Comparison of the population of Polish patients participating in the TRANSITION study with the international population: a post hoc analysis
Key words: acute heart failure, angiotensin receptor–neprilysin inhibitor, heart failure with reduced ejection fraction, sacubitril / valsartan, TRANSITION study



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Comparison of the population of Polish patients participating in the TRANSITION study with the international population: a post hoc analysis
Introduction: Heart failure (HF) patients discharged from a hospital are at a high risk of death and rehospitalization. Scarce data are available on the use of sacubitril / valsartan in this population in Poland.
Objectives: The aim of this study was to compare the efficacy and tolerability of sacubitril / valsartan in the group of Polish patients who participated in the TRANSITION study with the patients recruited at other sites.
Patients and methods: This is a post hoc secondary analysis of the TRANSITION study comparing sacubitril / valsartan initiation pre- vs postdischarge in 991 patients hospitalized for acute decompensated HF with reduced ejection fraction (HFrEF). The Polish subgroup consisted of 104 patients.
Results: Significant differences were identified in the characteristics of Polish vs non‑Polish populations. At baseline, the Polish population showed higher proportion of men, higher body mass index, lower heart rate, N‑terminal pro–B‑type natriuretic peptide and high‑sensitivity troponin T levels, and significantly lower New York Heart Association class. The Polish patients were better managed in terms of implanted electrotherapy devices, percutaneous coronary interventions, and drug therapy, and were more often hospitalized. The primary end point of achieving the target dose of sacubitril / valsartan at treatment week 10 was met by 45.6% of the Polish patients and 48.4% of the non‑Polish population (P = 0.61). Approximately 90% of the Polish patients received and maintained any sacubitril / valsartan dose for 2 weeks over 10‑week treatment vs 87.5% of the non‑Polish patients (P = 0.36). The rate of permanent sacubitril / valsartan treatment discontinuation was low in both Polish (3.9%) and non‑Polish populations (6.4%) (P = 0.33).
Conclusions: Sacubitril / valsartan can be used safely in the early period after an episode of acute HF both in the Polish and non‑Polish patients with HFrEF, and the likelihood to achieve the maximum dose is the same despite significant differences between the studied populations.
What's new?
Drugs introduced into clinical practice have rarely been tested in national populations. It is generally assumed that the results of pivotal studies are the same in different populations. Due to the considerable population of patients in the TRANSITION study recruited at Polish sites, a post hoc analysis was performed to compare the efficacy and safety of sacubitril / valsartan in the group of Polish patients with the patients recruited at other sites. This analysis provides additional information both on the patient characteristics and efficacy and safety of early sacubitril / valsartan initiation after an acute heart failure episode in the population of Polish patients with heart failure with reduced ejection fraction. To the best of our knowledge, the only comparison of Polish patients with the patients from other countries participating in the Heart Failure Pilot Survey was published in 2013. In addition, it is one of the few analyses concerning the Polish experience with the use of this modern treatment.
Introduction
A recent study by Puch‑Walczak et al1 assessing the current prevalence of heart failure (HF) in the general population of Poland shows that a diagnosis of HF was reported by 4.3% of the NATPOL 2011 study participants and 2.4% of the cases were confirmed by the National Health Fund database. HF remains a significant medical problem with an increasing number of cases, frequent hospitalizations, and poor prognosis.2,3 Patients discharged from a hospital after acute decompensation of HF (ADHF) are at a particularly high risk of death and rehospitalization. During the first 30 days after hospital discharge (ie, in the so‑called vulnerable phase), approximately 25% of the patients are rehospitalized due to ADHF, and the mortality rate during this period is about 10%.2,4 Therefore, the recommendations of scientific societies highlight the important role of initiation and optimization of treatment in accordance with the guidelines even before the patient is discharged.5,6 Recent years have brought further advances in the treatment of this condition. One of the developments was an extension of pharmacotherapy recommended in HF with reduced ejection fraction (HFrEF) with a new class of drugs, that is, sodium‑glucose cotransporter 2 (SGLT‑2) inhibitors. The other was a conclusion that HFrEF treatment with sacubitril / valsartan can be effectively and safely initiated in patients with de novo HF and in patients hospitalized for ADHF.5,7 The PIONEER‑HF study,8 comparing the effects and safety of angiotensin receptor‑neprilysin inhibitors (ARNIs) with enalapril in an ADHF population, showed that early initiation of sacubitril / valsartan treatment in hemodynamically stable patients during hospitalization is not only safe but also entails significant reductions in the risk of rehospitalization and death during the first 3 months after discharge. The multicenter, international, randomized TRANSITION trial,9 designed to compare 2 strategies for ARNI treatment initiation in patients hospitalized for ADHF after hemodynamic stabilization (predischarge and shortly postdischarge), demonstrated that both strategies were equally effective in achieving the target dose of sacubitril / valsartan of 97/103 mg twice daily (bid) over 10 weeks. Treatment tolerance, as measured by the rate of adverse events (AEs) and treatment discontinuation, were similar in both arms.
Drugs implemented into clinical practice are rarely tested at a national level. It is generally presumed that the outcomes of general studies are the same in different populations. As a considerable proportion of patients was recruited at Polish sites (10% of all TRANSITION study participants), a post hoc analysis was carried out to compare the efficacy and safety of sacubitril / valsartan in the group of patients recruited in Poland with the patients recruited in the other 18 countries participating in the TRANSITION study. To the best of our knowledge, the only comparison of the Polish patients with the patients from the other countries participating in the Heart Failure Pilot Survey (ESC‑HF Pilot) was published in 2013.10
Patients and methods
The TRANSITION study was an international, phase IV, randomized, multicenter, open‑label study aimed to generate complementary safety and tolerability data on sacubitril / valsartan initiation and uptitration to 97/103 mg bid target dose in hemodynamically stabilized patients with HFrEF recently hospitalized for an acute HF episode. The study was conducted in 19 countries and 156 hospital centers worldwide. All participants were randomized 1:1 to predischarge (in‑hospital) vs postdischarge initiation of sacubitril / valsartan, stratified by prior renin‑angiotensin‑aldosterone system (RAAS) status. The study design encompassed 2 parts. Part 1 was a 10‑week treatment initiation period (The Treatment Epoch), and part 2 was continuation during a 16‑week follow‑up treatment. The primary objective of the study was to evaluate the proportion of patients in the predischarge and postdischarge treatment groups achieving the target dose of sacubitril / valsartan 97/103 mg bid at week 10 after randomization, regardless of previous temporary dose interruption or downtitration. The study design and rationale have been published previously.11
This post hoc secondary analysis compared the Polish population with the non‑Polish population of the TRANSITION study and the predischarge and postdischarge treatment groups of the Polish cohort. The Polish subset of patients was recruited in 7 hospital centers in Poland and comprised 10% (104/991 patients) of all study participants. The study was conducted in accordance with the International Council for Harmonisation Harmonized Tripartite Guidelines for Good Clinical Practice and with the ethical principles of the Declaration of Helsinki. The trial protocol was approved by ethics committees at the participating centers. All participants of the study gave their written informed consent. The primary results of the TRANSITION study were published elsewhere.9
Statistical analysis
The size of the international (non‑Polish) population was calculated by subtracting the Polish population from the population of the entire TRANSITION study. The full analysis data set (FAS) consisting of all randomized patients, except for those randomized inadvertently, was used for the analysis of the demographic data. The safety data set consisting of all patients included in the FAS who received at least 1 dose of the study medication was used for the primary and secondary end point analysis (Figure 1). Treatment group comparisons have been performed using the χ2 test for categorical variables and the t test for continuous variables. For the data expressed as mean (SD), the analysis of variance with the Tukey Honest Significant Difference method, if applicable, was performed. The risk ratio (RR, probability ratio of achieving the target dose at the end of week 10 in the predischarge vs the postdischarge initiation group) was estimated with a 2‑sided 95% CI along with the estimated probability and 95% CI for each treatment group. In the case of the variable “Permanently discontinued sacubitril / valsartan due to AEs” zero‑cell corrections have been applied by adding a fixed value of 0.5. A 2‑tailed P value below 0.05 was considered significant for all tests.
Statistical analysis was performed using SAS software v.9.4 (SAS Institute Inc., Cary, North Carolina, United States).
Results
Study population
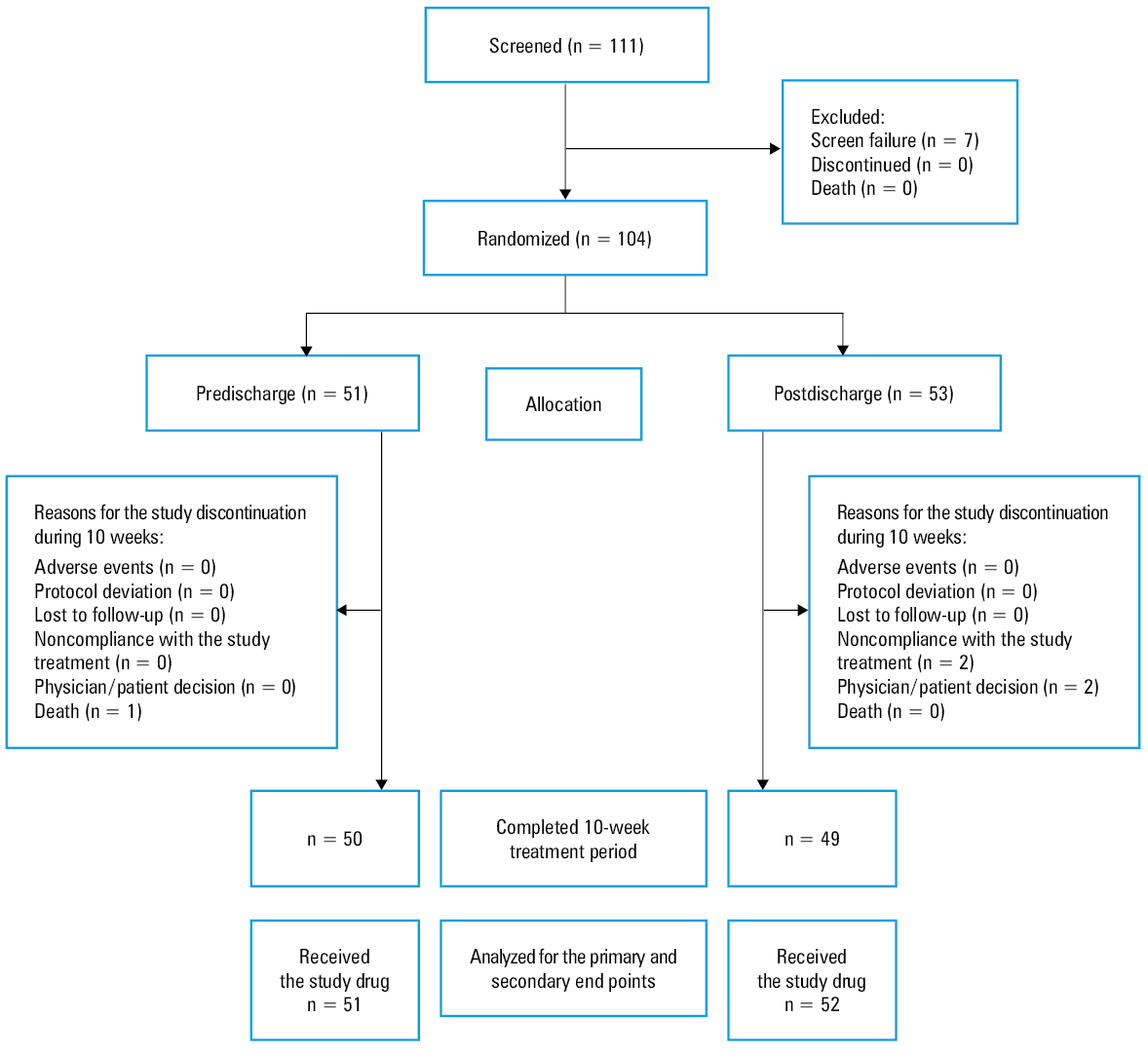
In this post hoc analysis, the subgroup of the Polish patients screened for inclusion in the TRANSITION study included 111 enrolled individuals, of whom 104 were randomized: 51 to the predischarge group and 53 to the postdischarge group (Figure 1).
In the Polish population, the predischarge and postdischarge groups did not differ significantly in terms of clinical characteristics or treatment. Table 1 summarizes the data describing the Polish population and the non‑Polish population, and shows that the groups did not differ in terms of age. However, the Polish subgroup had a higher proportion of men, the patients had significantly higher body mass index, as well as significantly lower heart rate and serum N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) and high‑sensitivity troponin T (hs‑TnT) levels at baseline. The patients in the Polish group were significantly better managed in terms of implanted electrotherapy devices, percutaneous coronary interventions (PCIs), and drug therapy. It should be noted that the Polish patients were significantly more often treated with angiotensin‑converting enzyme inhibitors (ACEIs) before the study enrollment, which resulted from a significantly lower proportion of de novo HF in this subgroup. The study participants in the Polish group had significantly lower New York Heart Association (NYHA) class, and ischemic heart disease was the most common cause of HF. Paradoxically, despite the seemingly less advanced HF among the Polish patients (lower NYHA class, lower NT‑proBNP and hs‑TnT levels), the number of prior hospitalizations was significantly higher in this group. Considering the higher prevalence of coronary artery disease in the Polish population, a significantly more frequent history of myocardial infarction (MI) and PCI was observed.
Parameter | Total (n = 991) | Polish (n = 104) | Non‑Polish (n = 887) | P value | ||
a At screening
b At randomization
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; CABG, coronary artery bypass graft surgery; CRT, cardiac resynchronization therapy; eGFR, estimated glomerular filtration rate; hs‑TnT, high‑sensitivity troponin T; ICD, implantable cardioverter defibrillator; IQR, interquartile range; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; NYHA, New York Heart Association; PCI, percutaneous coronary intervention | ||||||
Age, y, mean (SD) | 66.8 (12) | 65.6 (10.28) | 67 (12.18) | 0.21 | ||
Male sex, n (%) | 744 (75.1) | 86 (82.7) | 658 (74.2) | 0.06 | ||
BMI,a kg/m2, mean (SD) | 29.31 (5.84) | 30.4 (5.61) | 29.18 (5.85) | 0.04 | ||
Systolic blood pressure,a mm Hg, mean (SD) | 124.3 (13.95) | 123.7 (13.66) | 124.3 (13.99) | 0.67 | ||
Diastolic blood pressure,a mm Hg (SD) | 74.4 (10.75) | 76.3 (8.5) | 74.2 (10.96) | 0.02 | ||
Heart rate,a bpm, mean (SD) | 74.4 (12.89) | 70.1 (8.72) | 74.9 (13.21) | <0.001 | ||
Serum creatinine,b μmol/l, mean (SD) | 106.1 (30.02) | 111.6 (29.5) | 105.5 (30.03) | 0.05 | ||
eGFR,b ml/min/1.73 m2, median (IQR) | 59.8 (46.4–75) | 57.3 (45.3–70.3) | 60 (46.7–75.2) | 0.13 | ||
NT‑proBNP,b ng/l, median (IQR) | 1745 (846–3726) | 1120 (482–2636) | 1813.5 (903–3870) | <0.001 | ||
hs‑TnT,b ng/l, median (IQR) | 29 (18–44) | 22 (16–37) | 29 (18–46) | 0.002 | ||
Ejection fraction, %, mean (SD) | 28.79 (7.56) | 28.95 (8.42) | 28.78 (7.46) | 0.83 | ||
Medical history, n (%) | Hypertension | 745 (75.2) | 85 (81.7) | 660 (74.4) | 0.1 | |
Diabetes | 458 (46.2) | 50 (48.1) | 408 (46) | 0.69 | ||
Atrial fibrillation | 477 (48.1) | 54 (51.9) | 423 (47.7) | 0.41 | ||
Myocardial infarction | 339 (34.2) | 45 (43.3) | 294 (33.1) | 0.04 | ||
Stroke | 97 (9.8) | 7 (6.7) | 90 (10.1) | 0.27 | ||
CRT | 88 (8.9) | 15 (14.4) | 73 (8.2) | 0.04 | ||
ICD | 152 (15.3) | 33 (31.7) | 119 (13.4) | <0.001 | ||
Pretrial pharmacotherapy,b n (%) | Any drug | 991 (100) | 104 (100) | 887 (100) | 0.006 | |
ACEIs | 503 (50.8) | 66 (63.5) | 437 (49.3) | |||
ARBs | 247 (24.9) | 25 (24) | 222 (25) | |||
ACEI/ARB‑naïve | 241 (24.3) | 13 (12.5) | 228 (25.7) | |||
De novo heart failure, n (%) | 286 (28.9) | 9 (8.7) | 277 (31.2) | <0.001 | ||
NYHA class,b n (%) | I | 3 (0.3) | 0 | 3 (0.3) | 0.02 | |
II | 635 (64.1) | 81 (77.9) | 554 (62.5) | |||
III | 339 (34.2) | 23 (22.1) | 316 (35.6) | |||
IV | 11 (1.1) | 0 | 11 (1.2) | |||
Ischemic etiology, n (%) | 457 (46.1) | 58 (55.8) | 399 (45) | 0.04 | ||
Prior heart failure hospitalization, n (%) | 485 (48.9) | 67 (64.4) | 418 (47.1) | 0.001 | ||
Heart failure hospitalizations in the last 12 months, n (%) | 0 | 170 (35.1) | 24 (35.8) | 146 (34.9) | 0.93 | |
1 | 197 (40.6) | 25 (37.3) | 172 (41.1) | |||
2 | 73 (15.1) | 11 (16.4) | 62 (14.8) | |||
≥3 | 45 (9.3) | 7 (10.4) | 38 (9.1) | |||
Prior myocardial infarction, n (%) | 339 (34.2) | 45 (43.3) | 294 (33.1) | 0.04 | ||
Prior PCIs, n (%) | 260 (26.2) | 50 (48.1) | 210 (23.7) | <0.001 | ||
Prior CABGs, n (%) | 143 (14.4) | 11 (10.6) | 132 (14.9) | 0.24 | ||
Primary and secondary end points
The primary end point in the Polish subanalysis was reached by 45.1% of patients in the predischarge group and 46.2% of individuals in the postdischarge group, with no significant differences between these groups also with respect to secondary end points (Figure 2).
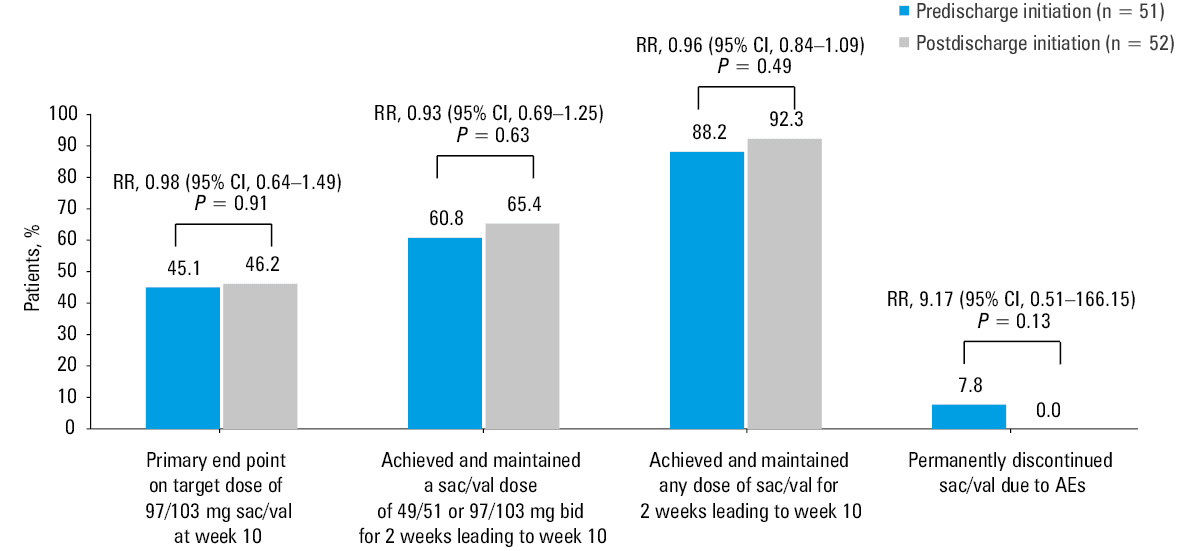
Abbreviations: AE, adverse event; bid, twice daily; RR, relative risk; sac/val, sacubitril / valsartan
The primary end point of achieving the target dose of sacubitril / valsartan at week 10 was achieved by 45.6% of the patients recruited in Poland vs 48.4% of the participants from the non‑Polish population (P = 0.61) (Figure 3). Approximately 90% of the patients received and maintained any sacubitril / valsartan dose for 2 weeks over 10‑week treatment. A total of 53.4% of the Polish population and 48.8% of the non‑Polish population met the secondary end point of achieving and maintaining either 100 mg or 200 mg of sacubitril / valsartan bid for at least 2 weeks up to week 26 after randomization (P = 0.38). There were no significant differences between the Polish and non‑Polish subgroups regarding the other secondary end points.
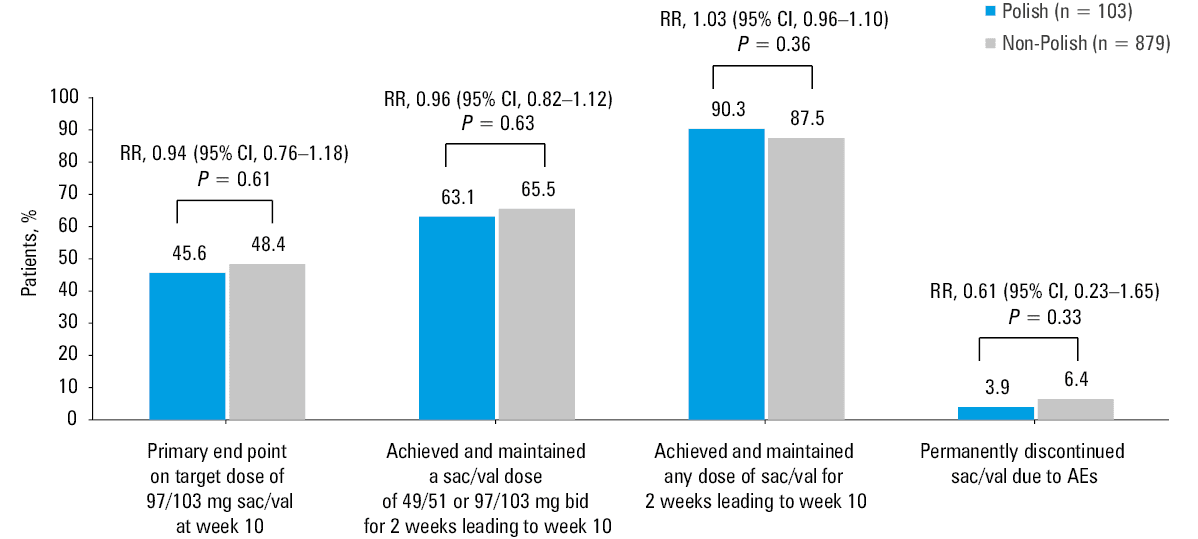
Abbreviations: see Figure 2
Safety
There were no differences in the safety end points between the analyzed groups. The rate of permanent discontinuation of sacubitril / valsartan due to treatment‑related AEs was low in both the Polish (3.9%) and the non‑Polish populations (6.4%) (P = 0.33) (Figure 3). In addition, there were no differences between the predischarge and postdischarge subgroups in the Polish population (Figure 2).
Discussion
This post hoc analysis of the Polish TRANSITION study population compared with the international population from the other 18 countries provides additional information both on the patient characteristics and the efficacy and safety of early sacubitril / valsartan initiation after an acute HF episode. This is one of the few analyses concerning the Polish experience with the use of this modern HFrEF treatment.12-14 Even in the selected population of patients enrolled in the clinical trial, prior HF hospitalizations were significantly more frequent in the Polish population than in the non‑Polish one. The Polish subgroup of the TRANSITION study constituted 10% of all recruited patients. The analyses showed that the Polish population had lower NT‑proBNP and hs‑TnT levels, a greater proportion of NYHA class II patients, and a greater proportion of patients with ischemic etiology, and included significantly more participants with chronic HF previously hospitalized for ADHF. This is a paradox, as although the Polish population seemed to have less advanced HF (lower NT‑proBNP levels, lower NYHA class, lower hs‑TnT levels), they were significantly more likely to be hospitalized before entering the study. A significantly higher percentage of patients treated with ACEIs and those with implantable devices may be due to more frequent hospitalizations as well as a lower proportion of individuals with de novo HF enrolled in the TRANSITION study in Poland, as compared with the international study population. The analysis of the TRANSITION study population revealed a significantly more frequent history of MI (43% vs 33%) and twice higher utilization of PCI (48.1% vs 23.7%) in Poland than in the other countries. The Polish population approximately 2 times more often used the implantable cardioverter‑defibrillator (ICD) (31.7%) than the patients from the other countries (13%), which might reflect a high level of Polish cardiology standard of care and can be partially explained by a significantly higher frequency of prior MI (43% in Poland vs 33% in the other countries). These differences might also be partly related to the selection of 7 highly‑qualified, advanced university hospitals in Poland and may indicate wide availability of interventional cardiology in Poland over the last decades. On the other hand, available publications emphasize the lack of a multidisciplinary model of cardiologic care for patients with HFrEF in Poland as a possible cause of the situation, resulting in hospitalizations remaining the main form of HF care in the country.15 This is consistent with the fact that, for many years, Poland has been a leader in the number of HF hospitalizations among the Organisation for Economic Cooperation and Development countries.16 In the years 2014–2019, the number of hospitalizations for HF exacerbations in Poland increased by 43%, and the associated costs increased by 125% between 2015 and 2020.17,18
The PARADIGM‑HF study19 showed that initiation and use of sacubitril / valsartan in the patients with HFrEF is safe. However, this study involved outpatients in the stable period of chronic HF, and there was still no evidence for the safety of initiating sacubitril / valsartan in the patients hospitalized for ADHF, including those hospitalized with de novo HFrEF.19 Subsequent studies on ARNIs provided new information on the initiation of treatment in a group of patients with newly diagnosed HF.8,9,20 In addition, recent studies show that treatment can be started even in the early phase during hospitalization, as soon as the patient’s clinical condition has been stabilized. In the PIONEER‑HF study, ARNI use, compared with enalapril, was associated with lower incidence of worsening renal function, hyperkalemia, angioedema, or symptomatic hypotension in patients hospitalized for HF decompensation.8 A subgroup analysis of high‑risk patients hospitalized for chronic HF decompensation also demonstrated the safety of ARNI use following stabilization and a reduction in the risk of cardiovascular death and rehospitalization for HF.21 In addition, the patients with more severe decompensation (eg, requiring transient use of pressor amines) experienced AEs with the same frequency as the enalapril‑treated group.21 Furthermore, switching from enalapril to ARNI 8 weeks after an acute HF decompensation event was also beneficial and safe.22 The observed benefit of ARNI was not only due to early initiation but was also associated with the starting dose and patient clinical profile.23 Similarly, in the analysis presented here (7.8% vs 0.0%; P = 0.134) as well as in the study by Wachter et al9 (7.3% vs 4.9%; P = 0.117), there were no significant differences in the rate of permanent sacubitril / valsartan discontinuation due to AEs between the predischarge and postdischarge groups. Serious AEs were observed in 18.4% of the patients and the time of ARNI initiation had no significant effect on their incidence. The PIONEER‑HF study also showed a significant early reduction in NT‑proBNP levels and a significant (39%) reduction in the rehospitalization rate due to worsening of HF in the ARNI group vs the enalapril group.8,21
More than 30% of patients in the PIONEER‑HF study population had newly diagnosed HF. Additional analyses from that study demonstrated that the patients with de novo HF benefited significantly more from ARNI treatment (had a lower risk of rehospitalization and death from cardiovascular causes22 and a greater reduction in NT‑proBNP levels24) than the patients with decompensated chronic HF. In the entire study group, only 50% of the patients had received an ACEI or an angiotensin receptor blocker (ARB) before entering the study.8
Similar analyses were performed for the TRANSITION study data, where 29% of the patients had de novo HF. A more detailed analysis showed that the patients in this group were younger, had lower left ventricular ejection fraction and less severe symptoms of HF, as assessed by the NYHA class. Before index hospitalization, 65% of the patients with de novo HF and 20% of the patients in the group with chronic HFrEF did not receive any ACEI or ARB treatment.20 Initiation of sacubitril / valsartan treatment was associated with an early and progressive reduction in both NT‑proBNP and hs‑TnT levels, with significantly greater decrease in NT‑proBNP values in the de novo HFrEF subgroup than in the patients with decompensated chronic HF. In both groups, similar risk reduction was achieved. The target dose (97/103 mg of sacubitril / valsartan) was achieved by a greater percentage of patients with de novo HFrEF, as compared with those with prior HFrEF diagnosis (56% vs 45%). The safety profile and treatment tolerance were better in the de novo HF group, with a lower percentage of permanent and temporary treatment discontinuation in these participants. In the Polish population, the patients with de novo HF accounted for only 8.7% vs 28.9% in the non‑Polish subgroup. There are no other data from the Polish population available that would indicate what percentage of patients hospitalized for ADHF had de novo HF or how often the treatment with sacubitril / valsartan was introduced in this group of patients during their hospitalization. In view of the PIONEER and TRANSITION study results, according to the new European Society of Cardiology (ESC) guidelines, early initiation of ARNI treatment should be considered in the patients with de novo HF.5
A few papers concerning ARNI use in HFrEF discuss the population of Polish patients in different contexts. A publication by Niemiec et al,14 presenting data on patients with HFrEF based on single‑site follow‑up, showed a significant increase in the proportion of patients treated with sacubitril / valsartan, from 7.8% to 23%, between 2018 and 2020. In contrast to the TRANSITION study population, sacubitril / valsartan treatment was frequently initiated in patients with advanced chronic HF; mean ejection fraction in the study group was 24%, and individuals in NYHA class III/IV represented 64% of the patients.14 Similarly, Lelonek et al12 reported that ARNI treatment was initiated in patients with more advanced HF, with slightly higher baseline NT‑proBNP levels (mean 2600 pg/ml vs 1997 pg/ml), while the ejection fraction was slightly lower (23.6% vs 29%) than in the TRANSITION study.9,20 Also, Kałużna‑Oleksy et al13 found that most patients were in NYHA class III (79%), and the mean NT‑proBNP level was 2900 pg/ml. The TRANSITION study showed that ischemic etiology was a significantly more common cause of HFrEF in the Polish population (56%) than in the non‑Polish subgroup (45%). In a Polish observational study conducted by Lelonek et al,12 this percentage was 42%, and the mean age of 62 years was slightly lower than the average age of the Polish population from the TRANSITION study, whereas in both studies, approximately 82% of the participants were men. Previous HFrEF treatment included ACEIs/ARBs in 98% of the patients, whereas 12.5% of the TRANSITION trial participants were ACEI/ARB‑naive. Implantable devices, such as ICDs, were used in 40% of the population and cardiac resynchronization therapy (CRT) in 17%, which was slightly higher than in the Polish population of the TRANSITION study, most probably due to enrollment of the patients with known stable HFrEF.12
Optimal therapy for the patients with HFrEF also includes implantable devices. A post hoc analysis of the Polish population of the TRANSITION study revealed a relatively higher proportion of patients with an implanted ICD or CRT defibrillator (CRT‑D) before initiation of ARNI therapy, which was also observed in the 2 previously discussed studies conducted in Polish HFrEF patients.12,14 In these studies, sacubitril / valsartan treatment was mostly initiated in the patients with advanced HF. In the current ESC guidelines, sacubitril / valsartan is recommended as the first‑line treatment, which should be included along with other HF‑modifying drugs as soon as during hospitalization, providing new, extended options for the use of this therapy.5 In the study by Lelonek et al,12 over a 1‑year follow‑up, 52% of the patients received the maximum dose of ARNI. Unfortunately, there are no data available on sacubitril / valsartan doses used by Niemiec et al.14 In the TRANSITION trial, more than 45% of the patients in the Polish subgroup and 48% of the patients in the non‑Polish subgroup received the maximum sacubitril / valsartan dose of 97/103 mg bid as early as at treatment week 10. In the Polish population, the proportion of patients who achieved the maximum sacubitril / valsartan doses did not differ between the predischarge and postdischarge subgroups (45% vs 46%; P = 0.91). These data are consistent with those published by Wachter et al,9 in which the percentage of patients achieving maximum sacubitril / valsartan doses was 45% and 50% in the predischarge and postdischarge arms, respectively.9 This confirms that sacubitril / valsartan treatment can be optimized in a considerable proportion of patients in the hospital setting or shortly after discharge, with the aim of achieving maximum doses in line with the current recommendations.
Nowadays, correct drug therapy optimization is a management problem in chronic HF. According to the ESC Heart Failure Long‑Term Registry, in HFrEF patients, RAAS inhibitors were used in 92.2%, whereas β-blockers and mineralocorticoid receptor antagonists (MRAs) were used in 92.7% and 67% of cases, respectively.25 The registry showed that only approximately 30% of the patients received target doses of HFrEF‑modifying drugs, and in more than one‑third the reason for failure to achieve the target doses was not documented.25 Similar conclusions were drawn in from previously published results of the ESC‑HF Pilot.26
The paper by Kolasa et al27 pointed out that during a 3‑month postdischarge follow‑up the optimization of HF therapy was conducted at 16% of primary care physician appointments and at 30% of outpatient cardiologist appointments, even though the recommendations in force between 2016 and 2021 emphasized the need for rapid treatment optimization for patients with HFrEF to improve their prognosis.28 The current recommendations also state the need for rapid, simultaneous optimization of treatment with the 4 drug classes that improve the prognosis for patients with HFrEF.5 The use of HFrEF‑modifying therapy at recommended doses, as compared with lower doses, allows for more effective reduction of the risk of death and HF hospitalization in the patients with HFrEF.29 Recently published data from the United States Change the Management of Patients With Heart Failure (CHAMP‑HF) registry, which included outpatients with HFrEF, also pointed to insufficient implementation of the guidelines issued by the societies of cardiology in clinical practice.29 The registry showed that, at the time of the study initiation, ACEIs/ARBs, β-blockers, MRAs, and ARNIs were used by 66.3%, 80.2%, 33.7%, and 13.6% of patients, respectively.29 Only 11.1% of the patients received the target dose of ACEIs/ARBs, whereas this percentage was 20.3% for β-blockers, 25.4% for MRAs, and only 1.7% for ARNIs.29 Most patients in this registry were on stable but suboptimal doses of HF‑modifying drugs during 1‑year follow‑up, except for ARNIs, the use of which increased by 19.8%, and the number of patients on the target dose increased by 3.4%.29 ARNIs were the group of drugs the least likely to be discontinued by patients in the CHAMP‑HF registry, and the main reason for their discontinuation was nonmedical (patient decision and / or refusal).29 In the patients discharged after HF decompensation, the risk of death is the highest during the first 30 days, and it is twice as high as the risk observed up to 6 months after the discharge.30 Therefore, it is important to initiate / optimize the therapy as soon as during hospitalization before the patient is discharged, as the chances of treatment modification in the outpatient settings are small.
According to the current ESC guidelines, ARNI, with the only representative sacubitril / valsartan, is 1 of the 4 pillars of pharmacotherapy for patients with HFrEF.5 There is a strong evidence for switching from ACEIs to ARNIs in the patients with HFrEF to reduce the risk of death and hospitalization.5,19 However, data from multicenter randomized trials, such as the registries referenced above, indicate the relatively rare use of ARNI in the patients with HFrEF. In the DAPA‑HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) trial, ARNIs were used in 10.7% of the patients (94% received ACEIs/ARBs/ARNIs, 96% a β-blocker, and 71% an MRA).31 In the EMPEROR‑REDUCED study, sacubitril / valsartan was used in 19.5% of the patients.31 The patients receiving ARNI were particularly well‑managed, as evidenced by lower heart rate and NT‑proBNP levels and higher use of implantable devices than in those not receiving sacubitril / valsartan.32 In the DAPA‑HF and EMPEROR‑REDUCED trials, concomitant treatment with ARNI and an SGLT2 inhibitor was well tolerated with significant additional benefits.31,32
Limitations
Some important limitations of the analysis must be acknowledged. First, this is a post hoc analysis of the data from the TRANSTION study. Second, the Polish patients constituted only 10% of the total study population. The small number of patients in the subgroups may not have provided sufficient statistic power to detect actual differences between groups in the clinical parameters examined in the study, including permanent drug discontinuation due to AEs.
Conclusions
In conclusion, our results confirm that sacubitril / valsartan can be used safely in the early period after an episode of acute HF in the Polish and non‑Polish patients with HFrEF, and the likelihood of achieving the maximum dose is the same as for the international population despite significant differences between the Polish and non‑Polish populations. The target dose of sacubitril / valsartan can be achieved in around 50% of cases during the peridischarge period in the patients with HFrEF hospitalized for acute HF. These results may translate into practical decisions about the initiation of sacubitril / valsartan during hospitalization or soon after discharge in a broader spectrum of HFrEF patients.
- Puch‑Walczak A, Bandosz P, Grodzicki T, et al. Prevalence of self‑reported heart failure in the adult Polish population: results of the NATPOL 2011 study. Pol Arch Intern Med. 2022; 132: 16184. | Crossref
- Straburzyńska‑Migaj E, Nessler J, Gackowski A, et al. Heart Failure in Poland ‑ report 2016. Heart Failure Working Group of the Polish Cardiac Society [in Polish]. http://www.niewydolnoscserca.pl/barometr.pdf. Accessed April 14, 2022
- Lippi G, Sanchis‑Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020; 5: 15. | Crossref
- Greene SJ, Fonarow GC, Vaduganathan M, et al. The vulnerable phase after hospitalization for heart failure. Nat Rev Cardiol. 2015; 12: 220‑229. | Crossref
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599‑3726.
ARTICLE INFORMATION