Outcomes of COVID-19 in patients vaccinated and unvaccinated against SARS-CoV-2 and suffering from pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension
Key words: chronic thromboembolic pulmonary hypertension, COVID-19, outcome, pulmonary arterial hypertension, vaccination



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Outcomes of COVID-19 in patients vaccinated and unvaccinated against SARS-CoV-2 and suffering from pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension
Introduction: Pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH) lead to progressive right heart failure. The mortality rates in PAH and CTEPH patients due to COVID‑19 are high, and vaccination against COVID‑19 is recommended in this group.
Objectives: We analyzed the incidence and outcomes of COVID‑19 in the PAH/CTEPH patients for 2 years of the pandemic, as well as the predictors of worse outcomes of COVID‑19 in this group.
Patients and methods: PAH/CTEPH patient data for this observational, cohort study were obtained from 3 pulmonary hypertension centers between March 11, 2020 and March 11, 2022.
Results: A total of 364 consecutive patients with PAH/CTEPH (248/122; 232 women [64%]; median [interquartile range] age, 61 years [18–92]) were included in the study. All the patients had advanced pulmonary hypertension at baseline. Eighty‑five patients (23%) suffered from COVID‑19. Seven of them (8%), all of whom were unvaccinated, died of COVID‑19. The unvaccinated patients suffered from COVID‑19 more often than the vaccinated ones (46% vs 9%; P <0.001). As many as 31% of the PAH/CTEPH patients with COVID‑19 needed hospitalization, in 8% of cases in the intensive care unit. Age equal to or above 65 years and severe pulmonary hypertension defined as a World Health Organization functional class 3 or 4 were associated with severe COVID‑19 in the PAH/CTEPH patients.
Conclusions: The vaccinated PAH/CTEPH patients suffered from COVID‑19 less frequently than the unvaccinated ones. The mortality rate and hospitalization due to COVID‑19 were higher in the PAH/CTEPH patients than in the general population. All efforts should be made to convince the PAH/CTEPH patients to vaccinate against COVID‑19.
What's new?
This observational, multicenter, cohort study was designed to follow the incidence and course of COVID‑19 in patients with pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH) during 2 years of the COVID‑19 pandemic. Only a few studies have examined the outcomes of COVID‑19 in the PAH/CTEPH patients, and none analyzed the impact of vaccination on COVID‑19 course. There is scarce evidence on the course of COVID‑19 in seriously ill PAH/CTEPH patients. We identified predictors of hospitalization and mortality due to COVID‑19. Severe PAH (defined as World Health Organization functional class 3 or 4), advanced age, and comorbidities were factors contributing to a more severe course of COVID‑19 in the PAH/CTEPH patients. To our knowledge, this is the first study on the course of COVID‑19 in the PAH/CTEPH patients that examines the impact of COVID‑19 vaccination on their morbidity and mortality. The results justify great efforts made to convince the PAH/CTEPH patients to vaccinate against COVID‑19.
Introduction
The first case of COVID‑19, which is caused by SARS‑CoV‑2, was recorded on November 17, 2019 in Wuhan, central China, while the first case in Poland was recorded on March 4, 2020.1 COVID‑19 was recognized as a pandemic by the World Health Organization (WHO) on March 11, 2020.2 Individuals with different underlying medical conditions, including chronic lung diseases, coronary heart disease, cancer, and cerebrovascular disease, have a higher risk of developing severe COVID‑19.3 Pulmonary hypertension (PH) is a severe disease characterized by an increase of the pressure in the pulmonary artery. Pulmonary arterial hypertension (PAH), which belongs to group 1 as per the clinical classification of PH by the WHO, is a rare disease characterized by progressive changes, which narrow the pulmonary arterial wall, and precapillary pulmonary hypertension, which leads to elevation of the pulmonary arterial pressure, pulmonary vascular resistance, and normal postcapillary wedge pressure.4,5 Chronic thromboembolic pulmonary hypertension (CTEPH), belonging to group 4 as per the clinical classification of PH according to the WHO, is a rare severe disease characterized by precapillary pulmonary hypertension caused by chronic occlusion with thromboembolic material located in the pulmonary arteries or their branches.4 Both groups of PH need specific treatment and frequent contact with medical staff. If left untreated, they may result in progressive right heart failure, overload, and poor outcome.4,6-8
During the first months of the COVID‑19 pandemic, there were reports from the United States and Europe of much higher mortality due to COVID‑19 in patients with PAH and CTEPH than in the general population.9,10 Only 1 study examined the impact of PH severity on COVID‑19 outcomes before vaccination.11 A high mortality rate may be the consequence of a more severe course of COVID‑19 in seriously ill PH patients, although limited diagnostic testing and control visits during the pandemic might have delayed PH diagnosis and early detection of the disease progression. Vaccination is strongly recommended by the WHO to prevent COVID‑19.12 Some experts suggested prioritization of COVID‑19 vaccination in the PAH/CTEPH patients with advanced disease or undergoing lung transplant evaluation.13 The COVID‑19 vaccination program in Poland started on December 27, 2020.14 In the beginning, only individuals aged over 80 years were eligible for vaccination. Younger adults were gradually incorporated, and from May 10, 2021 all adults in Poland were eligible for COVID‑19 vaccination.14,15
The aim of this study was to analyze the incidence and outcomes of COVID‑19 in PAH/CTEPH patients during 2 years of the pandemic. The analyses were based on the vaccination status and the impact of different predictors of severity on COVID‑19 outcomes.
Patients and methods
This observational, multicenter, cohort study was performed in 3 PH centers in Poland between March 11, 2020 (when the pandemic began) and March 11, 2022 (when the pandemic was considered to have ended). During this period, the PAH/CTEPH patients were admitted to the hospitals when the need arose, visited the outpatient clinics, or attended teleconsultations. The “starting point” of the observation for all PAH/CTEPH patients was March 11, 2020, when the pandemic began in Poland. Each patient was regularly followed‑up by the centers. The PH patients were in personal contact with the treatment center every 2 to 3 months before and during the pandemic, so if they did not die, they paid 6 to 8 visits to the center until March 11, 2022. Only for the first 3 months of the pandemic, the patients preferred telephone contact with the doctors. Later on, they paid personal visits to the centers or were hospitalized.
None of our 3 centers was dedicated to the treatment of COVID‑19 patients, so even if we diagnosed COVID‑19 in a PAH/CTEPH patient, they were transferred to another dedicated hospital or referred for outpatient treatment at home. If a patient suffered from COVID‑19 and was hospitalized, we analyzed their hospital discharge card. If they were treated on an outpatient basis, we used the medical records that they provided to us at the next PH visit and / or personal information from the patient. We received data on the patients who died from their family members or when contacting the family in order to confirm the date of the next PH follow‑up visit.
The patients were included in the study, if they had PAH/CTEPH according to the current guidelines,4 were aged at least 18 years, and were confirmed to have acute SARS‑CoV‑2 infection by a polymerase chain reaction test.
The study was of observational nature. All data regarding the medical history, clinical condition, present treatment, and comorbidities were obtained from the patients’ medical records and history of COVID‑19. All information about the number of doses, timing of vaccination against COVID‑19, and the relationship between the vaccination and SARS‑CoV‑2 infection was obtained from the patients, from the European Union Digital COVID Certificates, or from the gabinet.gov.pl application created by the Polish Ministry of Health. A patient was considered fully vaccinated 2 weeks after administration of the final dose in the primary vaccination series (at least 2 weeks after a single dose of the Johnson & Johnson vaccine or at least 2 weeks after the second dose of any other vaccine). The study design was approved by the Bioethics Committee of the Center of Postgraduate Medical Education, Otwock, Poland (KBE 23/2022) in accordance with the Declaration of Helsinki. Due to the retrospective character of the study, no written consent was obtained from the patients.
Statistical analysis
Distribution of the quantitative data was verified by the Shapiro–Wilk test in the entire sample, and then in the PAH/CTEPH patients with and without COVID‑19. In none of the cases the data followed normal distribution, so they were presented as medians with interquartile ranges (IQRs). Distribution of the qualitative variables was presented as percentages in the entire group and in the subgroups. Distribution of the quantitative data was compared with the Mann–Whitney test. The χ2 test was used to compare the frequencies of the qualitative trait categories. Logistic regression with dummy variables was used to identify predictors of hospitalization and mortality in the PAH/CTEPH patients with COVID‑19. The selected variables significant in univariable analysis were included in the multivariable analysis. Odds ratios with 95% CIs were calculated. All data analyses were performed with Stata Statistical Software, version 13.3 (TIBCO Software Inc., license acquired from a local distributor StatSoft, Kraków, Poland). The significance level was set at a P value below 0.05.
Results
Between March 11, 2020 and March 11, 2022, 378 PAH/CTEPH patients were considered for inclusion in the study. Twelve PAH/CTEPH patients were excluded, as they had had COVID‑19 before the diagnosis of PH. Next 2 patients were excluded due to the loss of their follow‑up data; they died, but the reason of death was unknown. Finally, 364 patients were included in further analysis (Figure 1). The study was performed in 3 PH centers in Poland; 300 patients (82%) were treated in the European Health Center in Otwock, 55 (15%) in the National Institute of Cardiology in Warsaw, and 9 (3%) in the Military Institute of Medicine in Warsaw. The median length of the follow‑up was 730 days (IQR, 601–730 days).
A total of 364 patients with PH group 1 and 4 (232 women, median age of 61 years [42–73]) were included in the study. Of those, 242 patients (66%) were diagnosed with PAH and 122 (34%) with CTEPH. All the patients had advanced PH at baseline. Eighty‑five patients (23%) suffered from COVID‑19, 19 (22%) of whom were vaccinated. The baseline characteristics of the entire study group and of the patients who did and did not suffer from COVID‑19 are shown in Table 1.
Parameter | Entire study group (n = 364) | Patients with COVID‑19 (n = 85) | Patients without COVID‑19 (n = 279) | P value (with vs without COVID‑19) | |
Data are shown as number (percentage) of patients unless indicated otherwise.
Differences were considered significant at P <0.05.
a Compared with the Mann–Whitney test
b PDE5‑I + ERA + prostacyclin analogue
c Riociguat or sildenafil
d Riociguat / sildenafil and treprostinil
Abbreviations: BPA, balloon pulmonary angioplasty; COPD, chronic obstructive pulmonary disease; CTEPH, chronic thromboembolic pulmonary hypertension; ERA, endothelin receptor antagonist; IPAH, idiopathic pulmonary arterial hypertension; PAH, pulmonary arterial hypertension; PAH‑CHD, pulmonary arterial hypertension related to congenital heart disease; PAH‑CTD, pulmonary arterial hypertension associated with connective tissue disease; PDE5‑I, phosphodiesterase type 5 inhibitor; PEA, pulmonary endarterectomy; portopulmonary PAH, pulmonary arterial hypertension associated with portal hypertension; WHO FC, World Health Organization functional class | |||||
Age, y, median (IQR) | 61 (42–73) | 57 (40–70) | 62 (43–74) | 0.09a | |
Female sex | 232 (64) | 57 (67) | 175 (63) | 0.46 | |
Duration of PAH/CTEPH, y, median (IQR) | 5.2 (2.2–11.2) | 6 (2.2–14.2) | 5.2 (2.2–10.2) | 0.08a | |
Vaccinated against COVID‑19 | 221 (61) | 19 (22) | 202 (73) | <0.001 | |
WHO FC | Median, IQR | 3 (2–3) | 3 (2–3) | 3 (2–3) | 0.23a |
I | 25 (7) | 3 (3.5) | 22 (8) | – | |
II | 154 (42) | 37 (43.5) | 117 (42) | ||
III | 160 (44) | 35 (41) | 125 (45) | ||
IV | 25 (7) | 10 (12) | 15 (5) | ||
PAH | Any type | 242 (66) | 63 (74) | 179 (64) | 0.08 |
Idiopathic or heritable PAH | 119 (49) | 27 (43) | 92 (51) | – | |
PAH associated with CHD | 72 (30) | 23 (37) | 49 (27) | ||
PAH associated with CTD | 42 (17) | 12 (19) | 30 (17) | ||
Portopulmonary PAH | 7 (3) | 1 (2) | 6 (3) | ||
Drug‑induced PAH | 1 (0.5) | 0 | 1 (0.5) | ||
PAH associated with HIV | 1 (0.5) | 0 | 1 (0.5) | ||
PAH monotherapy | Any drug | 76 (31) | 18 (29) | 58 (32) | 0.66 |
PDE5‑I | 36 (15) | 9 (14) | 27 (15) | – | |
ERA | 39 (16) | 9 (14) | 30 (17) | ||
Prostacyclin analogue | 1 (0.4) | 0 | 1 (0.5) | ||
PAH double‑combination therapy | Any combination | 100 (41) | 27 (43) | 73 (41) | 0.25 |
PDE5‑I + ERA | 78 (32) | 24 (38) | 54 (30) | – | |
PDE5‑I + prostacyclin analogue | 22 (9) | 3 (5) | 19 (11) | ||
PAH triple‑combination therapyb | 66 (27) | 18 (29) | 48 (27) | 0.65 | |
CTEPH | Any type | 122 (33.5) | 22 (26) | 100 (36) | 0.08 |
CTEPH‑PEA | 13 (11) | 3 (14) | 10 (10) | – | |
CTEPH‑BPA | 74 (61) | 16 (73) | 58 (58) | ||
CTEPH‑PEA and BPA | 12 (10) | 1 (5) | 11 (11) | ||
CTEPH monotherapyc | 85 (70) | 17 (77) | 68 (68) | – | |
CTEPH double‑combination therapyd | 2 (2) | 0 | 2 (2) | – | |
Anticoagulation | 172 (47) | 36 (42) | 136 (49) | 0.3 | |
Comorbidities | Any comorbidity | 229 (63) | 45 (53) | 184 (66) | 0.02 |
Arterial hypertension | 164 (45) | 33 (39) | 131 (47) | 0.18 | |
Diabetes | 57 (16) | 9 (11) | 48 (17) | 0.14 | |
COPD | 42 (11.5) | 4 (5) | 38 (14) | 0.02 | |
Coronary artery disease | 57 (16) | 11 (13) | 46 (16.5) | 0.43 | |
Neoplasm | 48 (13) | 8 (9) | 40 (14) | 0.24 | |
Obesity | 94 (26) | 21 (25) | 73 (26) | 0.78 | |
Depression | 45 (12) | 14 (16.5) | 31 (11) | 0.18 | |
The unvaccinated patients more often suffered from COVID‑19 than the vaccinated ones (n = 66/143 [46%] vs n = 19/221 [9%]; P <0.001). Vaccination was a factor that lowered the risk of COVID‑19 in the patients with PAH and CTEPH in the univariable and multivariable logistic regression models. Risk factors for COVID‑19 in the PAH/CTEPH patients are presented in Table 2.
Parameter | Univariable model | Multivariable model | ||
OR (95% CI) | P value | OR (95% CI) | P value | |
Differences were considered significant at P <0.05.
a Arterial hypertension, diabetes, chronic obstructive pulmonary disease, coronary artery disease, neoplasm, obesity, and depression
Abbreviations: OR, odds ratio; PH, pulmonary hypertension; others, see Table 1 | ||||
Age ≥65 y | 0.8 (0.4–1.2) | 0.35 | – | – |
Female sex | 1.2 (0.7–2) | 0.46 | – | – |
Group of PH, PAH | 1.6 (0.9–2.7) | 0.09 | – | – |
WHO FC 3 or 4 | 1.1 (0.7–1.8) | 0.65 | – | – |
Comorbiditiesa | 0.6 (0.4–0.9) | 0.03 | 0.5 (0.2–0.8) | 0.009 |
Vaccination | 0.1 (0.06–0.1) | <0.001 | 0.1 (0.05–0.1) | <0.001 |
Anticoagulation | 0.8 (0.4–1.2) | 0.3 | – | – |
Combination PAH therapy | 1.4 (0.7–3) | 0.37 | – | – |
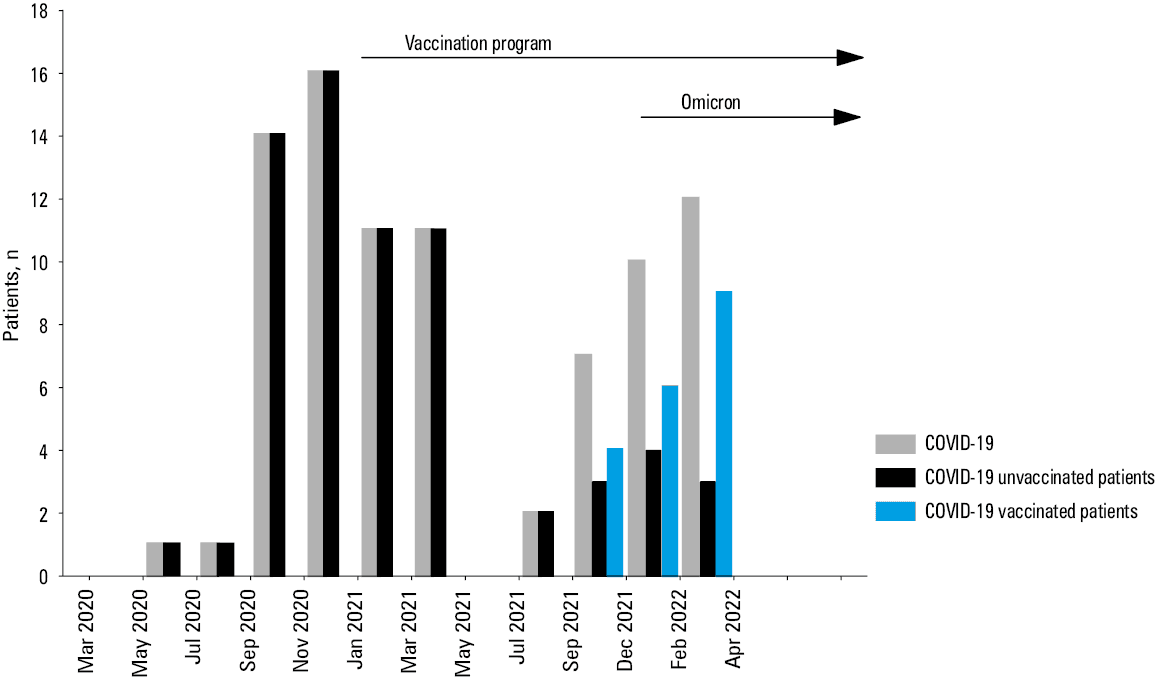
Eighty‑five PAH/CTEPH patients (23%) suffered from COVID‑19 during 2 years of the pandemic. Thirty‑two of these patients (38%) had been ill before the vaccination program started, 53 (62%) when immunization was available, and 22 (26%) when the Omicron variant of SARS‑CoV‑2 appeared. In the period before the vaccination program implementation, 41% of the patients who contracted COVID‑19 needed hospitalization, while 22% needed intensive care. All the patients in the intensive care died, whereas the mortality rate among the hospitalized individuals was 54%. After the commencement of the COVID‑19 immunization program, 24.5% of the patients needed hospitalization, no patient was referred to the intensive care unit (ICU), and no patient died due to SARS‑CoV‑2 infection. Two patients contracted COVID‑19 twice. The first time, both were unvaccinated and needed hospitalization due to pneumonia. They were both vaccinated the second time; the effects of the disease were then milder, and the patients were treated at home. Since they were unvaccinated the first time, both were assigned to the unvaccinated group. Time to COVID‑19 infection in the vaccinated and unvaccinated PAH/CTEPH patients during 2 years of the pandemic is presented in Figure 2.
By March 11, 2022, 281 (85%) out of the 332 surviving PAH/CTEPH patients had been fully vaccinated against COVID‑19. The main reason for refusing to get vaccinated was awareness of the side effects of the vaccines. In the unvaccinated subgroup, 33% of the patients needed hospitalization, while 11% needed intensive care; all patients in the ICU eventually died. No one in the vaccinated PAH/CTEPH group died of COVID‑19; 21% of the patients needed hospitalization but no one was referred to the ICU. COVID‑19 course in the entire group, as well as the vaccinated and unvaccinated subgroups, is presented in Table 3.
Parameter | Total COVID‑19 (n = 85) | Unvaccinated COVID‑19 (n = 66) | Vaccinated COVID‑19 (n = 19) | P value (unvaccinated vs vaccinated) |
Data are shown as number (percentage) of patients.
a New oxygen or increase of the dosage of used oxygen
b More than 3 months after COVID‑19 infection
Abbreviations: HF, heart failure; ICU, intensive care unit; others, see Table 1 | ||||
Death due to COVID‑19 | 7 (8) | 7 (11) | 0 | 0.14 |
Hospitalization due to COVID‑19 | 26 (31) | 22 (33) | 4 (21) | 0.3 |
ICU admission | 7 (8) | 7 (11) | 0 | 0.14 |
No ICU | 19 (22) | 15 (23) | 4 (21) | 0.87 |
Home treatment due to COVID‑19 | 59 (69) | 44 (67) | 15 (79) | 0.3 |
Additional oxygena | 27 (32) | 23 (35) | 4 (21) | 0.25 |
Pneumonia due to COVID‑19 | 25 (29) | 21 (32) | 4 (21) | 0.36 |
Aggravation of right HF due to COVID‑19 | 17 (20) | 13 (20) | 4 (21) | 0.89 |
Persistent decrease of WHO FCb | 18 (21) | 17 (26) | 1 (5) | 0.055 |
Change in PAH/CTEPH treatment | 8 (9) | 8 (12) | 0 | 0.11 |
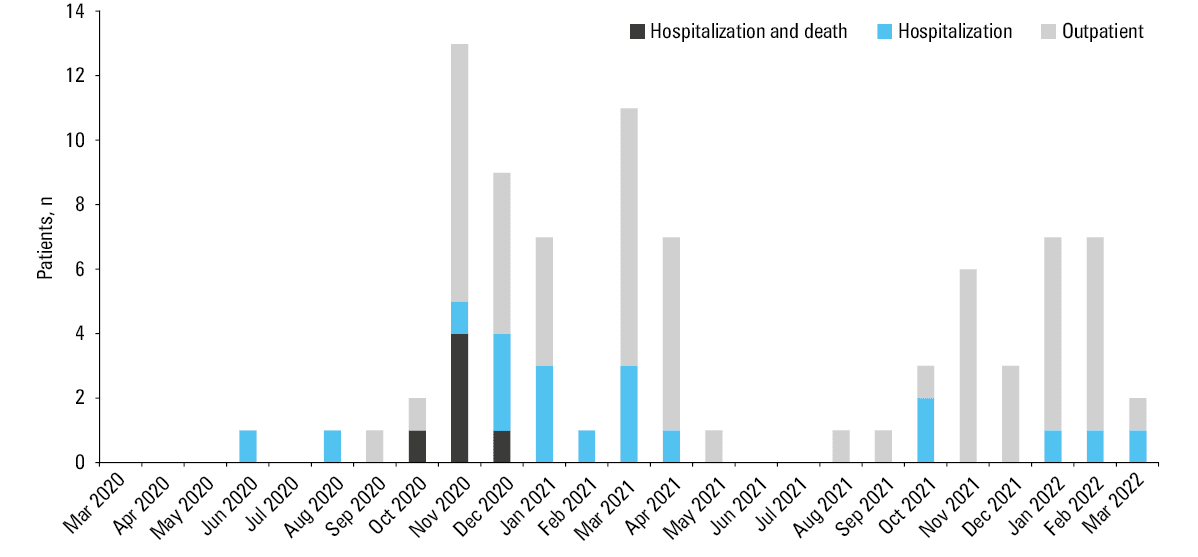
A severe course of COVID‑19 that necessitated hospitalization was observed in 26 patients (31%). Seven COVID‑19 patients (8%) died, all of them in the first year of the pandemic, before the vaccination program. Six patients died in the hospital, and 1 a few weeks after discharge from the hospital due to COVID‑19 complications. The hospital mortality rate was 23%. All the patients who died of COVID‑19 were elderly, aged from 66 to 90 years, with the WHO functional class 3 or 4, and unvaccinated. About 85% of these patients suffered from comorbidities. Three of them had idiopathic PAH, 3 had PAH due to connective tissue disease, and 1 had CTEPH. Figure 3 shows the clinical course of COVID‑19 in the PAH/CTEPH patients.
Advanced age and severe PH were associated with a more severe course of COVID‑19 in the logistic regression model. No protective effect of anticoagulation or PH type on the course of the disease was observed. Univariable and multivariable analyses of the variables associated with a more severe course of COVID‑19 in the PAH/CTEPH patients are presented in Table 4.
Parameter | Univariable model | Multivariable model | ||
OR (95% CI) | P value | OR (95% CI) | P value | |
Differences were considered significant at P <0.05.
| ||||
Age ≥65 y | 7.2 (2.6–20.1) | <0.001 | 3.5 (1.1–11) | 0.03 |
Female sex | 0.7 (0.3–1.8) | 0.47 | – | – |
PAH | 0.5 (0.2–1.5) | 0.22 | – | – |
WHO FC 3 or 4 | 2.9 (2–18.4) | 0.001 | 3.8 (1.1–12.9) | 0.02 |
PAH combination therapy | 0.7 (1.2–3.2) | 0.71 | – | – |
Vaccination | 0.5 (0.2–1.8) | 0.31 | – | – |
Anticoagulation | 0.9 (0.3–2.5) | 0.99 | – | – |
Comorbidities | ||||
Any comorbidity | 6.1 (2–16) | 0.001 | 3.2 (0.9–11.2) | 0.06 |
Arterial hypertension | 5.1 (1.8–13.6) | 0.001 | – | – |
Diabetes | 2 (0.4–8) | 0.34 | – | – |
COPD | 2.4 (0.3–17.8) | 0.40 | – | – |
Coronary artery disease | 5 (1.3–19.2) | 0.01 | – | – |
Neoplasm | 2.5 (0.6–10.9) | 0.24 | – | – |
Depression | 1.8 (0.6–6.2) | 0.18 | – | – |
Obesity | 2.7 (1–7.6) | 0.055 | – | – |
Vaccination | 0.5 (0.2–1.8) | 0.31 | – | – |
Anticoagulation | 0.9 (0.3–2.5) | 0.99 | – | – |
Discussion
This multicenter observational study followed the incidence and outcomes of COVID‑19 among the PAH/CTEPH patients during 2 years of the pandemic. The univariable and multivariable analysis showed that the vaccinated patients were well protected against COVID‑19. A total of 85 PAH/CTEPH patients (23%) contracted COVID‑19 during the study period. Of those, 32 individuals (38%) had contracted COVID‑19 before the vaccination program, and 53 (62%) became ill when the immunization was available. Vaccination against COVID‑19 in PAH/CTEPH patients is recommended based on expert opinion and observations from the general population.13,16,17 Experts suggest prioritization of vaccination for the patients with heart failure, including PAH and CTEPH, especially those in the New York Heart Association (NYHA) functional class 3 or 4, advanced in age, and with comorbidities.13,16,17 Our results confirm the validity of these recommendations. The PAH/CTEPH patients in the functional class 3 or 4 who were advanced in age (≥ 65 years) and had comorbidities were at a significantly higher risk of severe COVID‑19 outcomes, with a higher risk of hospitalization or death.
Unexpectedly, the multivariate analysis showed that not only vaccination but also the presence of comorbidities reduced the risk of COVID‑19 in the study group. At first, we hypothesized that the patients with comorbidities were most likely to be vaccinated against COVID‑19, because they were aware of the severe course of the disease due to comorbidities, but the subanalysis did not confirm this hypothesis. There were no differences in the vaccination rates in the PAH/CTEPH patients with and without comorbidities. Currently, there remains only 1 logical theoretical explanation, which has been confirmed by clinical practice. The PAH/CTEPH patients with comorbidities have been educated on their condition and are aware of the related risks, and they strictly respect social distancing, sanitary regime, isolation, and all other relevant instructions. A comorbid condition, chronic obstructive pulmonary disease (COPD), has been found to be associated with a reduced risk of COVID‑19 in the PAH/CTEPH patients in the multivariate logistic regression analyses. This is probably because the patients with complex medical problems tended to adhere to the principles of lockdown, isolation, and social distancing more strictly. It may also justify a reduction in hospitalized COPD exacerbations during COVID‑19 in the general population.18 During the restrictive lockdown, no cases of COVID‑19 were reported in the patients with PAH/CTEPH.
In this study, 12% of the PAH/CTEPH patients suffered from COVID‑19 during the first year, and 11% during the second year of the pandemic. This percentage is extremely high, as compared with other PAH/CTEPH surveys and the general population.19 In a survey by Lee et al,9 the incidence of COVID‑19 in the PAH and CTEPH patients in the United States was estimated at 2.9 cases per 1000 patients, which was similar to that in the general population.10 Farmakis et al20 reported a 3.6% incidence of COVID‑19 in the patients with PH group 1 and 4 in Greece, which was a little less than in the general population. Montani et al11 reported that 2.9% of PH patients with precapillary hypertension in France were diagnosed with COVID‑19, a Figure higher than the incidence in the general population. While we observed our PAH/CTEPH patients for 2 years of the pandemic, other authors collected data only in the early months of the pandemic, or before the vaccines rolled out.
The main reason for high incidence of COVID‑19 in our study might be low vaccination rate in both the PAH/CTEPH patients and the general population of Poland. The Food and Drug Administration first granted emergency use authorization for the Pfizer–BioNTech vaccine on December 10, 2020, and mass vaccinations in the United States began 4 days later. In Poland, first set of people to receive the vaccination were medical professionals, on December 27, 2020, after which the vaccination for elderly people gradually began. From May 10, 2021 all Polish adult inhabitants were eligible for vaccination.14,15 By the end of our observation, on March 11, 2022, only 58.7% of the population of Poland had received 2 doses of the vaccine, and the population immunity had not been achieved.21 Around the same time in Greece the corresponding Figure was 70.6%, while in the USA and France it reached 66.1% and 79.7%, respectively. In Poland, there was no vaccination prioritization for the PAH/CTEPH patients, even if they were seriously ill, except for the patients waiting for a lung transplant. At the end of our study, 85% of the PAH/CTEPH patients had been vaccinated, but in mid‑June 2021 the Figure was only 43%.22 Some of the previously unvaccinated patients changed their minds after they contracted COVID‑19, and some as a result of informative campaigns organized at the study centers. In our previous paper, we tried to identify clinical and demographic factors that might have impacted the vaccination decisions of the PAH/CTEPH patients. Only age equal to or above 60 years increased willingness to vaccinate against COVID‑19 in these individuals.22 The vaccines are less effective against the Omicron variant of SARS‑CoV‑2.23 We did not examine the SARS‑CoV‑2 variant that infected the patients in our study group, but 22 PAH/CTEPH patients (26%) were diagnosed with COVID‑19 when the Omicron variant was reported in Poland. When we focused on morbidity due to COVID‑19 among the PAH/CTEPH patients, we noted 2 waves of COVID‑19. The first one occurred before the vaccination program, and the second coincided with the time the Omicron variant appeared, and most of the patients needed an additional booster dose. In our study, data about preventive behaviors, such as using masks and physical distancing, that could have influenced the results, were not collected.
The mortality rate due to COVID‑19 in the PAH/CTEPH patients was 8% during 2 years of the pandemic, 16.2% in the first year, and 0% in the second year. The 2‑year Figure is much higher than the one in the general population of Poland, which was around 2%.19 It was similar to the mortality rate in a cohort of PAH/CTEPH patients in Spain (8%), but lower than in previous reports on PAH/CTEPH patients in the United States (12%), Europe (19%), France (24.6%), and Greece (22%).9-11,20 The hospitalization rate due to COVID‑19 in our group was 31%, which was similar to the rate described in the United States survey (30%), but lower than the rates reported in the surveys on the European (63%), French (60%), Greek (44%), and Spanish (70%) patients.9-11,20,24 Several factors might have impacted our results. We analyzed data from 2 years of the pandemic, from before and during the vaccination program, and when the Omicron SARS‑CoV‑2 variant appeared. The Omicron variant is highly transmissible but has significantly lower infection fatality rates than previous variants of SARS‑CoV‑2.23 The first case of the Omicron variant in Poland was confirmed on December 16, 2021. None of our PAH/CTEPH patients who were infected with SARS‑CoV‑2 died after this date due to COVID‑19. Other studies on the incidence and outcomes of COVID‑19 in PAH/CTEPH patients focused only on the first months of the pandemic before the vaccination programs. Some authors underlined that continuous expert care is crucial for good PH control and that noncompliance with or delay in elective hospital procedures might be harmful for PH patients and worsen their prognosis. From the beginning of the pandemic, the patients in our centers could choose between a personal visit to the referral center and teleconsultation. In the first 3 months of the pandemic, 54% of the patients preferred telephone contact, but after this period direct visits to centers were preferred. For 2 years of the pandemic, total mortality from all causes in the study group was 12%. This implies that 10% of the patients died from causes other than COVID‑19, 5% each year. This mortality rate did not differ significantly from that among the PAH/CTEPH patients before the pandemic.
Risk factors for a severe course of COVID‑19 were identified. A general risk factor of advanced age identified the PAH/CTEPH patients with a higher risk of hospitalization or death. Advanced age and presence of comorbidities determined in‑hospital mortality rate in the general population.25,26 Similar observations were published by Montani et al11 in a prospective cohort study of PH patients with precapillary hypertension, where in‑hospital mortality due to COVID‑19 was determined by advanced age, male sex, and comorbidities. Contrary to that, we identified impaired WHO functional class 3 or 4 as a factor of severe COVID‑19 outcome. Advanced NYHA/WHO functional class 3 or 4 predicts poor survival in PAH/CTEPH patients without COVID‑19.27 The type of PH did not determine the course of COVID‑19 either in our or study pr that by Montani et al11.
COVID‑19 increases the risk of venous thromboembolism (VTE), pulmonary embolism and / or deep venous thrombosis.28 A meta‑analysis disclosed around 15% rate of VTE events during COVID‑19.29 VTE worsens the prognosis of COVID‑19 patients.28,30,31 Some authors suggested that anticoagulation before COVID‑19 infection and hospitalization may protect against microthrombi and development of thromboembolic diseases during COVID‑19, and may decrease the risk of severe disease and death due to COVID‑19.32 Other studies did not confirm this theory.33,34 A therapeutic dose of anticoagulation may improve the course of COVID‑19 in hospitalized patients, especially when there is no need of ICU hospitalization.35 We observed no VTE cases being consequences of COVID‑19 in our PAH/CTEPH study group. However, not all patients had computed angiography performed, even if they were hospitalized, so the data could have been underestimated. About 47% of our PAH/CTEPH patients, and 45% of those who suffered from COVID‑19, received anticoagulants due to CTEPH, history of VTE, or atrial fibrillation. Only 2 of the 7 patients who died from COVID‑19 were taking anticoagulants. We found no impact of anticoagulation on either morbidity or severe course of COVID‑19. This is in accordance with previous studies in the general population.33,34 No thromboembolic events due to COVID‑19 were reported in the European population of PAH/CTEPH patients described by Belge et al10 or by Farmakis et al.20 Montani et al11 reported acute VTE in 4% of hospitalized PH patients. Anticoagulation was more frequently used in the hospitalized patients who survived than in those who died due to COVID‑19 at the hospital, but it had no impact on in‑hospital mortality in the multivariate regression model.11
Study limitations
The main limitation of our study is its retrospective design. The examined PAH/CTEPH group was relatively small, but the patients were followed for 2 years of the pandemic. The patients were tested for SARS‑CoV‑2 infection before hospitalization, if they or their relatives had symptoms suggesting COVID‑19, so asymptomatic patients could have been omitted. The study survival analysis would be the best type of analysis, but we decided to use logistic regression model due to problems with assessing the length of the follow‑up (to compare the vaccinated and unvaccinated patients, the follow‑up should start for the vaccinated individuals at the date of achieving the fully vaccinated status). The patients were vaccinated at different times, so we could only analyze the incidence of COVID‑19 and the course of the disease before and after vaccination, not at a specific time point for the entire study population. We included 66 patients diagnosed with PH after the start of the pandemic with negative COVID‑19 history. Negative COVID‑19 history was confirmed by the attending physician and checked in the central register of COVID‑19 cases of the Polish Ministry of Health. We assumed that the patients had had PH before the pandemic, because it is known from Polish and international registries that PH is a heterogenous disease diagnosed with a long delay. The median time from the onset of symptoms to diagnosis of PH is 12 to 14 months.36,37 In all 66 retrospectively enrolled PAH/CTEPH patients the first symptoms occurred several months before the onset of the pandemic.
Conclusions
Our findings are important for the PAH/CTEPH patients and their doctors in the next stages of the pandemic. We confirmed that the vaccinated PAH/CTEPH individuals were well protected against COVID‑19. The PH patients had a higher mortality risk and hospitalization rate due to COVID‑19 than the general population. The elderly patients in the functional NYHA/WHO class 3 or 4, had the highest risk of a severe course of COVID‑19. They should receive the greatest attention during PH center visits. All efforts should be made to convince the PAH/CTEPH patients to vaccinate against COVID‑19.
- Website of the Republic of Poland. Coronavirus: vaccinations and important information [in Polish]. https://www.gov.pl/web/zdrowie/pierwszy‑przypadek‑koronawirusa‑w‑polsce. Accessed Apr 3, 2022.
- World Health Organization General Director‑Speeches. General’s opening remarks at the media briefing on COVID‑19 ‑ 11 March 2020. https://www.who.int/director‑general/speeches/detail/who‑director‑general‑s‑opening‑remarks‑at‑the‑media‑briefing‑on‑covid‑19–11‑march‑2020. Accessed April 3, 2022.
- Flaherty GT, Hession P, Liew CH, et al. COVID‑19 in adult patients with pre‑existing chronic cardiac, respiratory and metabolic disease: a critical literature review with clinical recommendations. Trop Dis Travel Med Vaccines. 2020; 6: 16. | Crossref
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022; 43: 3618‑3731.
- Humbert M, Guignabert C, Bonnet S, et al. Pathology and pathobiology of pulmonary hypertension: state of the art and research perspectives. Eur Respir J. 2019; 53: 1801887. | Crossref
ARTICLE INFORMATION