Do circulating concentrations of L-arginine metabolites predict coronary artery disease status and likelihood of cardiovascular events?



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Do circulating concentrations of L-arginine metabolites predict coronary artery disease status and likelihood of cardiovascular events?
Acute myocardial infarction (MI) secondary to coronary heart disease remains one of the leading causes of death.1 Measurement of biochemical parameters in peripheral blood is minimally invasive, and can be technically undemanding as compared with angiography. Ideal biomarkers would be useful in predicting the disease stage and would indicate impending plaque rupture and thus increased likelihood of infarction. Unfortunately, such biomarkers have not yet been identified. In the current edition of Polish Archives of Internal Medicine, Mołek et al2 addressed such issues and reported that, among other clinical measures, thin‑cap fibroatheroma (TCFA) and increased intima‑media thickness are associated with an altered balance of L‑arginine (Arg) metabolites in patients with acute MI and 6 months later. In their earlier study, the authors observed a shifted balance of Arg metabolites in patients with acute MI.3
Arg is one of the most versatile amino acids in the human body.4 Free Arg is a precursor of numerous important biomolecules, such as nitric oxide (NO) and guanidinoacetate (GAA), and a precursor of the energy‑related creatine (Figure 1). Arg residues in proteins undergo several post‑translational modifications, notably guanidine (NG) methylation and citrullination.5 Proteolysis of NG-methylated proteins releases monomethylarginine (LMMA), asymmetric dimethylarginine (ADMA), and symmetric dimethylarginine (SDMA). These methylated Arg metabolites inhibit the activity of constitutive and inducible NO synthase (NOS) isoforms and may also interfere with the cellular Arg transport6 (Figure 1). All NOS isoforms convert Arg to NO and L‑citrulline, albeit with different activity, with inducible NOS (iNOS) being the most active, followed by neuronal NOS (nNOS), and endothelial NOS (eNOS). NO is a gaseous free radical molecule, a neurotransmitter, and one of the most potent endogenous vasodilators and inhibitors of platelet aggregation. Under physiological conditions or in the presence of medicines Arg‑consuming pathways change dynamically, but stay in balance with complex cellular interactions. Valid analytical methods are required to determine deviations of “normal” values and intervals of certain metabolites in the blood, which may then be used in diagnosis and therapy. Determination of several parameters enables a more complex assessment of the imbalance caused by a disease or by other circumstances, such as pharmacological interventions.7 Yet, there are many difficulties and limitations in this context.
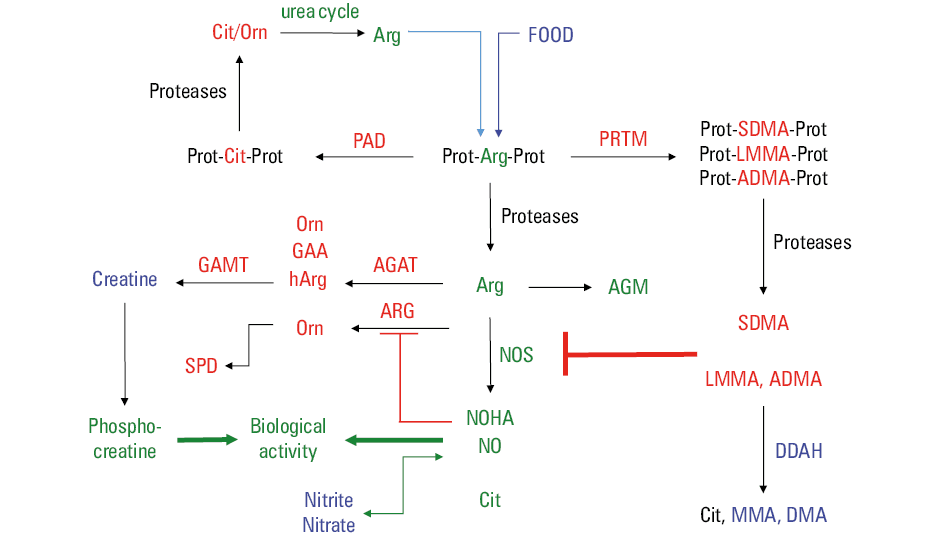
Abbreviations: hARg, L‑homoarginine
The global arginine bioavailability ratio (GABR) is a widely used composite measure in clinical studies investigating the pathways that involve Arg. GABR is a dimensionless ratio of the concentration of Arg and total concentration of its major metabolites, that is, citrulline (Cit) and ornithine (Orn) in the circulation: GABR = [Arg]/([Cit]+[Orn]). The GABR value of 1, which is equivalent to 100%, can be observed for low, normal, and high concentrations of Arg, Cit, and Orn, indicating in all the cases a balanced Arg pathway, yet at different levels of concentration. Temporary (over 4 h), drastic changes in GABR values (from 1 to 0.02) were observed in patients after orthotopic liver transplantation (OLT),8 likely due to a release of huge amounts of arginase from the liver graft.9 Nevertheless, despite the almost complete removal of Arg from the patients’ blood, no decrease in this time window was observed in the plasma and urine concentration of ADMA and its major metabolite dimethyl amine (DMA), or of nitrate and nitrite,8 the major NO metabolites and measures of its synthesis. This finding indicates a limited usefulness of GABR as a measure of the balance of the Arg pathway. GABR values without presentation of the corresponding discrete concentrations of Arg, Cit, Orn, and especially of nitrite and nitrate are of little usefulness. The absolute concentrations of Arg and other amino acids are of particular interest, as they affect the activity of enzymes and transporters, especially those associated with Arg. Thus, LMMA, ADMA, and SDMA inhibit the activity of NOS (Figure 1), and, to a lesser extent, the activity of Arg transporters due to their comparably lower concentrations.6 This also applies to homoarginine (hArg) which is produced from Arg and is a low‑affinity NOS substrate. At higher concentrations, hArg may compete with Arg for NOS and even decrease NOS‑catalyzed formation of NO.
Circulating nitrite and nitrate are metabolites of NO produced from Arg by the catalytical action of at least 3 NOS isoforms. eNOS, nNOS, and iNOS show different activity and are also differently inhibited by LMMA, ADMA, and SDMA.6 Thus, the concentrations of nitrite and nitrate in the plasma or serum are not dependable indicators and measures of a particular NOS isoform, but they reflect the contribution of all 3 NOS isoforms. Distinction between NOS isoforms would require invasive procedures to analyze their expression in cardiomyocytes. Not only for these reasons, it is difficult to assume that the presence of TCFA in the culprit lesion can be actually predicted based on the concentration of any Arg metabolite in the peripheral blood.
The concentration ratio of Cit to Orn (C/O), is often used as a measure of the relationship of NOS (Arg conversion to Cit) and arginase (Arg conversion to Orn). However, this is an extreme simplification, because it does not consider large contribution of other pathways yielding Cit and Orn. Dimethylarginine dimethylaminohydrolase (DDAH) hydrolyzes ADMA to Cit and DMA (Figure 1). The role of Arg citrullination and DDAH activity in the production of Cit is considerably greater than that of NOS activity. This also applies to the activity of a 2‑substrate enzyme arginine:glycine amidinotransferase (AGAT). AGAT catalyzes the reaction of Arg with glycine (Gly) that yields Orn and guanidino acetate (GAA), a precursor of creatine.7 The concentration ratio of Orn to Arg (O/A), and the concentration ratio of Arg to ADMA, (Arg/ADMA), have also been used by Mołek et al.2 The Arg/ADMA ratio is often used to determine the “capacity” of a system to produce NO from the NOS‑substrate Arg and the NOS‑inhibitor ADMA.10 The Arg/ADMA ratio is subject to great variations. To the best of our knowledge, no values or intervals have been recommended so far for GABR, C/O, O/A, or the Arg/ADMA ratios in experimental or clinical studies.
A major question that arises in this area is whether concentration changes seen in the circulation for the metabolites of Arg pathways, which are ubiquitous, are specific to a particular organ, tissue, or artery segment. It seems that this is realistic in acute rather than chronic conditions, as observed for arginase in OLT.8,9 But are altered Arg metabolites predictors of acute and chronic coronary heart disease and outcome? Mołek et al2 suggested that the cause of altered Arg metabolites may be locally increased arginase activity in ischemic and reperfused myocardium that results in impaired NO synthesis due to low Arg concentrations. However, a causal link with TCFA appears inconclusive. The authors referred to cell culture and animal studies, where increased arginase activity was observed in smooth muscle cells, the vessel wall, and in atherosclerotic plaques. However, arginase is highly expressed in the liver, small intestine, as well as in circulating monocytes, and alveolar macrophages. MI may evoke acute effects in these organs and cells, including changes in their arginase activity.11 Common comorbidities in MI patients, such as diabetes,12,13 and medications, such as ticagrelor14 and heparin15 may also alter Arg metabolism in different mechanisms including alteration of arginase activity. Further, contribution of nutrition, a major external source of Arg, nitrite, nitrate, and DMA, is a limiting factor. Finally, TCFAs were analyzed in the culprit lesions only, while patients may have suffered from multi‑vessel coronary disease or peripheral atherosclerotic disease, where the conditions of these vessels are unknown.
We noted in the papers by Mołek et al2,3 very low circulating concentrations of Arg, Cit, Orn, and proline, and very high circulating concentrations of agmatine (AGM) and spermidine (SPD). The reported AGM and SPD concentrations were even higher than those of their precursors. In addition, extreme values of Arg metabolites were omitted in some statistical analyses of the study,2 yet the reader is not aware of the origin and reasons for these deviations. Large deviations in analyte concentrations are likely to be due to analytical shortcomings, even when using highly sophisticated techniques such as liquid‑chromatography tandem mass spectrometry, and they may weaken the outcome of the study. The use of validated, precise, and accurate analytical chemistry methods for the measurement of concentrations of Arg metabolites in plasma or serum is an indispensable requirement.
Special attention needs to be paid when analyzing associations of biochemical measures, such as Arg and its metabolites, with specific functional clinical measures, such as TCFA. The statistical methods to be used in such clinical studies need to be clearly defined. They should include acceptance and rejection criteria for relevant parameters, including the extent of association of potentially new biomarkers with established specific biomarkers. The extent of minimum values for receiver operating characteristic (ROC), odds and hazard ratios also need definition alongside the acceptance and rejection criteria. In our opinion, ROC values of about 0.8 for GABR, O/A, and the other parameters are too low for serving as predictors of ischemia, even if analyses indicate statistical significance.
- Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. Lancet. 2017; 389: 197‑210. | Crossref
- Mołek P, Żmudzki P, Machnik A, et al. Thin‑cap fibroatheroma and increased coronary intima‑media thickness are associated with an altered arginine metabolites balance. Pol Arch Intern Med. 2023; 133: 16356. | Crossref
- Molek P, Zmudzki P, Wlodarczyk A, et al. The shifted balance of arginine metabolites in acute myocardial infarction patients and its clinical relevance. Sci Rep. 2021; 11: 83. | Crossref
- Wu G, Morris SM Jr. Arginine metabolism: nitric oxide and beyond. Biochem J. 1998; 336: 1‑17. | Crossref
- Tsikas D. Post‑translational modifications (PTM): analytical approaches, signaling, physiology and pathophysiology‑part I. Amino Acids. 2021; 53: 485‑487. | Crossref
ARTICLE INFORMATION