Mobile application and digital system for patients after myocardial infarction: early results from a randomized trial
Key words: acute myocardial infarction, cardiac rehabilitation, mobile application, telehealth, telemedicine



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Mobile application and digital system for patients after myocardial infarction: early results from a randomized trial
Introduction: Cardiac rehabilitation (CR) is a complex program aimed at better control of cardiovascular risk factors. It can be supported by mobile applications. Despite promising results from previous studies on telemedicine tools, there is a paucity of evidence when it comes to prospective randomized trials.
Objectives: The aim of this study was to comprehensively evaluate a newly‑developed mobile application called “afterAMI” in the clinical setting, and to assess the impact of the application‑supported model of care in comparison with standard rehabilitation.
Patients and methods: A total of 100 patients with myocardial infarction were recruited on admission to the Department of Cardiology at the Medical University of Warsaw. The patients were randomized into the group with an access to the afterAMI application or to the standard CR. Cardiovascular risk factors were analyzed along with the number of rehospitalizations and patient knowledge regarding cardiovascular risk factors. The analysis focused on the results obtained 30 days after discharge.
Results: Median age of the patients was 61 years (interquartile range, 51–67 years), and 65% of the participants were men. There were no differences in cardiovascular risk factor control between the study groups, apart from low‑density lipoprotein cholesterol levels, which were lower in the group using the afterAMI application (P <0.001), despite no differences being found at the beginning of the study. Similarly, a significant difference in N‑terminal pro–B‑type natriuretic peptide levels was observed after 30 days (P = 0.02), despite a lack of significant differences at randomization.
Conclusions: This study serves as an example of a telemedicine tool being implemented into everyday practice. The augmented rehabilitation program resulted in better control of cholesterol level. Longer follow‑up is required to establish prognosis in this population.
What's new?
It is important to prevent future heart attacks in patients who have suffered from acute myocardial infarction (AMI), for example by controlling the risk factors. Our study demonstrated that everyday care in such patients may be improved with a novel telemedicine solution. Supporting a standard rehabilitation with a dedicated mobile application, a simple and harmless tool, resulted in better control of the cardiovascular disease risk factors, such as low‑density lipoprotein cholesterol level. These results may contribute to telemedicine being introduced into standard medical practice and to improved care for postAMI patients.
Introduction
Cardiovascular disease (CVD) remains a huge challenge for both societies and individuals, carrying a substantial burden in terms of mortality and disability. In recent decades, significant progress has been made in the treatment of acute myocardial infarction (AMI) due to novel invasive procedures and tailored pharmacotherapy schemes. There are still major differences between countries regarding treatment outcomes, but in general, lower mortality has been observed.1 Nevertheless, approximately 10% of AMI patients die within a year of hospital discharge.2 It has been emphasized several times how important it is to control CVD risk factors in the patients in secondary prevention.3 According to data published by Jankowski et al,4 only 2.9% of patients with coronary artery disease (CAD) control all CVD risk factors according to the recommended values, with worse control in women than in men.5 Moreover, another study found that over 25% of patients died within 5 years after hospitalization for AMI in Poland.6 Only one‑third of the patients underwent cardiac rehabilitation (CR) during the 12 months following AMI. It seems that there is a huge potential for further decrease in mortality in the patients suffering from myocardial infarction (MI) in Poland.7 Up to 45% of deaths due to recurrent MI are preventable.3 It is crucial to constantly look for potential optimization, which could result in improved prognosis.
A number of approaches have been tested in several clinical trials aimed at improving prognosis of the patients. One of the newest solutions is based on the use of novel telemedicine devices and systems. There are approximately 6 billion smartphones in use globally, and the market is estimated to continue its growth.8 Therefore, implementing mobile applications into everyday clinical practice seems a natural step forward. Protocols and results of studies including mobile application use by patients after MI have been published.9-11 Moreover, some of them have shown promising results and improved blood pressure control.12 In a preliminary study published a few years ago, Widmer et al13 demonstrated that augmenting a regular CR program with an online and smartphone‑based program improved CVD risk factor management and reduced rehospitalizations and emergency department visits by 40% (P <0.05).
According to the available literature, cardiac patients use mobile applications mainly to access information about illnesses and drugs.14 However, the potential of dedicated mobile applications is much greater, and it seems that this solution is underutilized in the clinical settings. In a meta‑analysis published by Coorey et al,15 mobile applications were found to have a positive effect on CVD risk factor control, which is crucial in secondary prevention.
It should also be pointed out that both national and international societies recommended broader use of telehealth solutions.16,17 On the other hand, adding these solutions to everyday clinical practice remains a challenge, perhaps partially due to the unsatisfactory amount and quality of evidence. In this study, we aimed to investigate the impact of a novel telemedicine solution on rehospitalizations and / or urgent outpatient visits and on CVD risk factor control in patients after MI.
Patients and methods
Study design
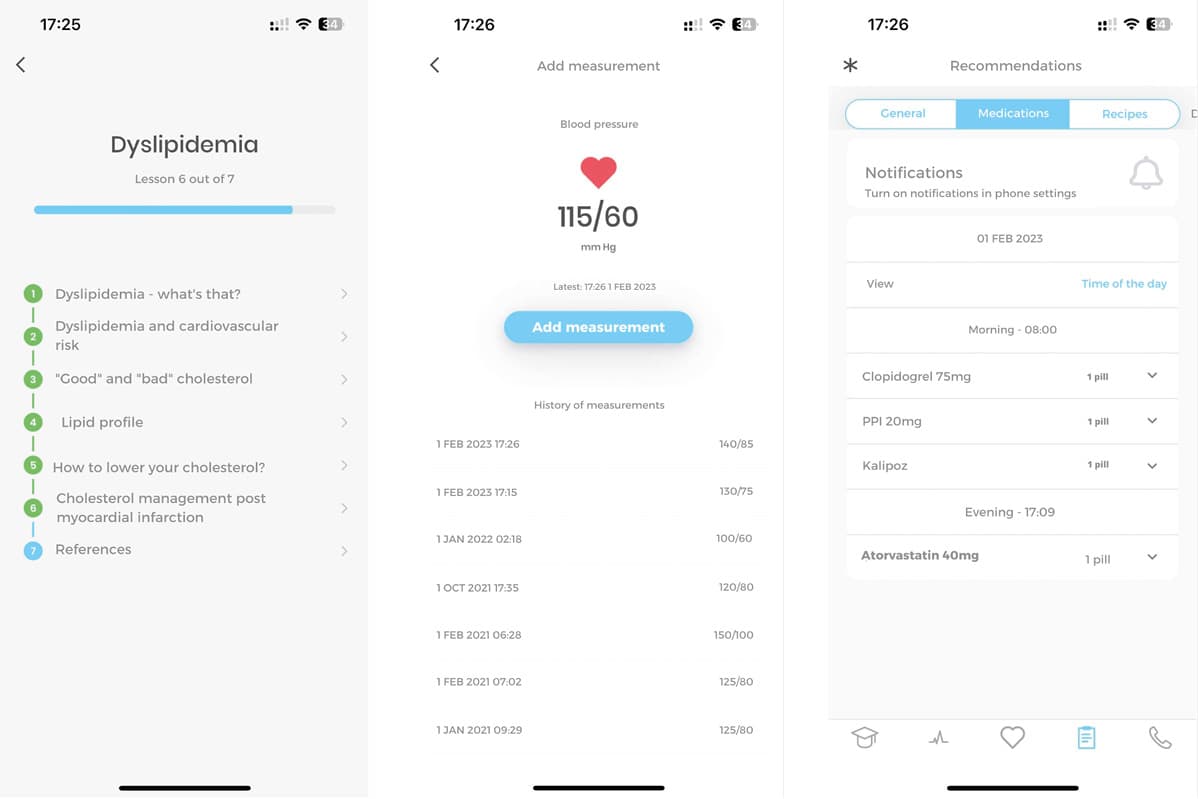
This study included data from the ongoing single‑center, randomized, open afterAMI trial (Mobile App and Digital System for Patients After Myocardial Infarction), registered at ClinicalTrials.gov (NCT04793425). The study was approved by a local ethical review board (KB/150/2020), and informed consent was obtained from each patient. Detailed description of the study design and methods has been provided in another paper.18 In brief, the study included patients who were hospitalized for AMI at the Department of Cardiology, Medical University of Warsaw, between 2019 and 2021. Following current guidelines, the diagnosis was made based on symptoms, troponin concentration, and electrocardiography results.19 The patients were randomized (1:1) into either the control group (CG), which underwent regular CR, or the intervention group (IG), where rehabilitation was supported by the use of a dedicated mobile application. Briefly, the application provides patients with an access to educational content about their diseases. Every educational tab was prepared by a cardiologist experienced in managing post‑AMI patients. Additionally, every patient regularly received messages with notifications about the recommended lifestyle interventions and promoting adherence to the therapy. All the messages were prepared based on the recommendations of the European Society of Cardiology (ESC).3 Another essential feature of the application is a panel dedicated to reporting vital signs (blood pressure, heart rate, weight, saturation, and glycemia), which were analyzed on a daily basis, and if necessary, a short message was sent to the patient, advising them to present to a primary health care clinic or an emergency department. The patients were instructed to report their parameters daily. Moreover, the application sent notifications with reminders about taking medications.
On top of that, the application includes a module with air pollution parameters measured according to the localization setup. Additionally, a medical history tab is created for each patient, based on their hospital discharge summary. This way, the patients always have a brief history of their coronary interventions at hand. This knowledge might be crucial for the physicians performing subsequent percutaneous coronary interventions, and could potentially decrease time‑to‑balloon. Finally, the application offers a contact panel to text and call the cardiologists at the hospital.
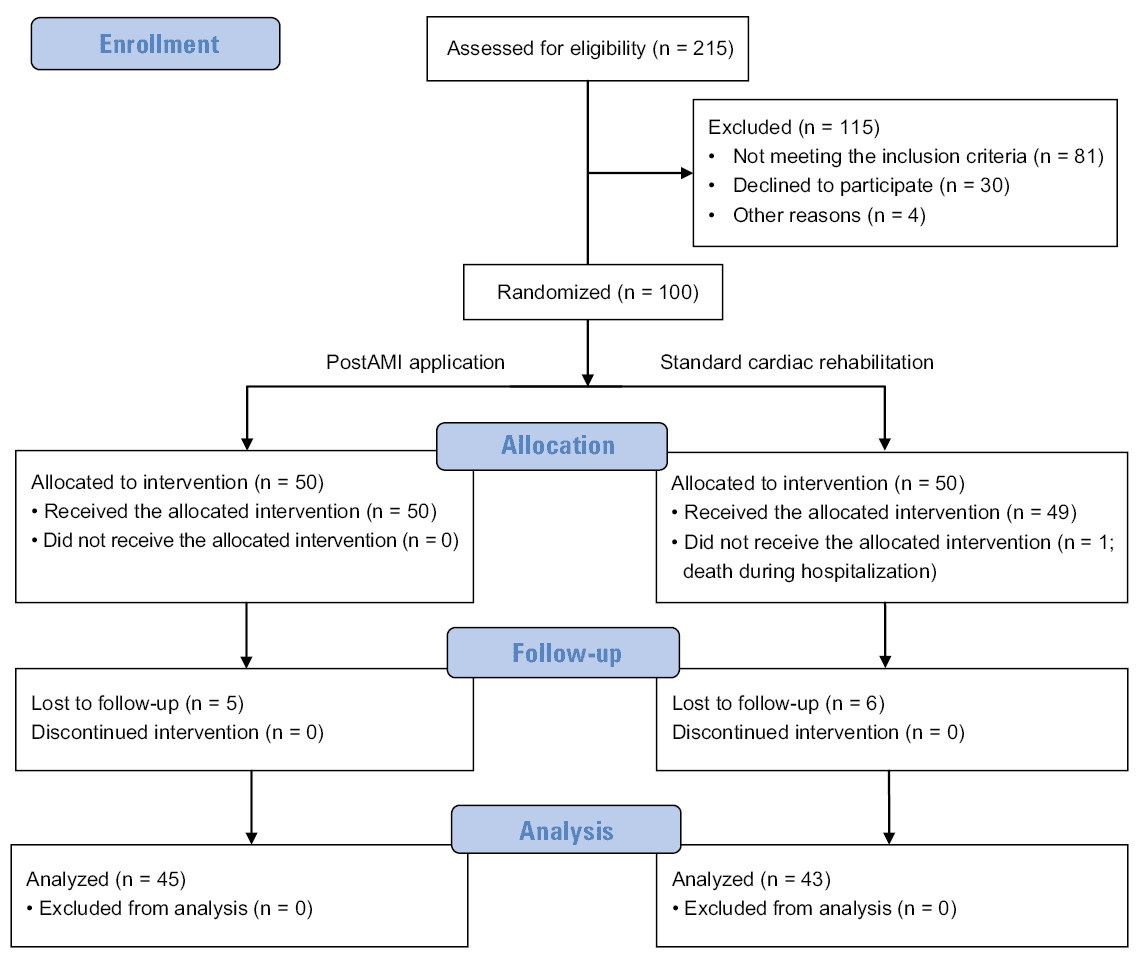
All demographic, clinical, and laboratory data, quality of life questionnaires, and information regarding AMI etiology and medication at discharge were collected in the application. All end points were set to be assessed twice: at 30 days and 6 months after randomization. A flowchart of the study is presented in Figure 1.
Study end points
The primary outcome included the need for rehospitalization and / or urgent outpatient visit between the baseline and the follow‑up visit 6 months after randomization. Moreover, there were 5 secondary outcomes related to cardiovascular risk factor control: blood pressure, body mass, smoking status, dyslipidemia, and the need for rehospitalization and / or urgent outpatient care within the first 30 days after randomization. Detailed target values regarding risk factor control were presented previously.18 Each target was categorized as being met or not. Secondary outcomes also included quality of life and depression severity assessment (MacNew, EQ‑5D‑5L, and DASS‑21 questionnaires), knowledge about cardiovascular risk factors (CVD risk factors, recommended blood pressure values, and desired lifestyle intervention identification), and return to work in the case of employed patients. The other collected data were demographic parameters (sex and age) and laboratory test results.
Statistical analysis
In terms of the end points, we looked at the frequency of the events. Regarding secondary end points, a change from the baseline and the frequency of rehospitalizations and / or urgent outpatient visits within 30 days after randomization were assessed. The distribution of continuous variables was estimated using the Shapiro–Wilk test. Continuous variables with a normal distribution are presented as mean values with SD. All continuous variables with a non‑normal distribution are presented as median values and interquartile ranges (IQRs). In the case of variables with normal and non‑normal distribution, the groups were compared using the t test and the nonparametric Mann–Whitney test, respectively. The comparison of qualitative variables between the groups was performed with the Fisher exact test. For quantitative variables, the change from the baseline was assessed. Per‑protocol analysis was performed after all the follow‑up visits had been completed. The analysis included all patients who met the inclusion criteria and signed the informed consent form, regardless of whether the follow‑up was completed. In the case of missing data, the patients were excluded from the specific analysis.
Results
The analysis of the afterAMI study included 100 patients. During hospitalization, 50 patients were randomized to the IG and 50 to the CG. Unfortunately, 11 individuals were lost to follow‑up (5 from the IG and 6 from the CG). One patient did not receive the allocated intervention due to his death during the initial hospitalization. A summary of patient characteristics at baseline is presented in Table 1. The 2 groups did not differ significantly at baseline in terms of sociodemographic characteristics (sex, body weight, and general cardiovascular risk factors). The median age of the entire study group was 61 years (IQR, 51–67), and 65% of the participants were men. The individuals assigned to the CG were older (63.42 [IQR, 56–69] years vs 56.8 [IQR, 51–65] years in the IG; P = 0.002). Both heart failure (HF) and atrial fibrillation were more prevalent in the CG. Over the 30‑day period, more patients in the IG achieved target low‑density lipoprotein cholesterol (LDL‑C) concentration than in the CG (27 [58.06%] vs 9 [21.88%]; P = 0.005). Similarly, a significant difference in median N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) levels was observed (257 pg/ml [IQR, 127.5–502.5] in the IG vs 626 pg/ml [IQR, 254–1043] in the CG; P = 0.02), despite a lack of significant differences at randomization (422 pg/ml [IQR, 133–1256] in the IG vs 886.5 pg/ml [IQR, 230–2250] in the CG; P = 0.07).
Variable | Intervention group | Control group | P value | |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
P values <0.05 were considered significant.
SI conversion factors: to convert creatinine to μmol/l, multiply by 88.4; NT‑proBNP to ng/l, by 1; hemoglobin to g/l, by 10; total cholesterol, HDL‑C, and LDL‑C to mmol/l, by 0.0259; TG to mmol/l, by 0.0113.
Abbreviations: AMI, acute myocardial infarction; ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor neprilysin inhibitor; ASA, acetylsalicylic acid; BMI, body mass index; CCB, calcium channel blockers; CR, cardiac rehabilitation; CVD, cardiovascular disease; DOAC, direct oral anticoagulant; EF, ejection fraction; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HDL‑C, high‑density lipoprotein cholesterol; ICD, implantable cardioverter‑defibrillator; LAD, left anterior descending artery; LCA, left circumflex artery; LDL‑C, low‑density lipoprotein cholesterol; MRA, aldosterone receptor antagonists; NSTEMI, non–ST‑segment elevation myocardial infarction; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; PCI, percutaneous coronary intervention; RCA, right coronary artery; STEMI, ST‑segment elevation myocardial infarction; TG, triglycerides; VKA, vitamin K antagonist; WBC, white blood cells | ||||
Clinical data | ||||
Age, y, mean (SD) | 56.8 (9.23) | 63.42 (11.4) | 0.002 | |
BMI, kg/m2, mean (SD) | 28.5 (4.06) | 28.11 (5.38) | 0.72 | |
Body weight, kg, mean (SD) | 88.95 (13.86) | 85.47 (24.33) | 0.46 | |
Height, cm, mean (SD) | 176.3 (7.23) | 171.6 (8.97) | 0.02 | |
Male sex | 34 (68) | 31 (61) | 0.67 | |
Comprehensive coordinated care after myocardial infarction (KOS‑Zawał) | 17 (34) | 9 (18) | 0.11 | |
CR (KOS‑Zawał and outside of KOS‑Zawał combined) | 27 (54) | 22 (44) | 0.42 | |
Duration of hospitalization, d | 6 (4–8) | 7 (5–11) | 0.21 | |
STEMI | 25 (50) | 20 (40) | 0.42 | |
NSTEMI | 25 (50) | 30 (60) | 0.42 | |
Infarction artery | LAD | 26 (52) | 24 (48) | >0.99 |
LCA | 15 (30) | 17 (34) | 0.52 | |
RCA | 16 (32) | 24 (48) | 0.14 | |
PCI | 39 (78) | 39 (78) | 0.62 | |
Bypass surgery | 5 (10) | 6 (12) | 0.76 | |
Smoking | 33 (66) | 32 (64) | >0.99 | |
Pack‑years | 20 (0–30) | 14 (0–32.5) | 0.79 | |
Type 1 diabetes | 2 (4) | 0 | 0.49 | |
Type 2 diabetes | 11 (22) | 11 (22) | >0.99 | |
Hypertension | 30 (60) | 34 (68) | 0.38 | |
Dyslipidemia | 36 (72) | 39 (78) | 0.31 | |
Atrial fibrillation / atrial flutter | 1 (2) | 7 (14) | 0.03 | |
Heart failure | 6 (12) | 15 (30) | 0.03 | |
Implanted pacemaker or ICD | 1 (2) | 5 (10) | 0.11 | |
Chronic kidney disease | 1 (2) | 1 (2) | >0.99 | |
Peripheral artery disease | 1 (2) | 1 (2) | >0.99 | |
EF at enrollment, %, mean (SD) | 51.78 (8.42) | 48 (9.22) | 0.04 | |
Knowledge about CVD risk factors | 8 (6–9) | 8 (4–9) | 0.41 | |
Employed | 27 (54) | 17 (34) | 0.13 | |
Laboratory tests at hospital | ||||
Troponin I, μg/l | 0.79 (0.22–5.57) | 0.69 (0.11–4.35) | 0.72 | |
Troponin II, μg/l | 2.25 (0.71–8.73) | 5.64 (0.44–34.63) | 0.17 | |
Creatinine, mg/dl, mean (SD) | 0.98 (0.21) | 1.05 (0.34) | 0.20 | |
eGFR, ml/min/1.73 m2, mean (SD) | 79.16 (17.22) | 73.28 (20.93) | 0.14 | |
Na, mmol/l, mean (SD) | 139.1 (3.05) | 139.6 (4.36) | 0.54 | |
K, mmol/l, mean (SD) | 4.17 (0.45) | 4.38 (0.51) | 0.04 | |
WBC, × 109/l, mean (SD) | 10.27 (3.04) | 10.19 (2.94) | 0.91 | |
HbA1c, % | 5.8 (5.4–7.1) | 5.6 (5.4–6) | 0.46 | |
NT‑proBNP, pg/ml | 422 (133–1256) | 886.5 (230–2250) | 0.07 | |
Hemoglobin, g/dl, mean (SD) | 14.58 (1.49) | 14.14 (1.83) | 0.20 | |
Total cholesterol, mg/dl, mean (SD) | 191.3 (71.57) | 192.1 (52.29) | 0.95 | |
HDL‑C, mg/dl, mean (SD) | 39.55 (10.02) | 46.78 (10.65) | 0.001 | |
LDL‑C, mg/dl, mean (SD) | 117.5 (68.59) | 111.7 (61.56) | 0.66 | |
TG, mg/dl | 146 (92–233) | 136.5 (87–201) | 0.24 | |
Drugs at discharge | ||||
ACEI | 42 (84) | 40 (80) | 0.52 | |
ARB | 4 (8) | 2 (4) | 0.23 | |
ARNI | 0 | 0 | – | |
MRA | 9 (18) | 15 (30) | 0.23 | |
β-Blocker | 42 (84) | 41 (82) | 0.74 | |
CCB | 20 (40) | 10 (20) | 0.03 | |
Statin | 46 (92) | 45 (90) | >0.99 | |
Ezetimibe | 5 (10) | 2 (4) | 0.27 | |
VKA | 0 | 0 | – | |
DOAC | 1 (2) | 2 (4) | >0.99 | |
ASA | 45 (90) | 43 (86) | >0.99 | |
Clopidogrel | 12 (24) | 13 (26) | >0.99 | |
Prasugrel | 2 (4) | 0 | 0.24 | |
Ticagrelor | 28 (56) | 28 (56) | >0.99 | |
Digoxin | 0 | 0 | – | |
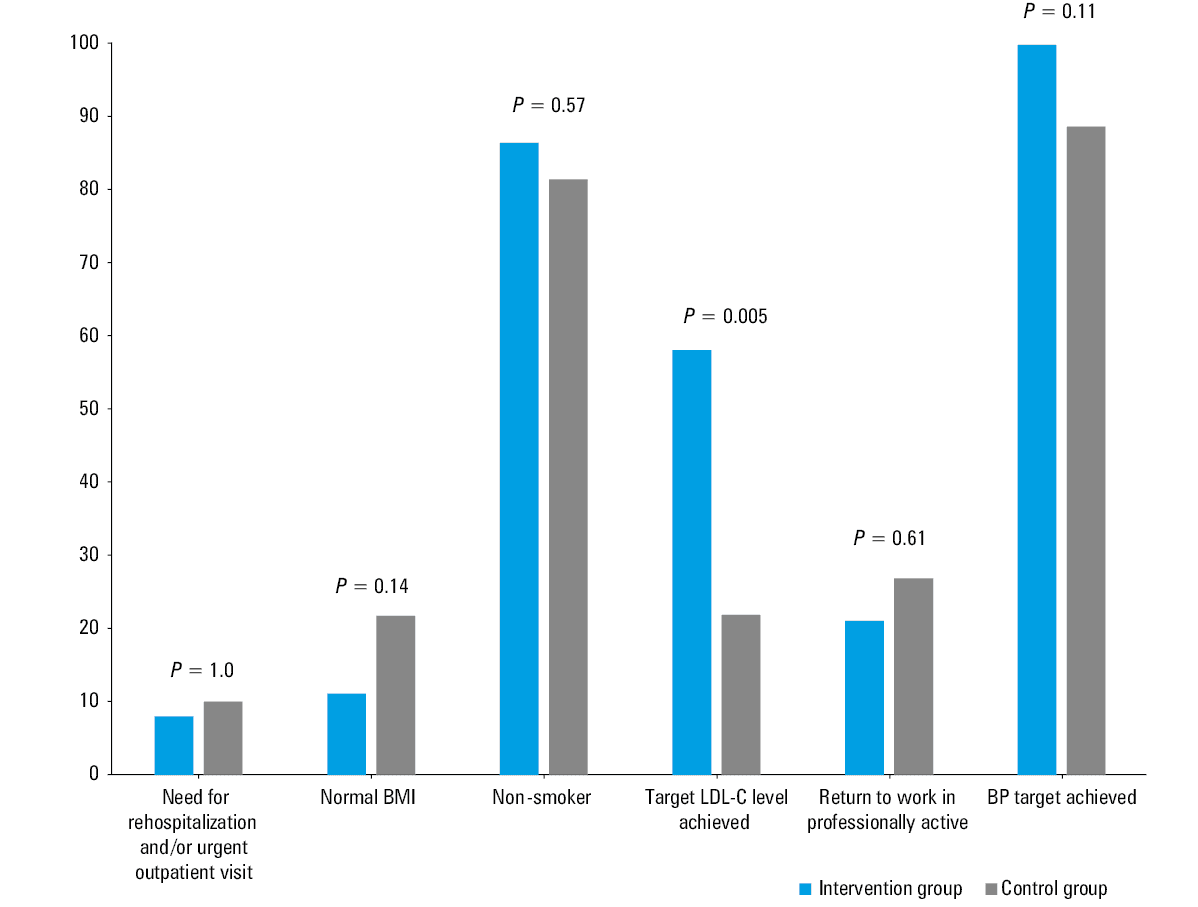
There was no significant difference between the groups regarding the need for rehospitalization and / or urgent outpatient care (4 [8%] in the IG vs 5 [10%] in the CG; P >0.99). Fewer patients in the IG had the body mass index (BMI) within the normal range (5 [11.1%] vs 10 [21.73%]; P = 0.14). Fewer patients in the IG smoked at follow‑up (35 [81.39%] vs 39 [86.67%]; P = 0.57). At the beginning of the study, the groups did not differ in their smoking status (33 [66%] in the IG vs 32 [64%] in the CG; P >0.99). More patients using the afterAMI application met the blood pressure target value, but the difference was not significant (44 [98.78%] vs 39 [88.63%]; P = 0.11). A summary of the results is presented in Figure 2 and Table 2. An overall trend toward better CVD risk factor control in the IG patients was demonstrated. Exemplary screens from the application can be found in Figure 3 and Supplmentary material.
Abbreviations: BP, blood pressure; others, see Table 1
End point | Intervention group | Control group | P value |
Data are presented as mean (SD) or median (interquartile range).
P values <0.05 were considered significant.
SI conversion factors: see Table 1
Abbreviations: see Table 1 | |||
Creatinine, mg/dl | 1.02 (0.18) | 1.01 (0.29) | 0.78 |
eGFR, ml/min/1.73 m2 | 78.73 (16.23) | 74.5 (19.7) | 0.34 |
HbA1c, % | 5.8 (5.6–6.6) | 5.75 (5.5–6) | 0.35 |
NT‑proBNP, pg/ml | 257 (127.5–502.5) | 626 (254–1043) | 0.02 |
Hemoglobin, g/dl | 14.38 (1.46) | 13.87 (1.15) | 0.12 |
Total cholesterol, mg/dl | 116.5 (30.43) | 143.9 (36.93) | 0.002 |
HDL‑C, mg/dl | 41.53 (8.64) | 47.79 (12.7) | 0.023 |
LDL‑C, mg/dl | 48.16 (25.97) | 73.45 (28.91) | <0.001 |
TG, mg/dl | 106.0 (86.5–136.5) | 99.5 (79.5–152.5) | 0.96 |
Discussion
In the afterAMI study we evaluated the impact of the CR augmentation with a mobile application. Despite some differences between the compared groups, which could have been due to a relatively small sample size, the IG patients had significantly lower LDL‑C and NT‑proBNP levels, with no significant differences at randomization.
Providing CAD patients with continuity of care remains a challenge, as over time many patients return to their previous habits, including a sedentary lifestyle, poor diet, and smoking. As a result, their cardiovascular health deteriorates, potentially leading to further adverse cardiac events. Therefore, investigating novel solutions to support risk factor control, educate patients, and sustain their motivation is crucial to improving long‑term prognosis.
According to the latest ESC guidelines, participation in CR programs is highly recommended after AMI and / or revascularization in chronic coronary syndrome (class I, level A).3 The definition of CR extends far beyond physical exercise. It should be considered a multidisciplinary intervention involving psychosocial support, patient education, dietary counselling, and risk factor modification. As indicated by several systematic reviews, CR programs effectively contribute to improved blood pressure, heart rate, body mass, and lipid profile.20 Moreover, many studies have demonstrated the beneficial effects of CR programs on clinical outcomes through reduced rates of recurrent MI, cardiovascular hospitalization and mortality, and all‑cause mortality.21,22 Patient motivation in terms of lifestyle improvement is the highest immediately after discharge from the hospital. The aim of providing the patients with the application was to maintain the highest achievable level of motivation for as long as possible. Similar conclusions were reached by Sinnadurai et al,23 who stated that a long‑term strategy to sustain the beneficial CR effects should be applied.
The market of digital health solutions is growing exponentially and is considered a promising approach. There are a variety of potential applications of telemedicine in CR, ranging from web‑based nationwide systems and online counselling platforms, through home‑based exercise programs, to mobile applications. However, only a few mobile applications have been adequately validated by demonstrating their evidence‑based effectiveness. The current ESC guidelines on CVD prevention state that mobile health (mHealth) solutions should be considered user‑friendly, economically attractive tools for risk factor control, promoting not only better therapy adherence but also lifestyle modifications in long‑term patient management.3
The principal finding of this analysis is that augmenting CR with a mobile application resulted in a significant reduction in LDL‑C concentrations and facilitated meeting guideline‑recommended target values in AMI patients during a 30‑day follow‑up. However, one should consider baseline differences between the randomized groups when analyzing the results. Already significant cholesterol level reduction in the IG patients might have been even greater thanks to some features of the application, such as expanded educational panel and medication reminder option. The use of mHealth technologies for improving cardiovascular risk factor control in CAD patients has already been widely explored. Although early feasibility studies showed promising results,13,24 more contemporary findings seem to be slightly conflicting. Some mobile applications are aimed at improving single risk factors, for example, physical activity25 or blood pressure.26 However, the researchers currently tend to present a more holistic approach,12 targeting most of the modifiable risk factors simultaneously, which is a strategy that we also decided to adapt. The patients in the IG had significantly lower NT‑proBNP level. Since this molecule has been found to be an independent prognostic factor for HF development and future coronary events,27 we believe the IG has therefore better prognosis.
In some cases, improvement was observed for only a single risk factor. In a study by Lunde et al,28 the only significant differences were demonstrated for improved peak oxygen uptake, exercise performance, and exercise habits of the application‑equipped patients.28 Another application contributed to significantly improved blood pressure and dietary habits in the first months after MI, with a nonsignificant trend toward better exercise capacity and higher smoking cessation rates.12 However, due to difficulties with objective dietary changes assessment, we decided to focus on other end points, which might be indirectly or sometimes directly influenced by dietary habits. Studies conducted by Michelsen et al12 and by Lunde et al28 focused on the outcomes after 25 weeks and 1 year, respectively, therefore comparing them with our findings would be misleading. While Johnston et al29 found no differences between their groups in BMI, physical activity, or smoking, a significant reduction in LDL‑C concentrations in the intervention group was achieved during a 6‑month follow‑up. The patients also had a visit scheduled 6–10 weeks after the discharge, but no laboratory investigations were presented in the study, making it impossible to directly compare it with our results.29 Nevertheless, the trend toward lower LDL‑C level was similar to that observed in our study. Commonly, an overall but insignificant trend for improved control of other risk factors can be observed. However, considering significant heterogeneity of the proposed interventions in terms of technology and duration, as well as the sample size and clinical outcomes, drawing clear conclusions remains a challenge.
One of the features of the investigated application is the patient education module. Poor health literacy among patients has been associated with increased hospitalization rates and greater emergency care use, resulting in higher costs for the health care system.30 This further confirms the vital role of the patient education in the long‑term management. The mobile‑based educational materials can be provided in various forms, including podcasts, videos, articles, daily checklists, chatrooms for professional counselling, etc. The afterAMI application has an option to send notifications in the form of short, motivational text messages about healthy lifestyle habits, directing the user to the corresponding educational module with a click. Personalized, patient‑tailored lifestyle advice supported by mobile phone text messages has been proven to be a clinically effective and cost‑effective solution in smoking cessation,31 hypertension management,32 and glycemic control in diabetic patients.33 Interestingly, the results of the TEXTMEDS (Text Messages to Improve Medication Adherence and Secondary Prevention After Acute Coronary Syndrome) trial34 suggest that after acute coronary syndrome, cardiac education and support delivered via text message did not impact medical adherence, but small positive effects on lifestyle risk factors were noted. Patients in the IG in that trial more often met the BMI goals, which we did not observe in our study, and reported to have healthier dietary habits. The end points were assessed at 6 and 12 months.34 Those findings may suggest the need for a more complex and comprehensive approach involving multiple interventions instead of only text‑message–based management.
As with most novel solutions, to successfully implement mHealth in the long‑term management of CAD patients, one must overcome the barrier of the initial learning curve. With growing evidence on the clinical effectiveness and feasibility of mobile application use in this population, the most efficient strategies are expected to be established soon.
Improving the patient prognosis remains the main goal of optimizing risk factor control. In a recently published study,35 an application‑based model of care (TeleClinical Care) dedicated to patients who suffered from acute coronary syndrome or HF resulted in a significant reduction in unplanned hospital readmissions, higher rates of completing CR, better medication adherence, and proven cost‑effectiveness. Interestingly, such observations were not made for the short‑term follow‑up, which is in line with our results.
It should be noted that the rate of patients taking part in CR within comprehensive coordinated care after MI (called KOS‑Zawał in the case of our patients) and outside of it was relatively low but similar across the studied groups. Every eligible patient was given a referral for CR but the response rate seemed low. It might have been due to fact that the study was conducted in the middle of the COVID‑19 pandemic, and some patients refused to participate in any form of stationary CR due to the fear of SARS‑CoV‑2 infection. Future studies in nonpandemic times will show the influence of this mobile application on the end points mentioned above.
Several studies aimed at comparing the clinical effectiveness of digital and traditional models of CR. Hybrid CR is a combination of a stationary and telemedical rehabilitation. Participation in CR programs often requires multiple visits to a clinic, which can limit attendance, especially of patients living in rural areas. Therefore, telehealth interventions can successfully complement traditional CR. Moreover, mobile application interventions have been shown to improve traditional CR attendance, completion rates, and outcomes.36,37 Future digital interventions in CR may include smartphones or wearable devices for monitoring patient vital parameters during remote CR structured exercise, providing the patients with detailed instructions, allowing them to design their own activity schedules or create personalized exercise programs using artificial intelligence–based algorithms, or interacting with chatbots for educational purposes.37
The median age of patients suffering from AMI in Poland is 66.8 (IQR, 57.4–76.6) years.6 There is a general concern regarding the feasibility of mHealth interventions in older patients. However, the recently published American Heart Association statement on mobile health technologies in preventing cardiovascular disease among older adults points out that mobile technology can be effective in improving healthy behaviors and medication adherence.38 It indicates that in the context of an aging society, it is crucial to implement mHealth solutions to improve health outcomes in older adults suffering from CAD. Similarly, the results from the TeleCheck‑AF study39 indicate that older age correlates with better motivation and adherence.
Telemedicine is undoubtedly a field of extensive research. Recently, more and more studies have been exploring other potential applications of the mHealth‑based model of care. Our study seems to bring a piece of new evidence regarding mobile application use in AMI patients.
Limitations
Despite several strengths, certain limitations of our study should be discussed when interpreting the results. Firstly, the participants in the IG were younger and experienced fewer HF and atrial fibrillation events, which may be due to an insufficient number of randomized patients. It should be also mentioned that possibly younger and healthier patients from the IG were more eager to cooperate with their physicians, which translated into better adherence and finally LDL‑C level reduction. Larger studies with the afterAMI application are planned to overcome this issue. Also, a single‑center study should be regarded as a feasibility project and an introduction to a larger, multicenter study. Secondly, not all cardiac patients are capable of using smartphones. Gallagher et al14 reported that 54.6% of cardiac patients eligible for CR used technology for health purposes, which is similar to our findings. In the screened population, 62.23% of the patients were able to use the mobile application. Thus, the solution is not currently for everyone. However, since the adoption of technology increases, we believe this percentage will grow. It should be emphasized that this was not a blinded study, because it is impossible to blind patients in the mobile application interventions, as also stated in other similar studies. Moreover, it was not possible to objectively compare physical activity between the groups, as the patients in the CG were not equipped with any form of wearable activity trackers due to limited resources.
This was a pilot research with a 30‑day duration and, as such, it cannot be used to assess the effects of the afterAMI application on the long‑term outcomes in CAD patients. However, we intend to publish more findings on this subject.
Conclusions
Telemedicine solutions are widely discussed and are gaining momentum when it comes to augmenting standard care. Our study proves the feasibility of the mobile application support in MI patients. The benefits regarding LDL‑C level may contribute to improved prognosis. Nevertheless, the observation period should be prolonged, and larger, multicenter studies should be planned.
- Degano IR, Salomaa V, Veronesi G, et al. Twenty‑five‑year trends in myocardial infarction attack and mortality rates, and case‑fatality, in six European populations. Heart. 2015; 101: 1413‑1421. | Crossref
- Santos IS, Goulart AC, Brandao RM, et al. One‑year mortality after an acute coronary event and its clinical predictors: the ERICO study. Arq Bras Cardiol. 2015; 105: 53‑64. | Crossref
- Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021; 42: 3227‑3337.
- Jankowski P, Kosior DA, Sowa P, et al. Secondary prevention of coronary artery disease in Poland. Results from the POLASPIRE survey. Cardiol J. 2020; 27: 533‑540. | Crossref
- Setny M, Jankowski P, Kamiński K, et al. Secondary prevention of coronary heart disease in Poland: does sex matter? Results from the POLASPIRE survey. Pol Arch Intern Med. 2022; 132: 16179. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION