Unusual rapid progression of TAVI valve degeneration confirmed on PET-CT scan after the valve-in-valve procedure followed by early valve thrombosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Unusual rapid progression of TAVI valve degeneration confirmed on PET-CT scan after the valve-in-valve procedure followed by early valve thrombosis
Transcatheter aortic valve implantation (TAVI) has become a standard treatment in severe aortic stenosis (AS).1 However, the major limitations of TAVI remain valve degeneration and thrombosis, which may affect long‑term outcomes.2-4
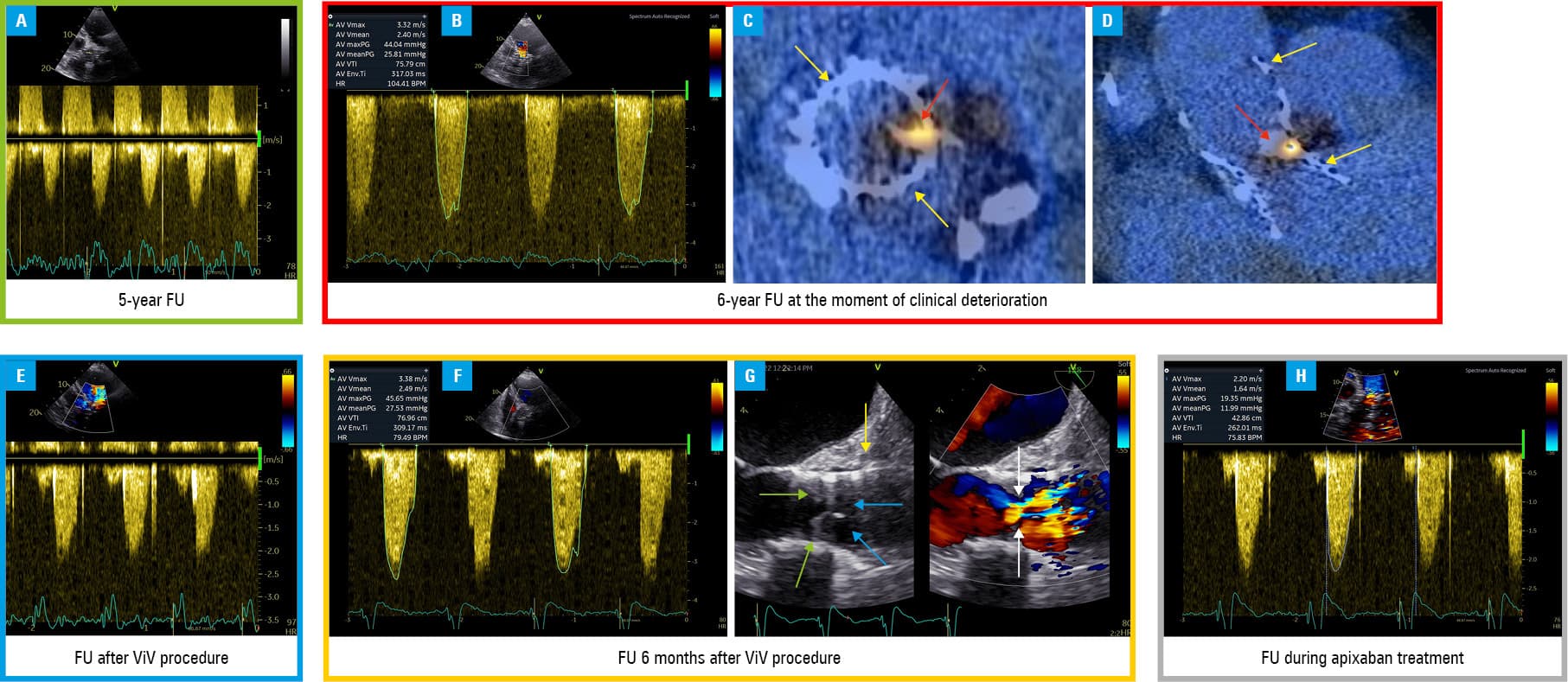
An 80‑year‑old man, 5 years after CoreValve 31 implantation due to severe AS with porcelain aorta, reported exertional dyspnea (New York Heart Association class IV). He had a history of percutaneous coronary intervention in the left main coronary artery, arterial hypertension, pacemaker implantation (complete atrioventricular block after TAVI), and massive obesity (body mass index of 48 kg/m2). Compared with baseline, transthoracic echocardiography (TTE) revealed a decrease in left ventricular ejection fraction (LVEF) from 65% to 20%, a mean transaortic pressure gradient (MTPG) increase from 9 to 26 mm Hg, and a decrease in the effective orifice area (EOA) after TAVI from 1.9 to 0.8 cm2 (Figure 1A and 1B). Transesophageal echocardiography (TEE) revealed leaflet thickening with slight focal changes and 1 immobile leaflet. Because of a relatively fast (12 months) significant gradient increase, valvular thrombosis was suspected. Anticoagulation treatment was introduced. Due to the decrease in LVEF, a control coronary angiography was performed, and a good outcome of the previous procedure was confirmed. Computed tomography of the heart combined with an 18F‑sodium fluoride (18F‑NaF) positron emission tomography computed tomography (PET‑CT) was performed. An increased 18F‑NaF focal uptake within the valve, typical of valve leaflet calcification, was confirmed (Figure 1C and 1D). Thus, severe degenerative TAVI valve dysfunction was diagnosed. The Heart Team referred the patient for an urgent valve‑in‑valve procedure with the brain protection system, and Edwards S3 29 mm valve (Edwards Lifesciences, Irvine, California, United States) was successfully implanted via the transfemoral approach. The control MTPG was 11 mm Hg with EOA of 2 cm2 (Figure 1E). Because of the increased risk of thrombosis due to the valve‑in‑valve procedure and low LVEF, acetylsalicylic acid 75 mg combined with clopidogrel 75 mg daily were introduced. Six months after the procedure, echocardiography revealed an asymptomatic increase in MTPG to 27 mm Hg with EOA reduction to 1.2 cm2, and LVEF of 25% (Figure 1F). On TEE, decreased leaflet mobility due to thrombi was detected (Figure 1G). Apixaban 5 mg twice daily was introduced. As the LVEF remained decreased despite optimal pharmacologic treatment, an implantable cardiac resynchronization therapy defibrillator was implanted. On the follow‑up, MTPG was reduced to 12 mm Hg, with EOA of 1.6 cm2 and LVEF of 40% (Figure 1H).
The standard method for diagnosing TAVI dysfunction during follow‑up is TTE; however, finding out the etiology usually requires expanding imaging diagnostics with TEE or CT. New methods, such as PET‑CT, especially with 18F‑NaF as a calcification marker, may be helpful in detecting TAVI degeneration and differentiating other mechanisms of the valve structural deterioration, including leaflet calcification, leaflet tearing, stent rupture, or stent creep.4 The treatment of choice in patients with TAVI degeneration remains the valve‑in‑valve procedure,5 which, however, may be associated with an increased risk of subsequent valve thrombosis and the need for anticoagulant treatment. At the same time, thrombosis remains a risk factor for embolic events and accelerated valve degeneration.2,3,5
- Huczek Z, Rymuza B, Mazurek M, et al. Temporal trends of transcatheter aortic valve implantation in a high‑volume academic center over 10 years. Kardiol Pol. 2021; 79: 820‑826. | Crossref
- Capodanno D, Petronio AS, Prendergast B, et al. Standardized definitions of structural deterioration and valve failure in assessing long‑term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio‑Thoracic Surgery (EACTS). Eur Heart J. 2017; 38: 3382‑3390. | Crossref
- Sorysz D, Dziewierz A, Bagieński M, et al. Early results of the ongoing Polish Registry of Valve Thrombosis after Transcatheter Aortic Valve Implantation (ZAK‑POLTAVI). Kardiol Pol. 2020; 78: 681‑687. | Crossref
- Kwiecinski J, Tzolos E, Cartlidge TRG, et al. Native aortic valve disease progression and bioprosthetic valve degeneration in patients with transcatheter aortic valve implantation. Circulation. 2021; 144: 1396‑1408. | Crossref
- Kataruka A, Otto CM. Valve durability after transcatheter aortic valve implantation. J Thorac Dis. 2018; 10: S3629‑S3636. | Crossref
ARTICLE INFORMATION