. The ratio ranged between 28 and 47 in the examined age intervals, and was the highest in the age groups of 40–44 years and 45–49 years.
Limitations
Our study has several limitations. Firstly, it was a retrospective study on symptomatic patients. The prevalence of AG and BE might differ among symptomatic and asymptomatic individuals. This simplification results from the lack of data on asymptomatic individuals, as the screening gastroscopy is not available in Poland. Secondly, our methodology assumed that all cases of EA and non‑cardia GA would be avoided thanks to EGD in the patients aged at least 40 years. That stems from the lack of data on the expected development of precancerous conditions after negative index EGD. Also, potential bias of higher risk of cancers in men than in women, or other reported clinical factors cannot be omitted.24 Due to the retrospective nature of our study, the proportion of patients with a history of H. pylori infection could not be assessed. A close relationship between GC and H. pylori would suggest validity of referring patients for EGD based only on the infection diagnosed with noninvasive tests. However, BE development risk decreases with H. pylori infection, predominantly because of achlorhydria due to chronic inflammatory changes.25 This means that H. pylori –uninfected individuals are at a greater risk of BE development, and referring only the infected patients for EGD may lead to the exclusion of those at a greater risk of BE.
In conclusion, we demonstrated the potential efficacy of one‑time EGD as a “population triage.” We showed that the potential benefit‑to‑harm ratio of one‑time EGD could be as high as 28 to 47 in the age groups of 40 to 69 years. In the search for precancerous conditions, EGD may be considered one of the indications for the endoscopy of the upper digestive tract in a population with a low to moderate prevalence of esophageal and gastric cancer.
- Hyuna S, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021; 71: 209‑249. | Crossref
- Asplund J, Kauppila JH, Mattsson F, et al. Survival trends in gastric adenocarcinoma: a population‑based study in Sweden. Ann Surg Oncol. 2018; 25: 2693‑2702. | Crossref
- Sieg A, Hachmoeller‑Eisenbach U, Eisenbach T. Prospective evaluation of complications in outpatient GI endoscopy: a survey among German gastroenterologists. Gastrointest Endosc. 2001; 53: 620‑627. | Crossref
- Zhou L, Guan P, Sun LP, et al. Health economic assessment for screening of gastric cancer in a high risk population in northeastern China. Chin J Cancer Res. 2011; 23: 21‑24. | Crossref
- Huang HL, Leung CY, Saito E, et al. Effect and cost‑effectiveness of national gastric cancer screening in Japan: a microsimulation modeling study. BMC Med. 2020; 18: 257. | Crossref
ARTICLE INFORMATION