Seroconversion following a booster dose of COVID-19 vaccine in liver transplant recipients: a systematic review and meta-analysis
Key words: COVID-19, immunogenicity, liver transplant recipients, seroconversion rates, vaccine



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Seroconversion following a booster dose of COVID-19 vaccine in liver transplant recipients: a systematic review and meta-analysis
Introduction: Although it is well established that 2 doses of COVID‑19 vaccines are associated with reduced immune responses in liver transplant recipients (LTRs), studies regarding their immunogenicity and tolerability after a booster dose are limited.
Objectives: We aimed to review the available literature data regarding antibody responses and safety of the third dose of COVID‑19 vaccines in LTRs.
Patients and methods: We searched PubMed and Google Scholar for eligible studies. The primary outcome was to compare the rates of seroconversion after the second and third dose of COVID‑19 vaccine in LTRs. This meta‑analysis was performed using a generalized linear mixed model and the Clopper and Pearson method was employed to calculate the 2‑sided CIs.
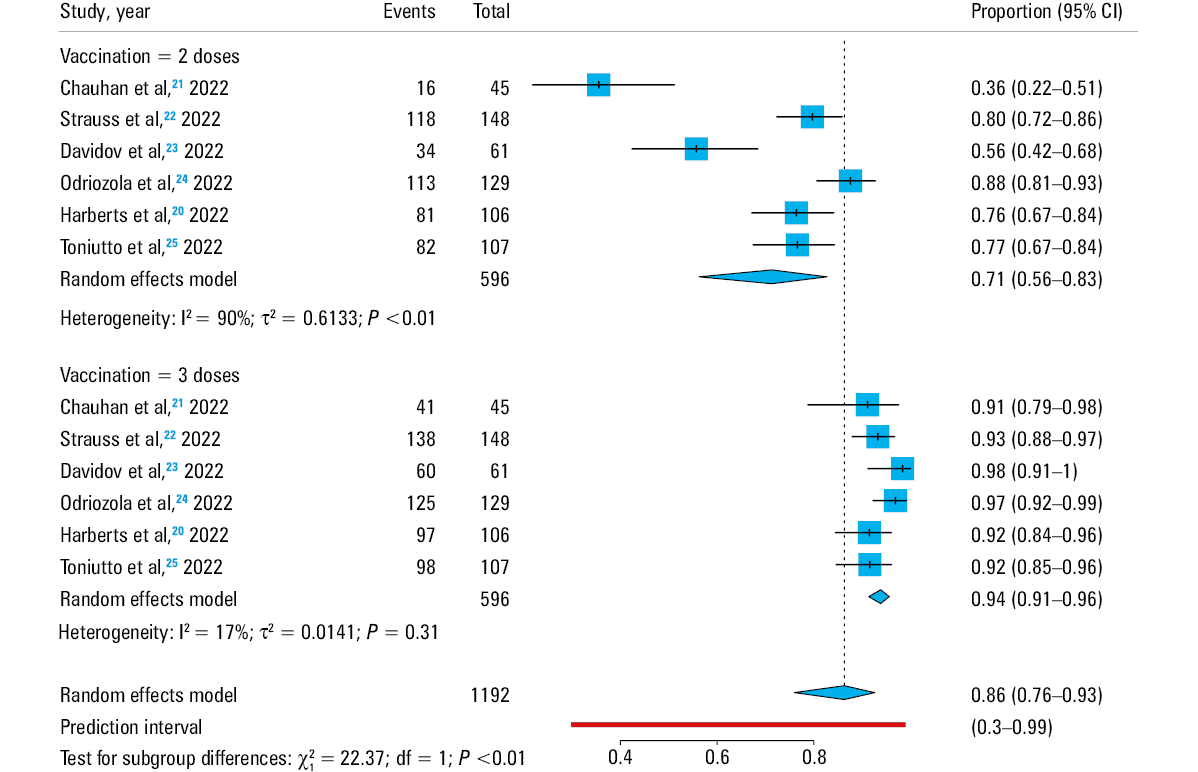
Results: Six prospective studies involving 596 LTRs met the inclusion criteria. The pooled rate of antibody response before the third dose was 71% (95% CI, 56%–83%; heterogeneity, I2 = 90%; P <0.001), while after the third dose it was 94% (95% CI, 91%–96%; heterogeneity, I2 = 17%; P = 0.31). There was no difference in antibody responses after the third dose in relation to the use of calcineurin inhibitors (P = 0.44) or mammalian target of rapamycin inhibitors (P = 0.33), while the pooled rate of antibody responses in the patients on mycophenolate mofetil (MMF) was 88% (95% CI, 83%–92%; heterogeneity, I2 = 0%; P = 0.57). It was significantly lower (P <0.001), as compared with those on MMF‑free immunosuppression (pooled rate, 97%; 95% CI, 95%–98%; heterogeneity, I2 = 30%; P = 0.22). No safety concerns were reported for the booster dose.
Conclusions: Our meta‑analysis demonstrated that the third dose of COVID‑19 vaccines induced adequate humoral and cellular immune responses in LTRs, while MMF remained a negative predictor of immunologic responses.
What's new?
Low immunogenicity response following the second dose of COVID‑19 vaccine in the liver transplant (LT) setting is well established. This meta‑analysis supports the administration of a booster dose of a COVID‑19 vaccine in LT recipients, which is associated with excellent efficacy and very good safety. However, during the vaccination period for the booster dose, mycophenolate mofetil should be reduced or withdrawn temporary if feasible, since its administration is a risk factor for low immune response.
Introduction
Coronavirus disease, caused by SARS‑CoV‑2, has been spreading globally since December 2019, leading to high morbidity and mortality,1 particularly among immunocompromised patients, such as those with solid organ transplantation (SOT), including liver transplant (LT) recipients.2 In addition, several studies have shown that SOT recipients characterized by prolonged viral shedding after SARS‑CoV‑2 infection, pose a risk of mutations and emergence of new variants.3 As a result, health care systems, which have been severely impacted by the COVID‑19 pandemic, have tried to prioritize the development of safe and effective anti–SARS‑CoV‑2 medications and vaccines. The latter have been the most effective means of preventing the virus spread and poor outcome, and both BNT162b2 and mRNA‑1273 vaccines have shown almost excellent efficacy in the general population.4 However, patients receiving immunosuppressive regimens were excluded from the initial licensing clinical trials of COVID‑19 vaccines. In addition, accumulative data have shown lower immunogenic response in SOT recipients, as compared with the general population,5-7 attributable mainly to the use of immunosuppression. A recent systematic review / meta‑analysis of 29 studies and 11 713 recipients of SOT documented reduced seroconversion rates after 2 doses of COVID‑19 vaccine (44.9% [0%–79.1%] seroconversion rate for antispike antibodies and 22.6% [0%–47.5%] for neutralizing antibodies).8 Regarding liver transplant recipients (LTRs), there are robust and sufficient literature data concerning their immune responses after 2 doses of COVID‑19 vaccine, whereas a recent meta‑analysis focused on this setting confirmed lower antibody response rates of LTRs, as compared with healthy controls (HCs), or patients with chronic liver disease (CLD) (risk ratio and 95% CI for LTRs, 0.68 and 0.59–0.77 vs HCs or CLD, 0.96 and 0.9–1.02; P = 0.14).9
Based on these literature findings, indicating lower vaccine seroconversion, a complete immunization schedule with an additional booster dose against COVID‑19 for SOT recipients is recommended by the current guidelines.10,11 The efficacy of this approach in SOT recipients has been recently evaluated in a systematic review / meta‑analysis,12 which confirmed low seroconversion rates following the second dose of COVID‑19 vaccine, but also showed improved immunogenicity after a booster dose (34% vs 66% seropositivity after the second and third dose, respectively). In this meta‑analysis,12 no separate data for LTRs were provided, as the included studies were not focused on LTRs. However, heterogeneity in seroconversion rates among SOT recipients after COVID‑19 vaccination, depending on the type of transplanted organ, is well established,6 indicating the need for studies reporting data separately for each organ recipient group. In fact, only recently, studies including solely LTRs have been published regarding the immunogenicity and tolerability after a booster dose of COVID‑19 vaccine in the LT setting. Therefore, focusing on this knowledge gap, we aimed to review the current available data regarding antibody response of LTRs, as well as the safety profile of a third dose of COVID‑19 vaccine.
Materials and methods
Data sources, study selection, and quality assessment
We searched for studies published in English from December 2019 to August 2022, according to the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses checklist to identify all medical literature about serologic response of LTRs after the third dose of a COVID‑19 vaccine. We also searched the reference lists of relevant papers to identify related papers. The studies were considered eligible if: 1) they included adult LTRs either exclusively or as a subgroup of the whole study population, and 2) provided data for LTRs regarding serological response before and after the third dose of a COVID‑19 vaccine. The studies which did not provide results separately for LTRs were excluded. The search of the published literature was conducted across PubMed and Google Scholar databases using the keywords three doses or third dose or booster or third COVID‑19 vaccine AND solid‑organ transplant recipients or liver transplant recipients AND COVID‑19 vaccine or messenger RNA vaccine or mRNA vaccine or Pfizer or mRNA‑1273 or BNT162b2 or COVID‑19 mRNA vaccine or SARS‑CoV‑2 vaccine. Two reviewers (AG and VL) independently searched for relevant studies, based on the title and abstract of each article, and extracted data using a predefined form. Any disagreement was resolved by the third reviewer (EC). The Newcastle–Ottawa scale was used to assess the quality of the included studies.13
Data extraction
The following data were extracted by 2 independent reviewers (AG and VL): the first author, the country of origin, the type of study, sample size of LTRs, sex, mean or median age, time between LT and vaccination, as well as time between the second and the third dose, the type of vaccine used, the type of test used for evaluation of serological response, the agents of immunosuppression, the number of LTRs seropositive after the second dose, the number of LTRs seropositive after the third dose, the cellular response, and side effects after the third dose.
Study objectives
The primary outcome of interest was to compare the rates of seroconversion after the second and third COVID‑19 vaccine dose, while secondary outcomes included identification of risk factors associated with poor antibody response, as well as evaluation of cellular immunity and vaccine safety after the third dose.
Statistical analysis
This meta‑analysis was performed using a generalized linear mixed model.14 The Clopper and Pearson method was used to calculate the 2‑sided CIs for the single proportions of each study.15 The interstudy variance component (τ2) was estimated with the maximum likelihood method, based on marginal distribution.16 Heterogeneity was quantified using I2, while a random effects or a fixed effect model was applied, depending on the presence or lack of significant heterogeneity across studies, respectively.17 Pooled proportions, 95% CIs, and the prediction intervals were calculated.18 The analysis was conducted with R v4.1.2 software (R Foundation for Statistical Computing, Vienna, Austria), using meta‑packages and metaprop functions.19
Results
In total, there were 6 studies, all prospective (2 from the United States, 3 from Europe [Spain, Germany, and Italy], and 1 from Israel) meeting the inclusion criteria.20-25 The initial search retrieved a total of 7 studies, but 1 of them was excluded because it provided no data regarding serological response after the second dose.26 The main characteristics of the 6 included studies are presented in Tables 1 and 2. A total of 596 LTRs were evaluated. Based on the available data, 373 were men, and 528, 188, 61, and 52 patients were on calcineurin inhibitors (CNIs), mycophenolate mofetil (MMF), steroids, and mammalian target of rapamycin (mTOR) inhibitors respectively.
Study, year | Type of study | Country | Newcastle–Ottawa scale | LTR, n | LT responders, 2nd dose, n | LT responders, 3rd dose, n | Men / men, 3rd dose responders, n | Agea | Time from LT, ya | Time between 2nd and 3rd dose, da | Type of vaccine |
a Data are presented as mean (SD), if available, or median (interquartile range).
Abbreviations: LT, liver transplant; LTR, liver transplant recipient; NA, not available | |||||||||||
Chauhan et al,21 2022 | Prospective | US | 8 | 45 | 16 | 41 | 30/– | 65.2 (7.3) | – | 164 | mRNA (Pfizer / Moderna) or Johnson and Johnson |
Strauss et al,22 2022 | Prospective | US | 7 | 148 | 118 | 138 | 68/
64 | 63 (51–69) | 6 (2–13) | 169 (148–188) | Pfizer‑BioNTech BNT162b2 mRNA or mRNA‑1273, Moderna |
Davidov et al,23 2022 | Prospective | Israel | 7 | 61 | 34 | 60 | 35/34 | 65 (52–70) | 7 (4–16) | NA | Pfizer‑BioNTech BNT162b2 mRNA |
Odriozola et al,24 2022 | Prospective | Spain | 7 | 129 | 113 | 125 | 99/97 | 60.6 (56–28) | 7 (4–12) | 4 mo (133–139) | mRNA‑1273, Moderna |
Harberts et al,20 2022 | Prospective | Germany | 9 | 106 | 81 | 97 | 64/– | – | 8.8 (2.6–14.8) | 157 (127–188) | Pfizer‑BioNTech BNT162b2 mRNA or mRNA‑1273, Moderna |
Toniutto P,25 2022 | Prospective | Italy | 7 | 107 | 82 | 98 | 77/
71 | 67.3 | 91 mo (48–189) | 6 mo (161–169) | Pfizer‑BioNTech BNT162b2 mRNA |
Study, year | Responders / nonresponders on CNIs | Responders / nonresponders on MMF | Responders / nonresponders on mTORi | Type of test used for evaluation of serological response | Safety |
Abbreviations: CNI, calcineurin inhibitor; ELISA, enzyme‑linked immunosorbent assay; Ig, immunoglobulin; MMF, mycopholate mofetil; mTORi, mTOR inhibitor; RBD, receptor binding domain | |||||
Chauhan et al,21 2022 | 30/4 | – | – | Antibodies against receptor binding domain to SARS‑CoV‑2 spike protein using the Roche electrochemiluminescence and Elecsys LabCorp semiquantitative immunoassay | No serious side effects / most commonly pain at the injection site (43%) and fatigue (11%) |
Strauss et al,22 2022 | 116/10 | 37/6 | 24/1 | Roche Elecsys Anti–SARS‑CoV‑2 enzyme immunoassay
or EUROIMMUN EIA | – |
Davidov et al,23 2022 | 60/1 | 17/1 | 7/0 | “In‑house” ELISA against the RBD | Only mild side effects (37% local pain, fatigue) |
Odriozola et al,24 2022 | 113/2 | 29/3 | 9/1 | Anti–SARS‑CoV‑2 S1 antibodies by chemiluminescent microparticle immunoassay (Roche, Mannheim Germany) and the SARS‑CoV‑2 IgG II Quant assay (Abbot, Chicago, Illinois, United States) | – |
Harberts et al,20 2022 | 97/9 | 45/4 | – | DiaSorin LIAISON XL anti–SARS‑CoV‑2 TrimericS IgG ChemiLuminescent ImmunoAssay Roche Elecsys anti–SARS‑CoV‑2 S Ig and ElectroChemiLuminescent ImmunoAssay (anti‑S RBD) | Only mild side effects (60% local side effects, 35% fatigue) |
Toniutto et al,25 2022 | 86/9 | 38/8 | 10/0 | Anti–SARS‑CoV‑2‑N protein (iFlash – Shenzhen Yhlo Biotech Co. Ltd., China) and antispike glycoprotein‑specific IgG RBD antibodies (Roche Elecsys, F. Hoffmann‑La Roche Ltd., Mannheim, Germany) | No safety concerns,
11% local side effects |
The mean time between LT and vaccination was 7.3 (2.5) years, the time between the second and the third dose ranged from 4 to 6 months, and the type of the vaccine was mainly mRNA one (Pfizer‑BioNTech BNT162b2 or 1273 Moderna) in all but 3 LTRs; all 3 LTRs who received a viral vector vaccine as a booster dose were included in the same study.21
Seroconversion rates: humoral immune responses
Antibody seropositivity before and after receiving the third dose of the vaccine ranged between 36%–88% and 91%–98%, respectively (Table 1). The pooled rate of antibody response before the third dose was 71% (95% CI, 56%–83%; heterogeneity, I2 = 90%; P <0.001), while after the third dose it was 94% (95% CI, 91%–96%; heterogeneity, I2 = 17%; P = 0.31), indicating a significant increase (P <0.001) (Figure 1).
Abbreviations: df, degrees of freedom
Cellular immunity to COVID‑19 vaccine
Unfortunately, cellular immunity after COVID‑19 vaccination is poorly investigated in the literature, probably due to the complexity and cost of the laboratory techniques evaluating T‑cell responses. Two studies evaluated cellular response of the LTRs after administration of the third dose of the vaccine. One study reported improved responses after the booster dose,24 while the other study showed that the third dose enhanced the cellular immunity but to a lesser extent than in HCs.20 Specifically, Harberts et al20 assessed the vaccine‑induced SARS‑CoV‑2 spike‑specific T‑cell response in LTRs using a commercial, standardized interferon γ release assay (IGRA, EUROIMMUN), and a sensitive assay measuring cytokine production following in vitro expansion of spike‑specific T cells. The latter showed 72% response rate after the third dose, as compared with 32% after the second dose of the vaccine. In the study by Odriozola et al,24 the assessment of SARS‑CoV‑2 T‑specific response was based on the surface expression of activation‑induced markers after exposure to specific SARS‑CoV‑2 peptide pools, using flow cytometry. The assay was performed in the LTRs who remained seronegative after the third dose of the vaccine, and it was found that 25% of them had vaccine‑specific T‑cell response.24 However, it should be mentioned that in both studies the T‑cell response after the third dose of the vaccine was evaluated in a small number of patients (n = 39 and n = 4, respectively). Thus, more studies are needed in order to clarify this issue.
Risk factors for poor antibody response
Immunosuppressive agents
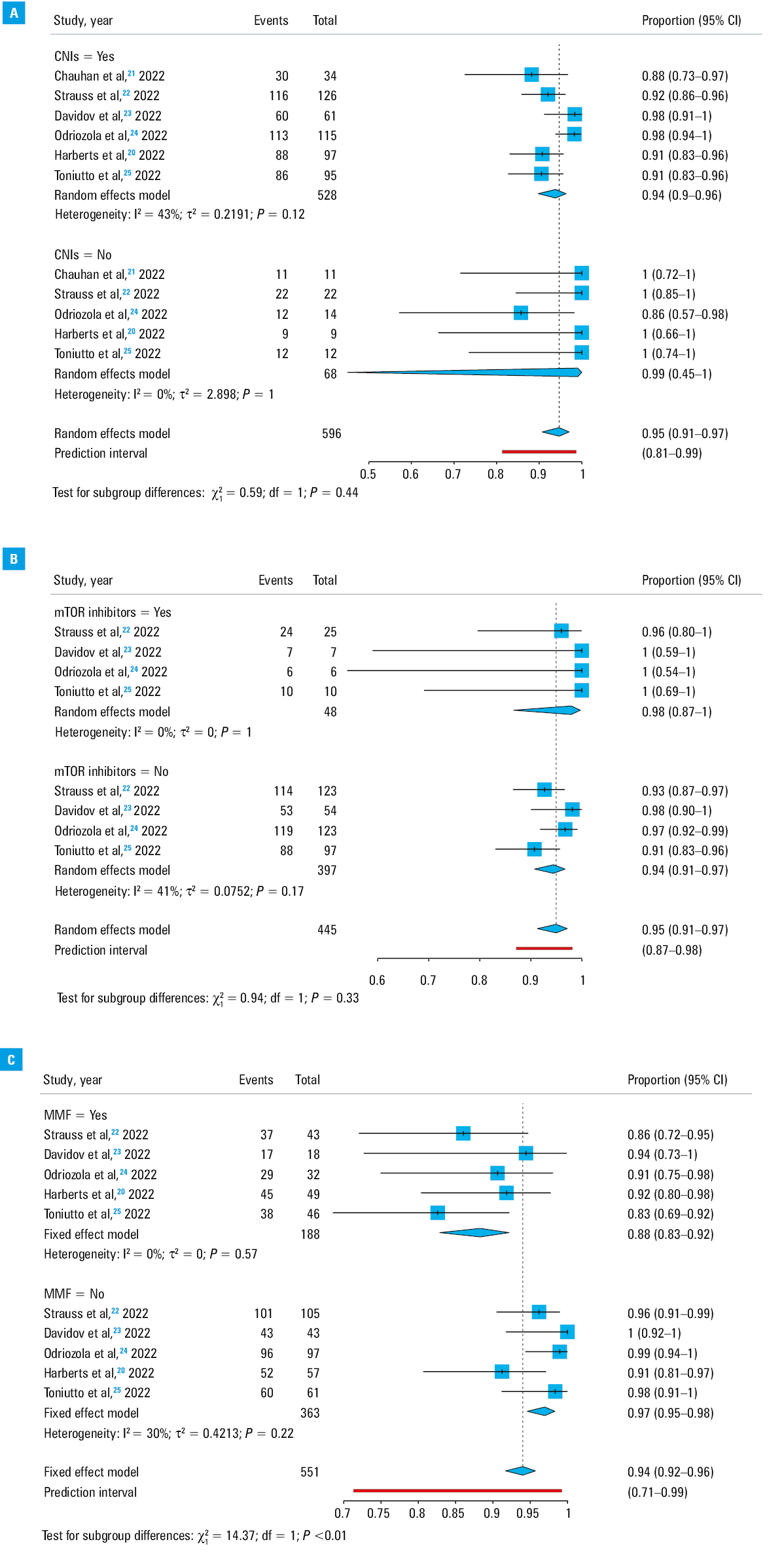
There was no difference in the antibody response in relation to the use of the main immunosuppressive regimens such as CNIs (P = 0.44) or mTOR inhibitors (P = 0.62) (Figure 2A and 2B ), but the serological responses after the third dose were found to differ significantly in relation to the use of MMF. In particular, the pooled rate of the antibody responses in the patients on MMF was 88% (95% CI, 83%–92%; heterogeneity, I2 = 0%; P = 0.57), significantly lower (P <0.001) than in those on MMF‑free immunosuppression (pooled rate, 97%; 95% CI, 95%–98%; heterogeneity, I2 = 30%; P = 0.22) (Figure 2C).
Abbreviations: see Table 2
Other potential risk factors
The difference in the pooled seroconversion rates by sex was not significant (Figure 3A), as 95% (95% CI, 92%–97%) of male and 93% (95% CI, 88%–96%) of female LTRs were seropositive after the third dose (P = 0.34).
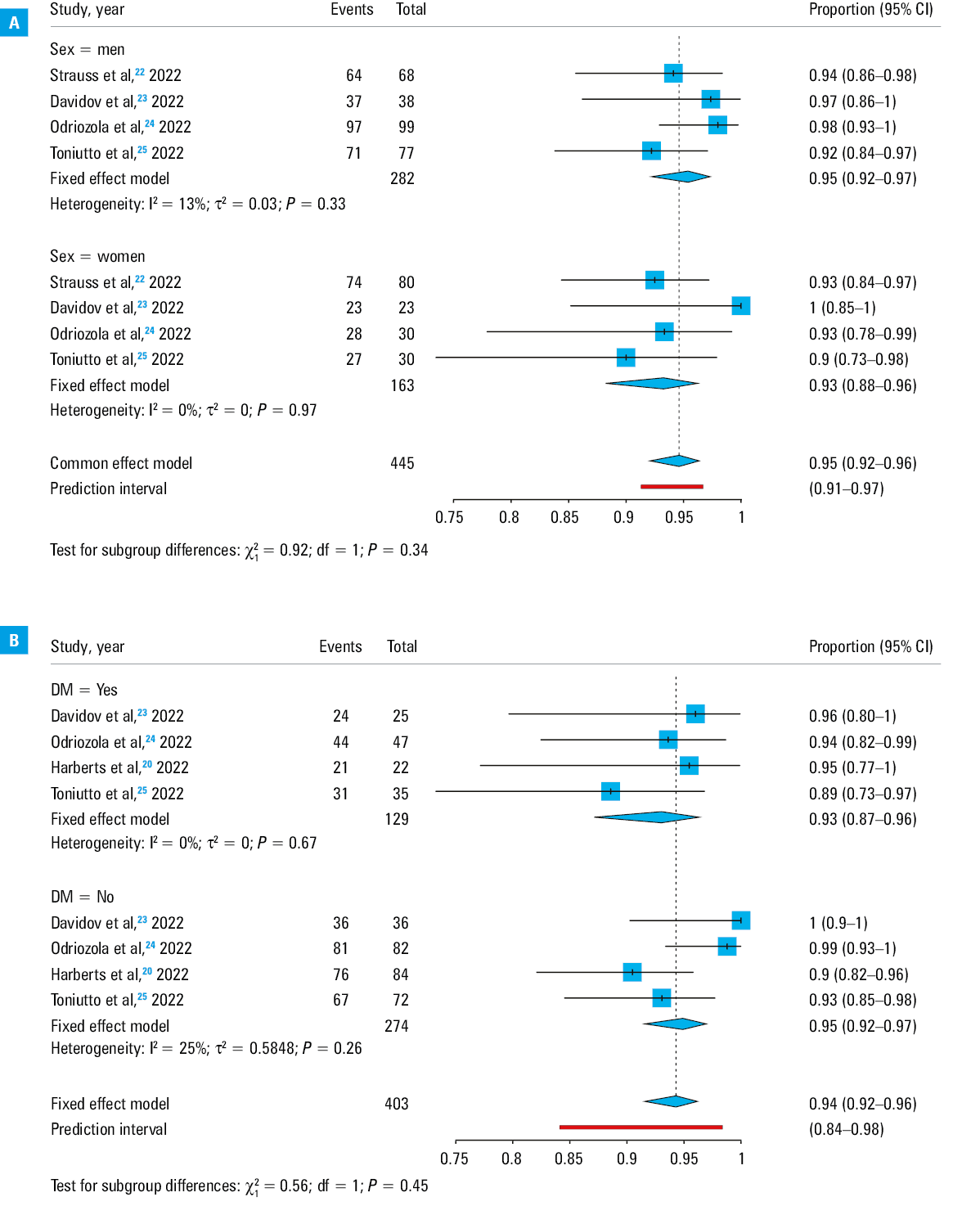
We further compared the seroconversion rates in the patients with and without diabetes mellitus (DM), as it may affect the vaccination response rates. Again, there was no significant difference in relation to the DM status (P = 0.45) (Figure 3B), indicating that DM did not adversely affect immunogenicity.
Safety of the third dose
In total, 4 studies reported data regarding safety of the booster dose, with the most common adverse events being mild, mainly local pain at the injection site in about 38%, and fatigue in about 28% of the LTRs18,19,21,23 (Table 2). Importantly, no graft rejection episodes were reported. For example, in the study by Harberts et al,19 the most frequent side effects were pain or swelling at the injection site, followed by low grade systemic reactions, such as headache or fatigue. Similarly, Chauhan et al,21 as well as Davidov et al,23 reported good tolerability of the booster dose, frequently identifying local adverse reactions and fatigue.
Discussion
Several recent studies have shown a reduced immunogenicity response among SOT recipients after the first and second mRNA vaccine doses for COVID‑19, as compared with the general population,12 which supported the need for the third dose.27-29 In fact, a recent meta‑analysis30 showed that a booster dose of COVID‑19 vaccine results in significant immune response, with a considerable increase in the neutralizing antibodies in the SOT recipients, with good safety profile. However, no separate data regarding LTRs were provided, and the factors associated with poor response in this setting were not evaluated.30 Thus, the current meta‑analysis is the first one that investigated the efficacy and safety of the third dose of a COVID‑19 vaccine in the LT setting. Nevertheless, there are no well established antibody cutoff levels after vaccination against COVID‑19 that provide complete protection against severe forms of the disease. Moreover, there are no literature data to confirm that higher antibody levels after COVID‑19 vaccination are associated with superior protection and more favorable disease outcome.31 Nevertheless, a recent study investigating the impact of prior COVID‑19 vaccination status on the clinical course of SARS‑CoV‑2 infection in SOT recipients showed reduced mortality among already fully vaccinated vs partially vaccinated or unvaccinated patients.32 Another study also showed that partially vaccinated SOT recipients (with 1 or 2 doses of a COVID‑19 vaccine) had similar severity of COVID‑19 to the unvaccinated patients, indicating the importance of the third dose of the COVID‑19 vaccine.33 Thus, adherence to the scheduled vaccinations seems to be crucial in this group of patients.
Our analysis of 6 prospective studies demonstrated that despite low antibody titers after 2 doses of the COVID‑19 vaccine, seropositivity increased significantly after the third dose in the LTRs (from 71% before to 94% after the third dose), which is in agreement with the findings of the recent studies including any SOT recipients.12,30,34 Since it remains unclear whether humoral or cellular immunity offers the main protection against COVID‑19, it is reassuring that both humoral and cellular responses were found to be sufficiently enhanced after the third dose of the vaccine. It should be noted that the existing literature has more often focused on specific neutralizing antibodies, mainly due to difficulties in assessing T‑cell responses, although the latter may be robust and provide adequate protection. Interestingly, available data suggest some coordination between the humoral and cellular immune response to COVID‑19 vaccination, indicating the pivotal role of both types of response against COVID‑19.31,35 In addition, T‑cell responses to COVID‑19 vaccination may offer adequate protection against severe infection and death, although more studies are needed to confirm this.36 In this review, we were not able to perform a proper meta‑analysis on T‑cell responses, since only 2 studies reported relevant data. However, both studies demonstrated sufficient cellular immune responses.20,23
Previous studies and meta‑analyses37-41 have revealed that factors such as age, treatment with MMF or with more than 2 immunosuppressants, the presence of DM, or renal dysfunction (ie, low estimated glomerular filtration rate [eGFR]) were associated with poor immunogenicity after 2 doses of COVID‑19 vaccine in the SOT recipients. However, in a recent meta‑analysis regarding the third dose of COVID‑19 vaccine in the SOT recipients,30 no pooled data were provided regarding this issue. Thus, our meta‑analysis is the first one that assessed the factors that may be potentially associated with seropositivity after the third dose of a COVID‑19 vaccine in LTRs. An interesting observation was the confirmation of MMF use as a risk factor for lower antibody response after the third dose. Thus, it seems that MMF remains a negative predictor of response not only after the second, but also after the third dose of COVID‑19 vaccine in the LT setting. Understanding the mechanism of action of this drug may contribute to enhancement of the vaccine efficacy. It is known that MMF inhibits proliferation of T and B lymphocytes, and thereby suppresses cell‑mediated immune responses and antibody formation.42,43 Thus, although SARS‑CoV‑2 infection may have a generally mild course in the LT setting,44 clinicians may consider a reduction of the daily dose (or [temporary] discontinuation, if feasible) of MMF during the COVID‑19 vaccination period on an individualized basis. The efficacy of this strategy was recently assessed in 19 LTRs who were seronegative or had low antibody titers after 2 doses of the vaccine, but became seropositive and / or increased their antibody titers after MMF withdrawal.45 However, it should be mentioned that although the LTRs have a lower risk of graft rejection after minimizing immunosuppression for a short period of time, as compared with lung or heart transplant recipients,46 this strategy is not recommended by the current guidelines.47 Nevertheless, further studies are needed to reach final conclusions. Fortunately, the use of CNIs or mTOR inhibitors was not found to be associated with poor immune response after the third dose. We further analyzed the impact of sex on immunogenicity after the vaccination, and found no association between the patient sex and vaccine antibody response. We also demonstrated no significant difference in the seroconversion rates of patients with or without DM, as opposed to the meta‑analysis in SOT recipients after the second dose.39 However, the latter observation should not imply complacency concerning vaccination programs for LTRs, as DM patients are known to be at an increased risk for severe COVID‑19.
This is the first meta‑analysis that sought to assess the response of the LTRs after the third dose of COVID‑19 vaccine, but we acknowledge that it has some limitations, including a small number of patients assessed in each study, and a lack of evaluation of other possible risk factors of poor response (such as eGFR) due to missing data. Additionally, although the main studied outcome was immunogenicity to the third dose of the COVID‑19 vaccine, prevention of severe illness after SARS‑CoV‑2 infection elicited by vaccination of LTRs constitutes the outcome of the utmost importance.
In conclusion, based on the aforementioned data concerning mild side effects, as well as the findings on safety published by Efros et al,30 it seems reasonable to support the administration of at least 1, and when indicated, a second booster dose of COVID‑19 vaccine in the LTRs, in an effort to optimize the vaccination efficacy in this specific population in accordance with the current guidelines.48 Finally, as a small proportion of this vulnerable group of patients continues to remain seronegative after the vaccination, future research should focus on the interventions to either improve the immune responses, or to offer pre‑exposure prophylaxis against COVID‑19, for example by using monoclonal antibodies.
- Phan T. Novel coronavirus: from discovery to clinical diagnostics. Infect Genet Evol. 2020; 79: 104211. | Crossref
- Long B, Carius BM, Chavez S, et al. Clinical update on COVID‑19 for the emergency clinician: presentation and evaluation. Am J Emerg Med. 2022; 54: 46‑57. | Crossref
- Dęborska‑Materkowska D, Kamińska D. The immunology of SARS‑CoV‑2 infection and vaccines in solid organ transplant recipients. Viruses. 2021; 13: 1879. | Crossref
- Fiolet T, Kherabi Y, MacDonald CJ, et al. Comparing COVID‑19 vaccines for their characteristics, efficacy and effectiveness against SARS‑CoV‑2 and variants of concern: a narrative review. Clin Microbiol Infect. 2022; 28: 202‑221. | Crossref
- Mehrabi Nejad MM, Moosaie F, Dehghanbanadaki H, et al. Immunogenicity of COVID‑19 mRNA vaccines in immunocompromised patients: a systematic review and meta‑analysis. Eur J Med Res. 2022; 27: 23. | Crossref
ARTICLE INFORMATION