Cancer-associated thrombosis: comparison of characteristics, treatment, and outcomes in oncologic and nononcologic patients followed by a pulmonary embolism response team
Key words: cancer-associated thrombosis, pulmonary embolism, pulmonary embolism response team, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Cancer-associated thrombosis: comparison of characteristics, treatment, and outcomes in oncologic and nononcologic patients followed by a pulmonary embolism response team
Introduction: The risk of venous thromboembolism (VTE) in patients with cancer is currently 12 times higher than in the general population, and even 23 times higher when they receive chemotherapy. The main goal of the pulmonary embolism response team at the Center for the Management of Pulmonary Embolism (PERT‑CELZAT) is to improve prognosis through interdisciplinary care, with a particular focus on patients with contraindications to standard pharmacologic treatment, requiring individual decision‑making, including a wider use of interventional therapeutic methods.
Objectives: The objectives of the study were to report and compare the characteristics and outcomes of pulmonary embolism (PE) in patients with and without cancer treated by the PERT‑CELZAT.
Patients and methods: The analysis included 235 patients diagnosed with VTE who were consulted by local PERT between September 2017 and December 2021. The study group was divided into 2 cohorts: oncologic patients (OP) and nononcologic patients (NOP). There were 81 patients in the OP group (mean [SD] age, 66.2 [14.1] years) and 154 patients in the NOP group (mean age, 57.4 [17.4] years).
Results: The OPs were older and more frequently diagnosed with incidental PE. In‑hospital mortality for all patients reached 6.4% (15/235), 3.7% in the OP and 7.8% in the NOP group (P = 0.27). In‑hospital events, such as major bleeding, minor bleeding, recurrent PE, and deep venous thrombosis occurred with similar frequency in both groups. Posthospital mortality up to 12 months after the PE diagnosis was 12.8% (10/78) in the OP and 4.2% (6/142) in the NOP group (P = 0.03). In a long‑term survival analysis, cancer was associated with increased risk of mortality (hazard ratio, 2.44 [95% CI, 1.51–3.95]; P <0.001) when adjusted for age.
Conclusions: The multidisciplinary therapeutic approach may provide the OPs with VTE an in‑hospital survival rate noninferior to that of the NOPs. The OPs died more often in the following months, because of their underlying neoplastic disease.
What's new?
This study is a retrospective analysis of consecutive patients with venous thromboembolism treated by the pulmonary embolism response team at the Center for the Management of Pulmonary Embolism, which compares the clinical characteristics, outcomes, and mortality of patients with and without cancer. It shows that the patients with cancer can be successfully treated for pulmonary embolism (PE), with their in‑hospital outcomes and mortality rate at the same level as in the patients without cancer. The study postulates that the patients with PE, especially those in the intermediate and high‑risk group or with contraindications for a standard therapy, should be followed by a multidisciplinary team. This may result in lower complication rates and lower in‑hospital mortality. However, a long‑term follow‑up shows that, despite successful treatment in the acute phase of PE, the cancer patients have shorter survival times, which may be associated with the progression of their neoplastic disease.
Introduction
Cancer‑associated thrombosis, manifested as deep venous thrombosis (DVT) and pulmonary embolism (PE), is a common problem experienced by oncologic patients (OPs).1 This population, in addition to cancer, is burdened with other common risk factors for venous thromboembolism (VTE), such as extensive surgery, immobilization, central venous lines, chemotherapy, or targeted anticancer therapy. Recent evidence shows that the risk of VTE in the OPs is currently 12 times higher than in the general population, and even 23 times higher when they receive chemotherapy or targeted therapy.2 The risk of VTE varies according to the type of cancer.3,4 The highest risk is associated with pancreatic cancer, hematological malignancies, lung cancer, gastric cancer, and brain cancer.5
Existing contraindications to thrombolytic and anticoagulant treatment, related to increased risk of bleeding, prevent optimal therapy in the oncologic population. In selected cases, advanced treatment methods, such as catheter‑directed thrombectomy (CDT) or catheter‑directed thrombolysis (CDL) can be applied. In patients with persistent contraindications to anticoagulant treatment or at a high risk of recurrent DVT, it may be necessary to implant an inferior vena cava (IVC) filter. Data from recent randomized controlled trials showed that rivaroxaban, edoxaban, and apixaban may be considered PE treatment options in patients with cancer.6-8
Given the diversity of clinical manifestations of PE and multiple therapeutic interventions available in acute PE,9 implementation of the optimal patient‑tailored treatment is of utmost importance, particularly in special populations such as the OPs. In addition, cancer is a strong independent factor of early death in the patients with PE.10,11 Following the European Society of Cardiology (ESC) recommendation to set up local interdisciplinary pulmonary embolism response teams (PERTs) for PE management,3 the Center for the Management of Pulmonary Embolism (CELZAT) in Warsaw was established in 2017.12 The main goal of CELZAT is to improve patient prognosis by developing a model of interdisciplinary, comprehensive care for patients with PE, with a particular focus on the population of people with contraindications to standard pharmacologic treatment who require individually‑made decisions regarding interventional therapies. Here, we report and compare the characteristics and outcomes of patients with and without cancer consulted by the PERT‑CELZAT.
Patients and methods
Center for the Management of Pulmonary Embolism
CELZAT was created by experts from the Department of Pulmonary Circulation, Thromboembolic Diseases and Cardiology, European Health Center in Otwock, Poland; First Department of Cardiology, Medical University of Warsaw, Poland; and the Department of Cardiac Surgery, Medicover Hospital, Warsaw, Poland.13 The flowchart for activating and operating the system was presented in our previous study.12
Patient enrollment and data collection
The analysis included all patients diagnosed with PE who were consulted by a local PERT between September 2017 and December 2021. All patients included in the study were diagnosed with PE following the current ESC standards.3,14 Information about clinical and treatment data was obtained from their medical records, and included 1) demographic data, 2) symptoms and signs at presentation, 3) risk factors of VTE, 4) comorbidities, 5) oncologic status, cancer stage, and cancer location for OPs, 6) relevant laboratory and imaging findings (levels of cardiac troponins and natriuretic peptides, features of right ventricular [RV] overload on echocardiogram or computed tomography [CT]), 7) VTE location, including the presence of DVT, 8) in‑hospital pharmacotherapy and interventional therapy, 9) the need for endotracheal intubation, extracorporeal membrane oxygenation (ECMO), or admission to an intensive care unit (ICU), 10) in‑hospital outcomes (mortality, stroke, recurrent PE or DVT, and bleeding complications, as defined by the International Society on Thrombosis and Hemostasis [ISTH]), and 11) follow‑up mortality.
Definition of comorbidities
Chronic kidney disease (CKD) was defined based on the presence of either kidney damage (structural or functional abnormalities other than decreased estimated glomerular filtration rate [eGFR]) or decreased kidney function (eGFR <60 ml/min/1.73 m2) for 3 or more months, irrespective of the cause. GFR was calculated using the CKD‑EPI formula. Stroke as a comorbidity at admission referred to both ischemic and hemorrhagic stroke. Obesity was defined as body mass index of 30 kg/m2 or higher. Thrombophilia was defined as a history of hereditary causes, such as factor V Leiden, the prothrombin 20210 mutation, congenital dysfibrinogenemia, hereditary antithrombin deficiency, heterozygous protein C deficiency, heterozygous protein S deficiency, or acquired causes, such as antiphospholipid syndrome or acquired dysfibrinogenemia. Smoking was defined as active smoking or smoking history of at least 5 pack‑years. Reduced mobility was defined as a limitation in the independent, purposeful physical movement of the body or 1 or more extremities. Recent hospitalization was defined as a hospital stay within 1 month prior to the onset of PE. Recent surgery was defined as a surgery within 1 month prior to the onset of PE. Recent trauma was defined as an injury within 1 month prior to the onset of PE.
Assessment of pulmonary embolism severity
The severity of PE was categorized each time into high, intermediate‑high, intermediate‑low, or low risk category, according to the most recent ESC guidelines.3,14 In all patients, the Pulmonary Embolism Severity Index (PESI) and simplified PESI (sPESI) were calculated. High‑risk PE was defined as confirmed acute PE with hemodynamic instability, that is, clinical symptoms of cardiogenic shock or persistent hypotension with systolic blood pressure (BP) below 90 mm Hg or systolic BP drop by at least 40 mm Hg lasting longer than 15 minutes and not caused by new‑onset arrhythmia, hypovolemia, or sepsis. The intermediate‑high risk group included patients who were hemodynamically stable but had features of RV overload (dysfunction on echocardiography or dilation on computed tomography pulmonary angiogram [CTPA]) and increased levels of laboratory markers of myocardial damage (troponin and natriuretic peptides). Elevated troponin was defined as a cardiac troponin I (cTnI) level higher than 0.014 μg/l. Elevated natriuretic peptide was defined as a N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) level above 125 pg/ml. The cutoff values used in our study to stratify patients into appropriate risk groups were those approved by local laboratories. Intermediate‑low risk was defined as the presence of RV overload on echocardiography or CTPA, or an elevated level of troponin, or PESI class III or higher, or sPESI score of at least 1. The low‑risk category involved patients in the PESI class I or II, or with sPESI score of 0.
Central PE was defined as the presence of saddle PE, embolic material located in the main pulmonary artery, lobar arteries, or intracardially, whereas peripheral embolism was diagnosed when segmental or subsegmental arteries were involved.
Treatment and outcomes
Therapeutic interventions in the hospital were recorded for each patient and included anticoagulation alone, systemic thrombolysis, catheter‑directed procedures, and a combination of these therapeutic options. Anticoagulation was defined as the administration of any of the following agents: unfractionated heparin, low‑molecular‑weight heparin (LMWH), vitamin K antagonists (VKAs), or direct oral anticoagulants (DOACs) without any additional therapies. Systemic thrombolysis referred to the intravenous administration of recombinant tissue plasminogen activator (rtPA). Catheter‑directed procedures included CDT and CDL. Another reperfusion method was surgical embolectomy.
Interventional treatment was provided to the patients with cardiogenic shock or significant hemodynamic instability, who either were nonresponsive or had contraindications to standard thrombolytic therapy, and those who were ineligible for pulmonary embolectomy due to logistic reasons (lack of technical possibilities to transport the patient to the embolectomy‑performing center, eg, due to hemodynamic instability). CDT was performed using the Cleaner XTTM Rotational Thrombectomy System (Argon Medical Devices, Athens, Texas, United States), or Indigo CAT8 XTORQ system (Penumbra, Alameda, California, United States), depending on the anatomical conditions and morphology of the clots. For CDL, a Fountain 5F infusion catheter with a 10‑cm long infusion segment (Merit Medical Systems Inc., South Jordan, Utah, United States) was used. The total dose of rtPA did not exceed 10 mg delivered at an infusion rate of 1 mg/h. The rate of CDL, surgical embolectomy, and ECMO was recorded, as well as the number of IVC filters that were placed in the patients with contraindications to standard anticoagulation therapy (eg, recent stroke).
Mortality and complications were assessed during hospitalization, including hemorrhagic stroke, recurrent PE, recurrent DVT, as well as major and clinically relevant nonmajor bleeding. Stroke concerning in‑hospital events referred to hemorrhagic stroke as a complication of anticoagulant therapy, and was defined as stroke caused by bleeding into the brain due to a blood vessel rupture. Recurrent PE was defined as another episode of PE confirmed on CTPA. Recurrent DVT was diagnosed when new thrombi were demonstrated during ultrasound compression tests in either proximal or distal segments of the deep venous system. Bleeding complications were defined according to the ISTH definition. Major bleeding included fatal bleeding and / or symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra‑articular or pericardial, or intramuscular with compartment syndrome, and / or bleeding causing a drop in hemoglobin level of 20 g/l (1.24 mmol/l) or more or leading to a transfusion of 2 or more units of whole blood or red cells. Clinically relevant nonmajor bleeding was described as any sign or symptom of hemorrhage (eg, more bleeding than would be expected for a clinical circumstance, including bleeding found on imaging alone) that did not fit the criteria for the ISTH definition of major bleeding but met at least 1 of the following criteria: requiring medical intervention by a health care professional leading to hospitalization or increased level of care prompting a face to face (ie, not just a telephone or electronic communication) evaluation.15,16
Posthospital mortality up to 12 months after the PE diagnosis was calculated for all the oncologic and nononcologic patients (NOPs). Long‑term survival was calculated from the date of PE diagnosis until the end of the observation. The median (interquartile range [IQR]) follow‑up from PE diagnosis to the end of the observation was 22.5 (14–37) months.
Comparison between the oncologic and nononcologic patients
The OP group included patients during diagnosis (with a suspected or an already confirmed cancerous lesion who have not yet started treatment), patients during therapy (treated with surgery, chemotherapy, radiotherapy, immunotherapy, etc.), and patients in remission (who have completed anticancer treatment). Cancer status was ascribed as of the date of admission to the hospital. NOPs were defined as those without any cancer diagnosis or any history of neoplastic diseases. We compared the groups for baseline clinical characteristics, risk stratification, parameters of PE severity, in‑hospital and postdischarge treatment, follow‑up events, and mortality.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics package, version 27.0 (IBM, Sheffield, United Kingdom). Categorical variables were presented as numbers and percentages. Continuous variables were presented as mean and SD or median with IQR, depending on the distribution. The χ2 test for categorical variables and the Mann–Whitney test for continuous variables were used to determine differences between the groups. For categorical variables with more than 2 categories, the χ2 test was used. No correction for multiple comparisons was performed. Long‑term survival was analyzed using the Kaplan–Meier test and the age‑adjusted Cox proportional hazards regression analysis. A P value below 0.05 was considered significant.
Ethics
Patient consent was waived due to the retrospective nature of the study. The approval of an ethics committee was not required.
Results
Baseline characteristics
PERT‑CELZAT activation occurred 235 times during 52 months of the study. These included 116 activations at the European Health Center in Otwock (49.3%), 104 at the Medical University of Warsaw (44.3%), and 15 at Medicover Hospital (6.4%). Of the entire analyzed population, 34.5% of the patients had active cancer. Characteristics of the patients on admission to the hospital, divided into OPs and NOPs, are presented in Table 1. The OPs were older and were more frequently diagnosed with incidental PE. Symptoms such as dyspnea, cough, pneumonia, and hemoptysis were reported with a similar frequency in both groups. The OPs less frequently reported chest pain and syncope. Both groups had similar comorbidities, but the OPs were less likely than the NOPs to present with obesity. Among other VTE risk factors, the OPs were more likely to have an indwelling catheter and less likely to present reduced mobility and recent trauma.
Parameter | Overall (n = 235) | OP (n = 81) | NOP (n = 154) | P value | |
Data are presented as number (percentage) of patients unless indicated otherwise.
Abbreviations: COPD, chronic obstructive pulmonary disease; DVT, deep venous thrombosis; NOP, nononcologic patients; NYHA, New York Heart Association; OP, oncologic patients; PE, pulmonary embolism; VTE, venous thromboembolism | |||||
Baseline characteristics | |||||
Age, y, mean (SD) | 60.5 (16.8) | 66.2 (14.1) | 57.4 (17.4) | <0.001 | |
Male sex | 126 (53.6) | 39 (48.1) | 87 (56.5) | 0.28 | |
Incidental PE | 13 (5.5) | 10 (12.3) | 3 (1.9) | 0.002 | |
Symptoms on admission | |||||
Dyspnea, NYHA | I–II | 43 (24.7) | 10 (20.8) | 33 (26.2) | 0.69 |
III | 73 (42) | 20 (41.7) | 53 (42.1) | ||
IV | 58 (33.3) | 18 (37.5) | 40 (31.7) | ||
Chest pain | 75 (31.9) | 18 (22.2) | 57 (37) | 0.03 | |
Syncope | 39 (16.6) | 7 (8.6) | 32 (20.8) | 0.02 | |
Cough | 37 (15.7) | 8 (9.9) | 29 (18.8) | 0.09 | |
Pneumonia | 31 (13.2) | 10 (12.3) | 21 (13.6) | 0.84 | |
Hemoptysis | 13 (5.5) | 3 (3.7) | 10 (6.5) | 0.55 | |
Comorbidities | |||||
Active cancer | 81 (34.4) | 81 (100) | 0 | <0.001 | |
Coronary artery disease | 24 (10.2) | 9 (11.1) | 15 (9.7) | 0.82 | |
Congestive heart failure | 22 (9.4) | 7 (8.6) | 15 (9.7) | 0.99 | |
Atrial fibrillation | 16 (6.8) | 8 (9.9) | 8 (5.2) | 0.18 | |
Arterial hypertension | 113 (48.1) | 40 (49.4) | 73 (47.4) | 0.77 | |
COPD | 11 (4.7) | 4 (4.9) | 7 (4.5) | 0.99 | |
Diabetes mellitus | 41 (17.4) | 16 (19.8) | 25 (16.2) | 0.59 | |
Obesity | 64 (27.2) | 14 (17.3) | 50 (32.5) | 0.01 | |
Chronic kidney disease | 17 (7.2) | 4 (4.9) | 13 (8.4) | 0.43 | |
Stroke | 15 (6.4) | 5 (6.2) | 10 (6.5) | 0.99 | |
Depression | 12 (5.1) | 3 (3.7) | 9 (5.8) | 0.55 | |
Thrombophilia | 12 (5.1) | 1 (1.2) | 11 (7.1) | 0.06 | |
Other VTE risk factors | |||||
Smoking | 58 (24.7) | 26 (32.1) | 32 (20.8) | 0.08 | |
Indwelling catheter | 7 (3) | 6 (7.4) | 1 (0.6) | 0.007 | |
Hormonal therapy | 13 (5.5) | 4 (4.9) | 9 (5.8) | 0.99 | |
Reduced mobility | 27 (11.5) | 4 (4.9) | 23 (14.9) | 0.03 | |
Recent hospitalization | 60 (25.5) | 27 (33.3) | 33 (21.4) | 0.07 | |
Recent surgery | 28 (11.9) | 10 (12.3) | 18 (11.7) | 0.99 | |
Recent trauma | 14 (6) | 1 (1.2) | 13 (8.4) | 0.04 | |
Prior PE | 13 (5.5) | 4 (4.9) | 9 (5.8) | 0.99 | |
Prior DVT | 39 (16.6) | 10 (12.3) | 29 (18.8) | 0.27 | |
Prior COVID‑19 | 14 (12.5)a | 2 (4.8) | 12 (17.4) | 0.08 | |
The characteristics of 81 OPs at the time of PE diagnosis are shown in Table 2. The most common tumor stage was metastatic (34.6%), followed by locally advanced cancer (29.6%), and a localized tumor (19.8%). The most frequent cancers were those of the kidney and urinary tract (17.3%), colorectal cancer (16%), and breast cancer (9.9%).
Parameter | OP (n = 81) |
Data are presented as number (percentage) of patients.
Abbreviations: see Table 1 | |
Oncologic status | |
During diagnostics | 18 (22.2) |
During therapy | 45 (55.6) |
In remission | 18 (22.2) |
Cancer stage | |
Localized | 16 (19.8) |
Locally advanced | 24 (29.6) |
Metastatic | 28 (34.6) |
Cancer location / type | |
Kidney and urinary tract | 14 (17.3) |
Colorectal | 13 (16) |
Breast | 8 (9.9) |
Gynecological | 6 (7.4) |
Pancreas | 5 (6.2) |
Stomach | 5 (6.2) |
Lung | 5 (6.2) |
Prostate | 4 (4.9) |
Musculoskeletal system | 3 (3.7) |
Brain | 3 (3.7) |
Hematopoietic system | 3 (3.7) |
Endocrine system | 2 (2.5) |
Melanoma | 2 (2.5) |
Other | 8 (9.9) |
Seventeen patients (21% of the OP group) were transferred from oncologic wards. One patient was referred from an oncology outpatient clinic. Two patients were diagnosed with PE during routine imaging check‑ups performed after oncologic treatment. The remaining OPs were referred from emergency departments.
Characteristics of pulmonary embolism
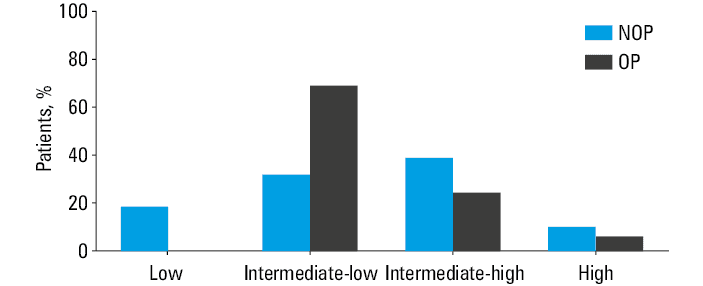
In Table 3 we present the characteristics of PE according to oncologic status of the patients. Figure 1 shows the distribution of early mortality risk groups regarding the oncologic status. Among 81 OPs, the risk was intermediate‑low for 69.1%, intermediate‑high for 24.7%, and high for 6.2% of the patients. Among 154 NOPs, the risk was assessed as low for 18.8%, intermediate‑low for 31.8%, intermediate‑high for 39%, and high for 10.4% of the individuals. The NOPs more commonly (P = 0.03) manifested intermediate‑high risk of early mortality. Bilateral localization, central PE, and saddle PE were more often observed in the NOP group (83.1% vs 66.7%; P = 0.007; 87.6% vs 72.8%; P = 0.007; and 22.7% vs 11.1%; P = 0.04, respectively). The presence of embolic material in the lobar arteries, segmental arteries, and heart cavities was similarly frequently detected in both groups. Among the parameters of PE severity, RV dysfunction on echocardiography was more frequent in the NOPs (52.6% vs 32.1%; P = 0.002). Parameters such as RV dilation on CTPA, cTnI elevation, NT‑proBNP elevation, and the presence of DVT were similar in both groups. PESI class I or II was less common in the OP group (16% vs 60.4%; P <0.001). PESI class III was similarly frequent in both groups, while classes IV and V were more common in the OP group (29.6% vs 9.7%; P <0.001 and 25.9% vs 11%; P = 0.005, respectively). The median PESI score was 108 (IQR, 93–126) in the OP vs 78 (IQR, 63–102) in the NOP group (P <0.001). The mean sPESI score was 1.68 for the OP group and 0.89 for the NOP group (P <0.001). All OPs were in the high‑score sPESI group. Of the NOPs, 44.2% were assigned to the low‑score sPESI group, and 55.8% to the high‑score sPESI group. Intubation and ECMO support were similarly rare in either group, while the OPs less frequently required ICU admission (40.7% vs 72.7%; P <0.001).
Parameter | Overall (n = 235) | OP (n = 81) | NOP (n = 154) | P value |
Data are presented as number (percentage) of patients unless indicated otherwise.
Abbreviations: CTPA, computed tomography pulmonary angiogram; ECHO, echocardiography; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; IQR, interquartile range; PE, pulmonary embolism; PESI, Pulmonary Embolism Severity Index; RV, right ventricle; sPESI, simplified Pulmonary Embolism Severity Index; others, see Table 1 | ||||
PE risk stratification | ||||
Low | 29 (12.3) | 0 | 29 (18.8) | <0.001 |
Intermediate‑low | 105 (44.7) | 56 (69.1) | 49 (31.8) | |
Intermediate‑high | 80 (34) | 20 (24.7) | 60 (39) | |
High | 21 (8.9) | 5 (6.2) | 16 (10.4) | |
PE location | ||||
Bilateral | 182 (77.4) | 54 (66.7) | 128 (83.1) | 0.007 |
Unilateral | 53 (22.6) | 27 (33.3) | 26 (16.9) | |
Central | 194 (82.6) | 59 (72.8) | 135 (87.6) | 0.007 |
Peripheral | 41 (17.4) | 22 (27.2) | 19 (12.3) | |
Saddle | 44 (18.7) | 9 (11.1) | 35 (22.7) | 0.04 |
Main pulmonary artery | 124 (52.8) | 29 (35.8) | 95 (61.7) | <0.001 |
Lobar artery | 176 (74.9) | 54 (66.7) | 122 (79.2) | 0.05 |
Segmental artery | 178 (75.7) | 64 (79) | 114 (74) | 0.43 |
Intracardiac | 9 (3.8) | 1 (1.2) | 8 (5.2) | 0.17 |
Parameters of PE severity | ||||
RV dysfunction (ECHO) | 107 (45.5) | 26 (32.1) | 81 (52.6) | 0.002 |
RV dilation (CTPA) | 51 (21.7) | 18 (22.2) | 33 (21.4) | 0.87 |
↑ Troponin | 131 (55.7) | 40 (49.4) | 92 (59.7) | 0.29 |
↑ Natriuretic peptides | 173 (73.6) | 65 (80.2) | 108 (70.1) | 0.08 |
DVT | 120 (51.1) | 38 (46.9) | 82 (53.2) | 0.45 |
PESI class | ||||
I–II | 106 (45.1) | 13 (16) | 93 (60.4) | <0.001 |
III | 52 (22.1) | 23 (28.4) | 29 (18.8) | |
IV | 39 (16.6) | 24 (29.6) | 15 (9.7) | |
V | 38 (16.2) | 21 (25.9) | 17 (11) | |
Score, points, median (IQR) | 89 (69–114) | 108 (93–126) | 78 (63–102) | <0.001 |
sPESI | ||||
Score, points, median (IQR) | 1 (0–2) | 1 (1–2) | 1 (0–2) | <0.001 |
Low score (0 points) | 68 (28.9) | 0 | 68 (44.2) | <0.001 |
High score (≥1 point) | 167 (71.1) | 81 (100) | 86 (55.8) | |
Clinical severity | ||||
Intubation | 26 (11.1) | 6 (7.4) | 20 (13) | 0.27 |
ECMO support | 15 (6.4) | 3 (3.7) | 12 (7.8) | 0.27 |
ICU admission | 145 (61.7) | 33 (40.7) | 112 (72.7) | <0.001 |
Abbreviations: see Table 1
Treatment
Data on in‑hospital and postdischarge therapy according to the oncologic status are shown in Table 4. Anticoagulation alone was the most common type of therapy, provided with similar frequency to both groups. Other therapies were also applied comparably frequently in the OPs and NOPs. LMWHs (enoxaparin and dalteparin) and DOACs (apixaban, dabigatran, and rivaroxaban) were used in standard therapeutic doses. In the patients with contraindications to full‑dose anticoagulation, IVC filters were implanted and anticoagulant doses were reduced individually. At discharge, the majority of the OPs received LMWH (60.3% vs 21.1%; P <0.001), while the majority of the NOPs received a DOAC (64.8% vs 37.2%; P <0.001). The NOPs were treated with VKAs significantly more often than the OPs (14.1% vs 2.5%; P = 0.008).
Parameter | In‑hospitala | P value | ||
Overall (n = 235) | OP (n = 81) | NOP (n = 154) | ||
Data are presented as number (percentage) of patients.
a The number of patients might exceed 235 due to combined therapies applied to some patients (eg, interventional therapy on top of anticoagulation or systemic thrombolysis).
b The number of patients at discharge is affected by in‑hospital mortality.
Abbreviations: CDL, catheter‑directed thrombolysis; CDT, catheter‑directed thrombectomy; DOAC, direct oral anticoagulants; IVC, inferior vena cava; LMWH, low‑molecular‑weight heparin; VKA, vitamin K antagonists; others, see Table 1 | ||||
Anticoagulation alone | 199 (84.7) | 73 (90.1) | 126 (77.3) | 0.13 |
Systemic thrombolysis | 15 (6.4) | 2 (2.5) | 13 (8.4) | 0.09 |
CDT/CDL | 11 (4.7) | 3 (3.7) | 8 (5.2) | 0.75 |
Surgical embolectomy | 15 (6.4) | 3 (3.7) | 12 (7.8) | 0.27 |
IVC filter | 19 (8.1) | 7 (8.6) | 12 (7.8) | 0.81 |
Parameter | At dischargeb | P value | ||
Overall (n = 220) | OP (n = 78) | NOP (n = 142) | ||
VKA | 22 (10) | 2 (2.5) | 20 (14.1) | <0.001 |
DOAC | 121 (55) | 29 (37.2) | 92 (64.8) | |
LMWH | 77 (35) | 47 (60.3) | 30 (21.1) | |
Outcomes
In‑hospital mortality among all patients reached 6.4%, including 3.7% for the OPs and 7.8% for the NOPs, with the difference not being significant (P = 0.27). Stroke, major bleeding, minor bleeding, recurrent PE, and recurrent DVT occurred with a similar frequency in both groups. Their frequency in the OP group was 1.2% for stroke, 2.5% for major bleeding, and 6.2% for minor bleeding. For the NOPs, the occurrence reached 1.3% for stroke, 3.2% for major bleeding, 4.5% for minor bleeding, 0.6% for recurrent PE, and 0.6% for recurrent DVT. In‑hospital outcomes for the OP and NOP groups are shown in Table 5.
In‑hospital event | Overall (n = 235) | OP (n = 81) | NOP (n = 154) | P value |
Data are presented as number (percentage) of patients.
Abbreviations: see Table 1 | ||||
Death | 15 (6.4) | 3 (3.7) | 12 (7.8) | 0.27 |
Hemorrhagic stroke | 3 (1.3) | 1 (1.2) | 2 (1.3) | 0.99 |
Major bleeding | 7 (3) | 2 (2.5) | 5 (3.2) | 0.99 |
Minor bleeding | 12 (5.1) | 5 (6.2) | 7 (4.5) | 0.76 |
Recurrent PE | 1 (0.4) | 0 | 1 (0.6) | 0.99 |
Recurrent DVT | 1 (0.4) | 0 | 1 (0.6) | 0.99 |
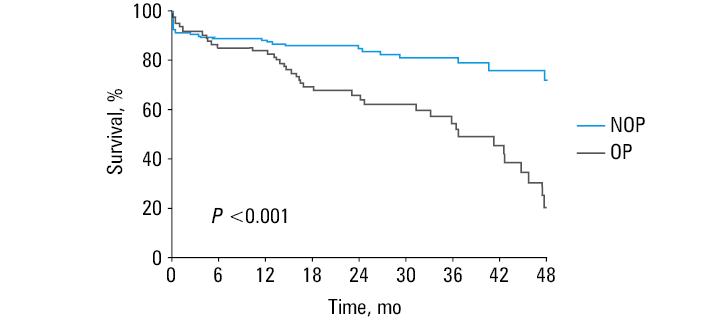
Posthospital mortality up to 12 months after the PE diagnosis was 12.8% (10/78) in the OP and 4.2% (6/142) in the NOP group (P = 0.03). Differences in the long‑term survival between the OP and NOP groups were demonstrated using the Kaplan–Meier curves (Figure 2). In the age‑adjusted analysis, positive oncologic status was associated with increased risk of mortality (hazard ratio, 2.44; 95% CI, 1.51–3.95; P <0.001).
Abbreviations: see Table 1
Discussion
The principles of local PERT‑CELZAT functioning and the characteristics of all patients consulted by the team were previously presented.12,17 Here, we focused on the challenging population of the OPs, who are at a high risk of VTE, which manifested as DVT and PE. The percentage of the OPs treated by our local PERT‑CELZAT was higher than in the other studies describing PERT activity. Almost 34.5% (81/235) of our patients suffered from malignancy, whereas in a meta‑analysis including 22 original studies and 4 surveys this number amounted to 23.5%.18 The co‑occurrence of malignancy and VTE is a sign of poor prognosis and mortality related to recurrent VTE, bleeding, and progress of the neoplastic disease.19 The relationship between malignancy and VTE is already thoroughly described but there is still a great need to broaden our knowledge regarding therapeutic options in VTE as well as assessment of their effectiveness.20
The population of the OPs who have an increased thromboembolic and bleeding risk may particularly benefit from the implementation of PERT. Our novel finding is a similar rate of use of advanced treatment methods in the NOP and OP groups. The use of more intensive treatment methods was not associated with a higher frequency of bleeding complications and did not result in increased in‑hospital mortality. This finding contrasts with the results of a previous paper21 comparing the OP and NOP groups, but performed before the PERT implementation era.
Considering the baseline characteristics of the patients with PE, the main difference between the groups is that the OPs were significantly older. There were also several differences between the groups regarding the most common risk factors for PE. Obesity was a significantly more common risk factor in the NOPs. Approximately 55% to 70% of the OPs develop cancer‑related cachexia; that is why obesity appears to be a rare risk factor for PE in this group of patients.22 Au et al23 obtained similar outcomes, as the OPs they analyzed tended to be older and had lower body mass than the NOPs. Furthermore, Shalaby et al,24 in their retrospective cross‑sectional analysis, also described obesity as a less frequent risk factor in the group of OPs. An often‑appearing risk factor for PE in the group of OPs was an indwelling catheter. The central vein catheter is effectively and commonly used for the administration of chemotherapy, and VTE is a typical complication affecting 5% to 18% of patients after catheterization.25 In the OPs, who generally have an increased risk of VTE, central venous catheter insertion further stimulates thrombus formation and becomes another risk factor for PE. Moreover, reduced mobility and recent trauma were significantly more common risk factors in the NOPs.
It needs to be highlighted that in the OPs, PE was significantly more often incidental, reflecting a higher number of chest CT examinations performed for oncologic indications. In the latest analysis from a large oncologic center, it was also reported that in the patients with malignancy PE is most often incidental.26
Chest pain and syncope were significantly less common in the group of the OPs. Similarly, in the research by Au et al,23 the OPs presented chest pain and syncope less often. Furthermore, Althobaiti et al2 underlined that PE in the OPs has a mildly symptomatic nature.
The unilateral PE was diagnosed significantly more often in the OPs. Also, RV dysfunction on echocardiography was observed significantly less often in the OPs than in the NOPs. Again, our outcomes are similar to what Au et al23 described previously, as bilateral clots and right heart strain were indeed described in their patients less frequently. Moreover, Kim et al21 reported on the OPs who were more likely to develop incidental PE, and less likely to have bilateral embolism or RV dysfunction. Furthermore, the NOPs were more likely to be admitted to the ICU, probably due to the higher prevalence of symptomatic PE in this group.
It should be emphasized that the OPs with PE had higher values of the PESI and sPESI scores. The co‑occurrence of malignancy raised their scores on both scales. In addition, the risk for all OPs was calculated as at least intermediate‑low, because their sPESI score was 1 or higher. It seems important to assess the patients even if they are hemodynamically stable on admission, because they can be at a risk of early complications due to comorbidities such as cancer.27
Several differences in the type of in‑hospital treatment can be observed between the groups. Anticoagulation alone was the most frequently implemented treatment in both groups. There was a significant difference between the groups in the type of treatment at discharge. In the NOP group, DOACs were used most often, while in the OP group, LMWH was the most common therapeutic option. At the same time, only a minority of patients received VKAs as a treatment at discharge in either group. The studied groups also included patients treated for PE before 2019, when the guidelines did not yet state DOACs as a reasonable choice in the OPs. That is why DOACs were rarely used in this group in our study. The selection of anticoagulation therapy for cancer‑related PE is still a subject of discussion and a major challenge for clinicians. The risk of thromboembolic events needs to be balanced with the risk of bleeding events.12,28 For many years, LMWH was used as a standard treatment for cancer‑related PE. LMWH was chosen mainly because of its higher efficacy and similar safety in comparison with VKA.12,29 LMWH remains the best thromboprophylaxis option for hospitalized patients with high risk of VTE incidence.30 The latest trials revealed that DOACs may be more successful in the prevention of recurrent cancer‑related thromboembolism.31,32 On the other hand, we need to acknowledge that they can increase the risk of bleeding, mainly in the patients with gastrointestinal (GI) or genitourinary (GU) cancer. Therefore, the ISTH International Initiative on Thrombosis and Cancer guidelines underline that DOACs can be used as the first‑line treatment for cancer‑associated thrombosis in non‑GI/GU OPs at a low bleeding risk. LMWH is still preferred in the patients with GI/GU cancer‑associated thrombosis. Consequently, the ESC guidelines recommend that edoxaban or rivaroxaban are considered as alternatives to LMWH, with special caution in patients with GI cancer.12,33
Considering the use of advanced PE treatment techniques, such as systemic thrombolysis, surgical embolectomy, or catheter‑directed procedures, the frequency of their usage was at a similar level in both groups. Moreover, the frequency of in‑hospital events also did not differ significantly between the groups. Despite cancer, the OPs can be effectively, and above all safely, offered advanced PE treatment options. Studies also prove that after establishing a PERT the access to advanced therapies is increased, while at the same time the number of bleeding complications does not increase in the OP group.34-36
In both groups, we noticed a similar in‑hospital survival rate. However, significantly higher mortality in the long‑term follow‑up was observed in the OP group, most likely related to their advanced neoplastic disease. Similarly, in the research by Au et al,23 cancer increased 1‑year mortality but did not affect in‑hospital mortality.
What makes our report unique is that other studies regarding local PERT experiences in Poland included a smaller proportion of oncologic cohorts.37,38 For this reason, we believe that our experience can provide a valuable guidance for decision‑making in OPs.
Limitations of the study
There are several limitations of our study that need to be acknowledged. First of all, the study group included 235 patients, so our results should be confirmed in a larger cohort. What is more, the large proportion of patients with low- and intermediate‑low risk in our analysis likely affected the assessment of thrombotic and overall mortality. The PERT focuses mainly on the treatment of patients with intermediate‑high or high risk, so to obtain a more accurate assessment of outcomes (treatment complications and overall mortality), we should include a more diverse group of NOPs in the future. Accordingly, we suggest treating the results reported here as a preliminary analysis. Moreover, the results we presented above are only reports of the activities of a single PERT. Although the PERT was established at highly specialized academic medical centers that have access to interdisciplinary care, local factors might have determined therapeutic choices. Hence, our data should not predict the outcomes of other institutions. Furthermore, our access to a complete medical history of oncologic diseases was sometimes hindered, as the patients were referred to the PERT from other hospitals. Due to the retrospective design of the study, we did not have the information regarding the symptom duration and prior administration of anticoagulation therapy. Also, the lack of data on prescribed medication at the time of consultation by the PERT might have affected the assessment of thrombotic and bleeding‑related outcomes. Moreover, the number of patients with lung cancer in our database is relatively low, which hampers generalization of the results. Additionally, the analysis of outcomes in the patients with PE should take into account that postdischarge death may result from malignancy. Several patients were admitted to the hospital due to PE while they were already at the stage of metastatic cancer. Due to the retrospective nature of the study, we were not always able to determine the specific cause of death. During the 12‑month follow‑up death could occur both due to a PE episode and the underlying oncologic disease. Unfortunately, the available data did not allow us to establish if the specific type of implemented oncologic treatment affected the frequency and severity of PE the patients developed.
Conclusions
As we have proven, the hospital treatment of patients with cancer‑related PE can be effective and safe. With appropriate therapeutic methods, and sometimes advanced PE treatment techniques, the OPs may have the in‑hospital survival rate noninferior to that of the NOPs. Therefore, there is a great need to monitor therapeutic options for cancer‑related PE, evaluate the PERT effectiveness, and analyze the benefits of PERT implementation in this special group of patients.
- Walker AJ, Card TR, West J, et al. Incidence of venous thromboembolism in patients with cancer ‑ a cohort study using linked United Kingdom databases. Eur J Cancer. 2013; 49: 1404‑1413. | Crossref
- Mulder FI, Horvath‑Puho E, van Es N, et al. Venous thromboembolism in cancer patients: a population‑based cohort study. Blood. 2021; 137: 1959‑1969. | Crossref
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020; 41: 543‑603.
- Chew HK, Wun T, Harvey D, et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006; 166: 458‑464. | Crossref
- Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer‑associated venous thrombosis. Blood. 2013; 122: 1712‑1723. | Crossref
ARTICLE INFORMATION