Short- and long-term survival of patients hospitalized for COVID-19 in relation to cardiovascular risk factors and established cardiovascular disease: the Cor-Cardio study
Key words: cardiovascular disease, cardiovascular drugs, cardiovascular risk factors, COVID-19, hypertension



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Short- and long-term survival of patients hospitalized for COVID-19 in relation to cardiovascular risk factors and established cardiovascular disease: the Cor-Cardio study
Introduction: The clinical presentation of COVID‑19 may range from asymptomatic infection to severe disease. Previous studies reported a relationship between the course of COVID‑19 and a history of cardiovascular (CV) disease (CVD).
Objectives: We aimed to analyze the influence of CV risk factors, established CVD, and treatment with CV drugs on short- and long‑term survival in patients hospitalized for COVID‑19.
Patients and methods: We retrospectively analyzed data of patients hospitalized in 13 COVID‑19 hospitals in Poland (between March and October 2020). Individual deaths during the follow‑up were recorded until March 2021.
Results: Overall, 2346 patients with COVID‑19 were included (mean age, 61 years; 50.2% women). A total of 341 patients (14.5%) died during the hospitalization, and 95 (4.7%) died during the follow‑up. Independent predictors of in‑hospital death were older age, a history of established CVD, heart failure, and chronic kidney disease (CKD), while treatment with renin‑angiotensin‑aldosterone system blockers or statins was associated with a lower risk of death during hospitalization. Factors that independently predicted death during the follow‑up were older age, a history of established CVD, CKD, and a history of cancer. The presence of CV risk factors did not increase the odds of death either in the hospital or during the follow‑up. Of note, higher systolic blood pressure and oxygen blood saturation on admission were associated with better short- and long‑term prognosis.
Conclusions: Established CVD and CKD were the main predictors of mortality during both the hospitalization and the follow‑up in the patients hospitalized for COVID‑19, while the use of CV drugs during the hospitalization was associated with better prognosis. The presence of CV risk factors did not increase the odds of in‑hospital and postdischarge death.
What's new?
The influence of various factors on the course of COVID‑19 has been widely analyzed. In the present study, we assessed the impact of cardiovascular risk factors and established cardiovascular disease not only on in‑hospital but also on long‑term mortality during a follow‑up of at least 5 months. Of interest, cardiovascular risk factors were not linked to the risk of death either in the hospital or during the follow‑up, while established cardiovascular disease significantly increased the mortality risk during both the hospitalization and the follow‑up.
Introduction
The clinical spectrum of SARS‑CoV‑2 infection ranges from asymptomatic infection to life‑threatening, fatal disease with persistent severe symptoms and even marked organ dysfunction, including cardiorenal damage.1,2 The degree of cardiac involvement in COVID‑19 is variable and ranges from mildly elevated levels of cardiac biomarkers to acute cardiogenic shock and sudden cardiac death.3-5
There are reports in the literature of a relationship between the course of acute respiratory disease syndrome caused by SARS‑CoV‑2 and a history of hypertension and cardiovascular (CV) disease (CVD).6-10 The results of studies on the relationship of CV risk factors, established CVD, and the use of CV drugs with the course of COVID‑19 are inconsistent.6,10-13
In the first year of the pandemic, comorbidities such as hypertension, diabetes mellitus, and hypercholesterolemia were identified as risk factors for poor outcome in COVID‑19.6-8,10,12 Similarly, for unconfirmed reasons, the prognosis of patients with COVID‑19 was speculated to be negatively affected by the use of angiotensin‑converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs).14 In subsequent studies, based mainly on retrospective analyses, the prognostic value of hypertension turned out to be insignificant,11,15 and it was also stated that the use of ACEIs/ARBs did not worsen the prognosis of patients with COVID‑19.11,16-18 Considering most of the established risk factors for CVD, it was observed that the coexistence of COVID‑19 with established CVD worsens the prognosis.7,10,12 However, a question arises whether the CV risk factors are indeed independent predictors of mortality in COVID‑19 patients without established CVD.
As the number of patients with COVID‑19 constantly increases, the assessment of short- and long‑term prognosis of these patients in relation to the CV risk factors, presence of CVD, and its treatment represents an important aspect in terms of clinical management of COVID‑19.7,12 This multicenter Cor‑Cardio study undertaken by the National Institute of Cardiology in Warsaw and the University Hospital in Kraków aimed to assess the influence of CV risk factors, established CVD, and the use of CV drugs on short- and long‑term survival of patients hospitalized for COVID‑19.
Patients and methods
Data of consecutive patients with COVID‑19 treated in 13 COVID‑19 hospitals in Poland were analyzed in the study. In all centers, data on prehospital diagnoses and medications, clinical status on admission, clinical course, complications, and duration of the hospitalization were collected. Hospitalizations took place between March 6, 2020 and October 15, 2020. The status of the patients (alive or deceased) was established as of March 26, 2021 based on data from the National Electronic Population Registration System in Poland.
The Cor‑Cardio study was registered at ClinicalTrials.gov (NCT04374110), and received the approval of the Ethics Committee at the National Institute of Cardiology (1860).
COVID‑19 was diagnosed according to the World Health Organization and Polish guidelines with the use of the reverse transcription–polymerase chain reaction test.19,20 The patients were treated in accordance with the recommendations of the Polish Association of Epidemiologists and Infectiologists.19,20 We defined the CV risk factors as follows: 1) type 2 diabetes mellitus: a history of diabetes or current use of hypoglycemic drugs, 2) hypertension: a history of hypertension or current use of antihypertensive drugs, and 3) hypercholesterolemia: a history of hypercholesterolemia or current use of lipid‑lowering drugs. Established CVD included a history of 1) coronary artery disease: a history of myocardial infarction, coronary revascularization, or a diagnosis of chronic coronary syndrome, and 2) cerebrovascular disease: a history of stroke or transient ischemic attack. Both CV risk factors and established CVD were identified based on the medical history of prehospital diagnosis and / or treatment, and were defined according to the current guidelines of the European Society of Cardiology.21
Other evaluated diseases were defined as follows: 1) heart failure (HF): previous HF diagnosis, 2) atrial fibrillation (AF): a history of AF or AF on admission, 3) chronic kidney disease (CKD): previous CKD diagnosis or prehospital estimated glomerular filtration rate (eGFR) value below 60 ml/min/1.73 m2, 4) chronic obstructive pulmonary disease (COPD) or asthma: a history of COPD or asthma, and 5) cancer: a history of or current cancer. We also analyzed the use of selected CV drugs that had previously been associated with a prognosis in COVID‑19, including β-blockers, ACEIs/ARBs, statins, mineralocorticoid receptor antagonists (MRAs), and acetylsalicylic acid (ASA).
The analyzed end points according to the protocol of our study were in‑hospital all‑cause mortality and out‑of‑hospital mortality in the patients surviving the hospitalization. We also assessed the need for mechanical ventilation and length of hospital stay.
Statistical analysis
Database management and statistical analyses were performed with the PASW Statistics 18 software (formerly SPSS Inc., Chciago, Illinois, United States) and SAS software, version 9.4 (SAS Institute, Cary, North Carolina, United States). The results are expressed as percentages for categorical variables and mean with SD or median with interquartile range (IQR) for continuous variables, depending on the normality of their distribution (assessed by the Shapiro–Wilk test).
To analyze the differences between the studied groups (survivors vs nonsurvivors and in‑hospital death vs death during the follow‑up), we applied the 1‑way analysis of variance (ANOVA) for the normally distributed and the Kruskal–Wallis test for the non‑normally distributed continuous variables. Categorical variables were compared by the χ2 test in the FREQ Procedure. All post hoc analyses were performed using the Bonferroni adjustments.
Finally, in the logistic regression analyses, independent predictors of in‑hospital death or death during the follow‑up were explored. Differences were considered significant at P below 0.05.
Results
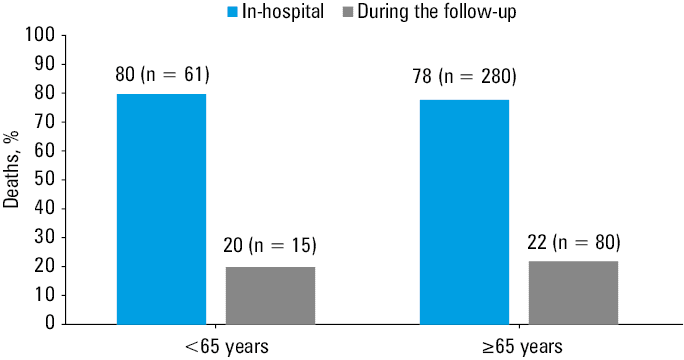
We evaluated 2346 patients hospitalized for COVID‑19 between March and October 2020. The mean (SD) age of the patients was 61 (17) years, and 50.2% of them were women. The median (IQR) duration of hospitalization was 16 (10–24) days. During the hospitalization, a total of 341 patients died (14.5%). The median (IQR) follow‑up of the patients who survived the hospitalization was 213 (172–293) days. During this period, 95 patients died, which represented 4.7% of the 2005 patients discharged from the hospital. The vast majority of in‑hospital and follow‑up deaths occurred among the patients over 65 years of age. Among the 95 patients who died during the follow‑up, only 15 were younger than 65 years (Figure 1).
In the group of patients who survived the hospitalization or were alive at the end of the follow‑up we observed a lower prevalence of established CVD, HF, CKD, and history of cancer than in the nonsurvivors (Table 1). The patients who survived were also younger than those who died during the hospitalization or the follow‑up. The number of individuals with CV risk factors but without established CVD was higher among the survivors than in those who died during the hospitalization. The patients who died during the hospitalization shared a similar prevalence of CV risk factors, established CVD, and other concomitant diseases to those who died during the follow‑up (Table 1). Regarding the clinical condition on admission, the patients who died in the hospital, as compared with those who survived the hospitalization, were characterized by lower blood pressure, higher heart rate and plasma glucose concentration, as well as by lower oxygen saturation. They also more often required mechanical ventilation (Table 1). The patients who died during the follow‑up were hospitalized for a longer time and more frequently required mechanical ventilation than those who were alive at the end of the follow‑up (Table 1).
Variable | All patients (n = 2346) | Group 1: alive (n = 1910) | Group 2: in‑hospital death (n = 341) | Group 3: death during the follow‑up (n = 95) | P value (ANOVA) | 1 vs 2 | 1 vs 3 | 2 vs 3 |
Data are presented as mean (SD), median (IQR), or percentage.
a Data available in 935 patients for BMI, 2028 patients for SBP, 2024 patients for DBP, 1975 patients for HR, 1987 patients for SpO2, 1881 patients for glucose, 2345 patients for CKD, 2345 patients for COPD, 2345 patients for asthma, and 344 patients for a history of cancer
Abbreviations: AF, atrial fibrillation; ANOVA, analysis of variance; BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; CVD, cardiovascular disease; DBP, diastolic blood pressure; DM, diabetes mellitus; HCH, hypercholesterolemia; HF, heart failure; HR, heart rate; HT, hypertension; SBP, systolic blood pressure | ||||||||
Male sex, % | 49.8 | 49.1 | 54.3 | 48.4 | 0.21 | 0.08 | 0.9 | 0.31 |
Age, y | 61.1 (17.4) | 57.8 (16.7) | 75.6 (12.5) | 75 (11.9) | <0.001 | <0.001 | <0.001 | 0.96 |
Duration of hospitalization, d | 16 (10–24) | 16 (11–24) | 10 (5–18) | 29 (15–43) | <0.001 | <0.001 | <0.001 | <0.001 |
BMIa, kg/m2 | 28.4 (5.1) | 28.5 (4.9) | 28 (5.8) | 26.2 (5.5) | 0.16 | 0.91 | 0.28 | 0.61 |
SBPa, mm Hg | 133 (21) | 134 (20) | 126 (26) | 131 (23) | <0.001 | <0.001 | 0.75 | 0.18 |
DBPa, mm Hg | 82 (13) | 83 (12) | 75 (17) | 80 (15) | <0.001 | <0.001 | 0.17 | 0.01 |
HRa, bpm | 85 (15) | 84 (14) | 87 (19) | 82 (16) | <0.001 | <0.001 | 0.46 | <0.001 |
SpO2a, % | 96 (93–97) | 96 (94–97) | 93 (87–96) | 95 (92–97) | <0.001 | <0.001 | <0.001 | 0.001 |
Glucosea, mmol/l | 5 .77 (5.03–7.11) | 5.68 (5.02–6.88) | 6.89 (5.34–9.34) | 5.5 (4.82–7.44) | <0.001 | <0.001 | 0.94 | 0.001 |
Mechanical ventilation, % | 9 | 3.5 | 40.2 | 9.5 | <0.001 | <0.001 | 0.003 | <0.001 |
HT, % | 56.6 | 53.5 | 71.8 | 64.2 | <0.001 | <0.001 | 0.04 | 0.15 |
DM, % | 24.4 | 21.3 | 36.4 | 44.2 | <0.001 | <0.001 | <0.001 | 0.16 |
HCH, % | 20.2 | 19.6 | 21.7 | 25.3 | 0.13 | 0.37 | 0.18 | 0.46 |
Presence of CV risk factors, % | 32.6 | 34.1 | 25.8 | 25.3 | 0.003 | 0.002 | 0.07 | 0.91 |
CAD, % | 16.2 | 13.1 | 30.2 | 27.4 | <0.001 | <0.001 | <0.001 | 0.59 |
Stroke, % | 7.8 | 5.9 | 14.7 | 21.1 | <0.001 | <0.001 | <0.001 | 0.13 |
History of established CVD, % | 21.3 | 17.4 | 36.9 | 42.1 | <0.001 | <0.001 | <0.001 | 0.36 |
AF, % | 9.9 | 7.6 | 19.4 | 23.2 | <0.001 | <0.001 | <0.001 | 0.41 |
HF, % | 11.9 | 8.3 | 27.9 | 26.3 | <0.001 | <0.001 | <0.001 | 0.77 |
CKDa, % | 6.7 | 4.4 | 17.0 | 16.8 | <0.001 | <0.001 | <0.001 | 0.97 |
COPDa, % | 5.3 | 4.3 | 8.2 | 13.7 | <0.001 | 0.002 | <0.001 | 0.11 |
Asthmaa, % | 5.8 | 6.3 | 3.2 | 3.2 | 0.04 | 0.03 | 0.21 | 0.97 |
History of cancera, % | 11.8 | 10.5 | 15.9 | 22.1 | <0.001 | 0.004 | <0.001 | 0.16 |
The frequency of treatment with the selected CV drugs is presented in Table 2.
Variable | N | All patients (n = 2346) | Group 1: alive (n = 1910) | Group 2: in‑hospital death (n = 341) | Group 3: death during the follow‑up (n = 95) | P value (ANOVA) | 1 vs 2 | 1 vs 3 | 2 vs 3 |
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin II receptor blocker; ASA, acetylsalicylic acid; MRA, mineralocorticoid receptor antagonist; others, see Table 1 | |||||||||
ACEI/ARB, % | 2346 | 28.3 | 29.1 | 22.9 | 31.6 | 0.049 | 0.02 | 0.61 | 0.08 |
β-Blocker, % | 2346 | 39.3 | 36.8 | 47.8 | 59.4 | <0.001 | <0.001 | <0.001 | 0.04 |
MRA, % | 2344 | 4 | 4 | 1.8 | 11.5 | <0.001 | 0.04 | <0.001 | <0.001 |
Statin, % | 2346 | 16.6 | 16 | 18.5 | 23.2 | 0.11 | 0.25 | 0.06 | 0.31 |
ASA, % | 2344 | 17.6 | 16.4 | 20.8 | 28.4 | 0.003 | 0.046 | 0.002 | 0.12 |
The patients who died during the hospitalization were less commonly treated with ACEIs/ARBs or MRAs than those who survived both the hospitalization and the follow‑up (P ≤0.04). The patients who died after discharge form the hospital were more often treated with β-blockers, MRAs, and ASA than those who survived in the post‑discharge period (P ≤0.002).
Independent predictors of in‑hospital death
Older age, a history of established CVD, HF, and CKD were independently associated with higher odds of in‑hospital death, while a history of asthma and treatment with ACEIs/ARBs, MRAs, and statins correlated with a lower risk of in‑hospital death (Table 3).
Evaluated variable | In‑hospital death | Death during the follow‑up | ||
Model 1 | Model 2 | Model 3 | Model 4 | |
Data are presented as odds ratios (95% CIs).
a Without established cardiovascular disease
Abbreviations: see Table 2 | ||||
Clinical characteristics | ||||
Male sex | – | – | – | – |
Age (per 10‑year increase) | 1.08 (1.07–1.09) | 1.1 (1.08–1.12) | 1.08 (1.06–1.1) | 1.09 (1.06–1.12) |
Presence of CV risk factorsa | – | – | – | – |
History of established CVD | 1.55 (1.09–2.22) | – | 1.83 (1.02–3.27) | – |
AF | – | – | – | – |
HF | 1.77 (1.24–2.55) | 1.76 (1.11–2.77) | – | – |
CKD | 2.58 (1.68–3.96) | 2 (1.16–3.46) | 2.04 (1.04–4.01) | – |
COPD | – | – | – | – |
Asthma | 0.44 (0.22–0.87) | – | – | – |
History of cancer | – | – | 2.01 (1.16–3.5) | – |
Cardiovascular drugs (recognized as influencing the prognosis) | ||||
ACEI/ARB | 0.47 (0.34–0.64) | 0.48 (0.32–0.71) | – | – |
β-Blocker | – | – | – | – |
MRA | 0.2 (0.08–0.48) | 0.19 (0.06–0.55) | – | – |
Statins | 0.69 (0.48–0.99) | – | – | – |
ASA | – | – | – | – |
Clinical condition on admission | ||||
SpO2 (per 10% increase) | – | 0.92 (0.89–0.94) | – | 0.93 (0.9–0.97) |
SBP (per 10 mm Hg increase) | – | 0.99 (0.98–1) | – | 0.98 (0.97–1) |
DBP (per 10 mm Hg increase) | – | – | – | – |
HR (per 5 bpm increase) | – | 1.04 (1.02–1.05) | – | – |
In the next model, which included variables reflecting the clinical condition assessed on admission (blood pressure, heart rate, and oxygen saturation) along with the aforementioned variables, a history of HF and CKD, as well as increased heart rate, correlated with a higher risk of death, whereas treatment with ACEIs/ARBs or MRAs, as well as higher systolic blood pressure (SBP) and oxygen saturation, were associated with a lower risk of in‑hospital death.
Among the patients over 65 years of age, the predictors of death were similar to those identified in the whole study population (Supplementary material, Table S1). In the group of patients younger than 65 years, the presence of CVD risk factors, HF, and CKD were among the independent predictors of in‑hospital death. The use of CV drugs was not an independent predictor of in‑hospital death in this group (Supplementary material, Table S2).
Independent predictors of death during the follow‑up
The same models were constructed to evaluate the predictors of death during the follow‑up. This analysis showed that older age, a history of established CVD, CKD, and a history of cancer were associated with a higher risk of death during the follow‑up. In the model considering the clinical condition on admission, higher oxygen saturation and SBP were associated with better prognosis.
In the patients older than 65 years, the predictors of death were similar to those identified in the whole study population; however, the use of statins during the hospitalization positively influenced prognosis after discharge (Supplementary material, Table S1). In the group of patients younger than 65 years, few deaths during the follow‑up were observed, which precluded a meaningful analysis (Supplementary material, Table S2).
Discussion
This study demonstrates that the patients with COVID‑19 who survived both the hospitalization and the follow‑up were younger and had a lower prevalence of established CVD than the nonsurvivors. They were also characterized by a lower prevalence of other concomitant diseases. The patients who died during the hospitalization, as compared with those who died during the follow‑up, had a similar prevalence of CVD and other concomitant diseases. We showed that established CVD and CKD were the main predictors of death, whereas the use of CV drugs had a beneficial effect on survival. Moreover, we found that the presence of CV risk factors did not increase the odds of either in‑hospital or post‑discharge death.
Data from previous studies6,8 showed that CV risk factors, including hypertension, diabetes mellitus, and hypercholesterolemia, were associated with higher in‑hospital mortality in COVID‑19 patients; however, these observations were not confirmed in other analyses.11,22-24 Our findings support those of the latter studies, since we showed that CKD and established CVD were independent predictors of in‑hospital death but the presence of CV risk factors was not. Identification of independent predictors of death in COVID‑19 is important to select high‑risk patient groups, thus allowing to implement targeted intervention strategies. Based on our data, the risk of in‑hospital mortality in COVID‑19 patients seems to be similar in the individuals with and without CV risk factors, in the absence of CVD. The novel finding of our study is that the presence of CV risk factors is not a predictor of death during COVID‑19 hospitalization, while established CVD poses a significant risk. This finding highlights the importance of CVD prevention for the reduction of mortality in COVID‑19.25-28
At the beginning of the COVID‑19 pandemic, the use of renin‑angiotensin‑aldosterone system (RAAS) blockers was a matter of concern due to their potential for worsening the COVID‑19 course,14 which was not confirmed by later studies.11,16-18 Moreover, further observations have shown that the use of RAAS blockers is not only safe but also improves the prognosis.29-31 Our observations are in line with the results of those studies, showing beneficial effects of ACEI/ARB use on survival probability among patients hospitalized for COVID‑19. In addition, we showed that treatment with MRAs also improves prognosis, and that they can be used in the prevention of acute complications of COVID‑19, including HF, as formerly suggested by Chowdhury et al.29 Previous studies32,33 indicated that statins had a positive effect on survival in COVID‑19 patients. Our findings support this observation.
Most studies conducted so far focused mainly on post–COVID‑19 complications; few of them considered the topics of long‑term mortality and independent predictors of death during the follow‑up. Among such analyses, an Estonian study by Uuskula et al34 assessed the long‑term all‑cause mortality after SARS‑CoV‑2 infection in a group of 66 267 patients in comparison with a reference group of uninfected individuals (n = 254 969). They reported that in the individuals with SARS‑CoV‑2 infection, the mortality rate substantially increased during 12 months post infection, driven by deaths in older people (>60 years). Among the older participants, the risk of CV death was the highest during the first 5 weeks of the follow‑up, and the mortality rate was driven by deaths due to hypertensive heart disease, chronic ischemic heart disease, CKD, stroke, and myocardial infarction.34 This is in accordance with our results that also emphasize the impact of established CVD on long‑term postdischarge mortality in the patients hospitalized for COVID‑19.
The present Cor‑Cardio study has several limitations. First, the study population was relatively small and comprised patients from 13 centers. However, it can be assumed that the patients were managed in a similar way, in accordance with the general regulations on the management of patients with COVID‑19 in Poland. Second, it was a retrospective analysis that only included data available from hospital computer systems, with no information about treatment in the postdischarge period. Third, we acknowledge that our analysis of biochemical parameters was based on a single‑time measurement performed on admission, and must have been influenced by the infection status. Finally, we implemented the same statistical model to analyze the predictors of in‑hospital and postdischarge mortality. The differences in the follow‑up duration may have influenced our results.
To conclude, established CVD, but not the presence of CV risk factors, correlated with a higher risk of in‑hospital death and death during the follow‑up. The use of CV drugs during hospitalization was associated with better prognosis.
- Nosalski R, Siedlinski M, Denby L, et al. T‑cell‑derived miRNA‑214 mediates perivascular fibrosis in hypertension. Circ Res. 2020; 126: 988‑1003. | Crossref
- Chrzan R, Wojciechowska W, Terlecki M, et al. The role of artificial intelligence technology analysis of high‑resolution computed tomography images in predicting the severity of COVID‑19 pneumonia. Pol Arch Intern Med. 2022; 132: 16332. | Crossref
- Saeed S, Tadic M, Larsen TH, et al. Coronavirus disease 2019 and cardiovascular complications: focused clinical review. J Hypertens. 2021; 39: 1282‑1292. | Crossref
- Carfi A, Bernabei R, Landi F; Gemelli Against COVID‑19 Post‑Acute Care Study Group. Persistent symptoms in patients after acute COVID‑19. JAMA. 2020; 324: 603‑605. | Crossref
- Klocek M, Wojciechowska W, Terlecki M, et al. Cardiac biomarkers on admission and in‑hospital mortality in COVID‑19 patients with or without concomitant heart failure. Pol Arch Intern Med. 2022; 132: 16256. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION