Granulomatosis with polyangiitis: a rare case of a critical lesion encompassing the conduction system and the heart valve



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Granulomatosis with polyangiitis: a rare case of a critical lesion encompassing the conduction system and the heart valve
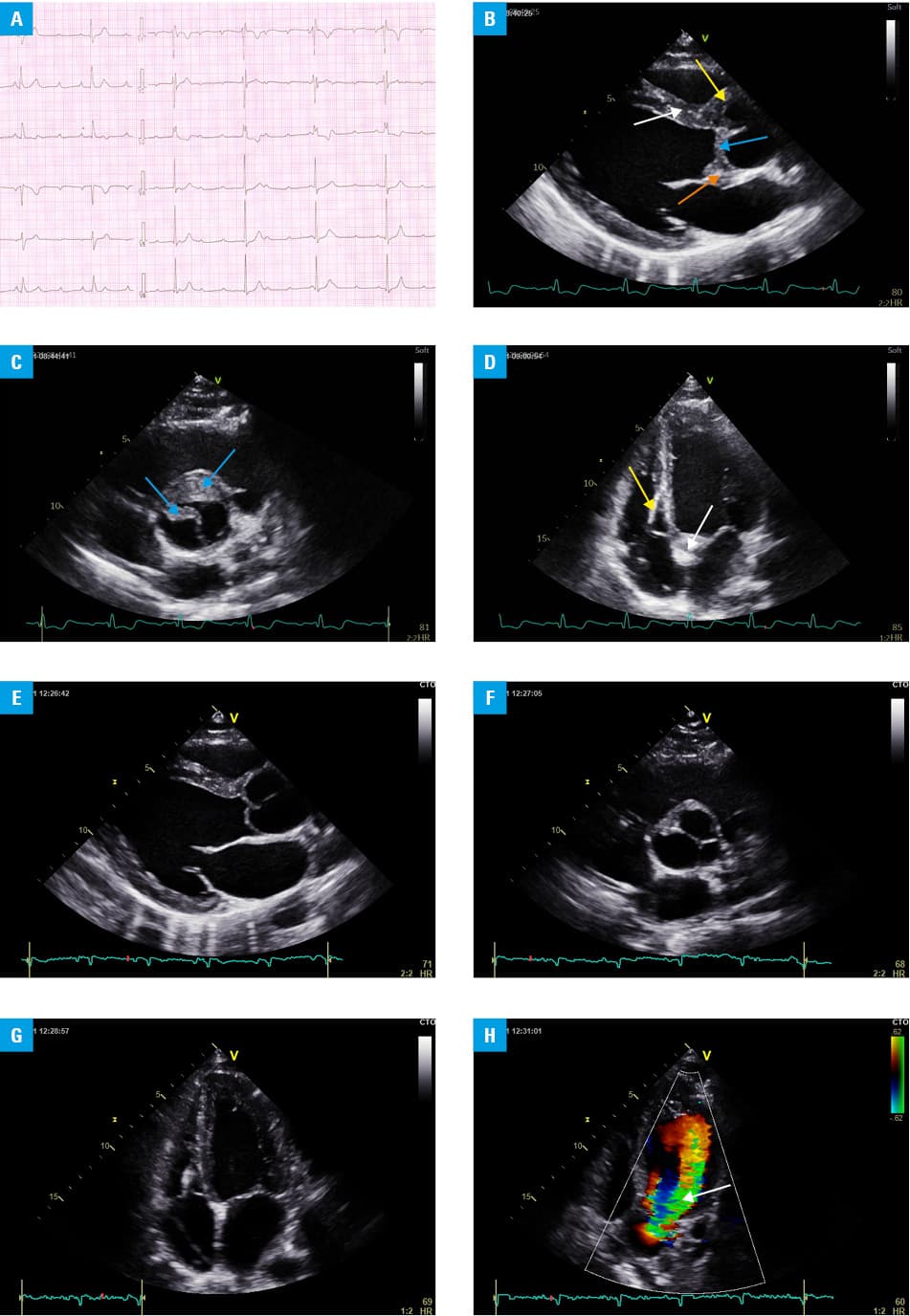
A 26‑year‑old man was urgently admitted to our cardiology department due to cardiogenic shock in the course of a third‑degree atrioventricular block (Figure 1A), with ventricular rate of 20–25 bpm. Initially, temporary pacing was used. In the following days, due to the persistence of a complete block, a dual‑chamber pacemaker was implanted.
Laboratory tests revealed negative blood cultures, C‑reactive protein at 20.1 mg/l (reference range [RR], <6.0 mg/l), procalcitonin 0.05 ng/ml (RR, <0.50 ng/ml), white blood cell count 10.6 G/l (RR, 3.5–10 G/l), hemoglobin 15.2 g/dl (RR, 12–17 g/dl), platelet count 365 G/l (RR, 125–400 G/l), creatinine 0.9 mg/dl (RR, 0.7–1.2 mg/dl), potassium 4.5 mmol/l (RR, 3.5–5.1 mmol/l), troponin T 37.4 pg/ml (RR, <13 pg/ml), creatine kinase muscle brain 11.5 U/l (RR, <25.0 U/l), thyroid stimulating hormone 1.15 µU/ml (RR, 0.27–4.20 µU/ml), and normal urinalysis.
The patient had a history of granulomatosis with polyangiitis (GPA) involving the upper and lower airways and left craniofacial area, and transient hematuria, diagnosed 5 years earlier. Echocardiography performed at that time was normal. The patient underwent surgery on the left maxillary sinus, was treated with cyclophosphamide, azathioprine, and mycophenolate mofetil, and had been in remission for several years.
The current echocardiographic examination (transthoracic and transesophageal echocardiography) revealed infiltration / thickening of the proximal segment of the interventricular septum, extending to the initial segment of the aortic root, mitro‑aortic curtain, and aortic valve, with slight impairment of the valve mobility and aortic regurgitation (Figure 1B–D). The left ventricular end‑diastolic diameter (LVEDD) was slightly enlarged (60 mm), with preserved ejection fraction (EF). Other heart valves and the pericardium showed no abnormalities.
Due to the suspicion of GPA recurrence, the patient was referred to a rheumatology department. Computed tomography revealed thickening of the left maxillary sinus mucosa and several pneumatoceles in both lungs, while serology revealed the presence of perinuclear anti‑neutrophil cytoplasmic antibodies, confirming GPA flare. High‑dose steroid therapy was implemented, with gradual normalization of the inflammatory parameters.
Two weeks later, control echocardiogram (Figure 1E–G) showed regression of the infiltrative changes in the aortic root and aortic valve. However, prolapse of the previously infiltrated leaflet and quite severe valve regurgitation were found, with progression of the left ventricular volume overload (LVEDD 64 mm) at preserved ejection fraction (EF 55%).
The patient was started on mycophenolate mofetil and rituximab. Follow‑up clinical evaluation and laboratory tests revealed no signs of the disease activity but subsequent echocardiograms showed persistent severe aortic regurgitation (Figure 1H). A few months later, the patient underwent surgical replacement of the aortic valve together with the ascending aorta with the Bentall‑de Bono method, when a conduit containing a mechanical valve was implanted. A small sequential pacing load was recorded in the pacemaker control.
Heart involvement in GPA is not as rare as previously thought and, according to various authors, ranges from several to several dozen percent.1 Early reports described mainly involvement of the pericardium, coronary arteries, and myocardium, and the most frequent electrocardiographic manifestation were supraventricular arrhythmias.1 In later reports using echocardiographic assessment, involvement of the heart valves was much more often described, especially the aortic valve regurgitation.2
Total atrioventricular block is one of the rarest cardiac complications of GPA.3,4 Damage to the aortic valve with its regurgitation and coexisting third‑degree atrioventricular block is undoubtedly even rarer.5 Echocardiography should be an integral part of the disease activity assessment in GPA patients.
- Fauci AS, Haynes BF, Katz P, Wolff SM. Wegener’s granulomatosis: prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med. 1983; 98: 76‑85. | Crossref
- Życińska K, Borowiec A, Zielonka TM, et al. Echocardiographic assessment in patients with granulomatosis with polyangiitis. Adv Exp Med Biol. 2017; 1022: 27‑33. | Crossref
- Santos LPS, Bomfim VG, Bezerra CF, et al. Heart conduction system defects and sustained ventricular tachycardia complications in a patient with granulomatosis with polyangiitis. A case report and literature review. Rev Bras Ter Intensiva. 2017; 29: 386‑390. | Crossref
- Valente F, Rozen L, Carlier S, Godart P. An uncommon case of complete AV block. BMC Cardiovasc Disord. 2022; 22: 429. | Crossref
- Ruisi M, Ruisi P, Finkielstein D. Cardiac manifestations of Wegener’s granulomatosis: case report and review of the literature. J Cardiol Cases. 2010; 2: e99‑e102. | Crossref
ARTICLE INFORMATION